
Abstract
This study investigates how social franchises extend health care in rural areas, thus addressing vast and persistent disparities in health care access. We conducted an inductive study of Unjani, a South African organization that extended primary health services to disadvantaged rural communities through a network of 135 health clinics. Our analysis focused on the process of impact intermediation—the propagation of impact across multiple layers of the franchise network, including franchisees and downstream beneficiaries. To facilitate impact intermediation, the franchisor harmonized the mission of the franchisees with its own mission and integrated community impact among franchisees. Such coordination and monitoring activity exposed franchisees to intermediation problems in the form of mission conflict and impact divergence. Our analysis reveals how Unjani nurtured network stewardship that afforded the franchisee nurses with greater support, autonomy, and ownership, thus overcoming intermediation problems in their pursuit of shared communal responsibilities to extend health care to rural communities.
Keywords
For he who has health has hope; and he who has hope has everything.
More than 400 million people in the developing world lack access to primary health services; consequently, preventable diseases such as tuberculosis and malaria contribute to 90% of mortalities in these countries (Vakili & McGahan, 2016). The World Health Organization (WHO, 2019) estimates that reducing these health inequities by extending primary health care interventions across low- and middle-income countries could save up to 60 million lives by 2030. The imperative for “good health and well-being,” which is one of the United Nations’ 17 Sustainable Development Goals, became crystal-clear when COVID-19 struck in late 2019 (WHO, 2019). More than 81% of the 14.9 million pandemic-induced deaths globally by the end of 2021 occurred in low- and middle-income countries that lacked robust health infrastructure and access to vaccines (Taylor, 2022). The disproportionate health and economic effects of the pandemic on the poor have heightened the moral urgency of ensuring equitable access to primary health care services globally (Dorado et al., 2022; Vakili & McGahan, 2016).
A chorus of for-profit and non-profit organizations have started to experiment with novel means of organizing to bridge these persistent inequalities in health care access (Park et al., 2022). Social franchising represents an innovative organizational form for extending health care services in developing regions, where public health care services suffer from mal-administration, human capital shortages, and resource constraints (Littlewood & Holt, 2018; Vickers et al., 2017). Social franchising is an adaptation of commercial franchising in which a franchisor who has developed a successful and proven social business concept works with franchisees to extend social benefits to a larger number of people (Iddy et al., 2022; Volery & Hackl, 2010). This model facilitates rapid scaling by enabling the franchisee and the franchisor to pool resources and know-how, thus sharing market risk that would slow down growth (Asemota & Chahine, 2017; Tracey & Jarvis, 2007).
The rapid diffusion of social franchises in Africa and other developing regions points to their unique ability to facilitate the creation of economic and social value for marginalized communities (Asemota & Chahine, 2017; McKague et al., 2014). Nonetheless, how social franchises can effectively scale their social impact is not fully understood, and studies have offered conflicting evidence on their ability to extend health care services to disadvantaged communities (Nguyen & Dey, 2023; Nijmeijer et al., 2014). On one hand, high agency costs associated with the dual goals of social franchises—profit and impact—can make it difficult to achieve goal alignment, leading to conflict, instability, and eventual failure (Tracey & Jarvis, 2007). At the same time, recent research suggests that social franchises could mitigate these challenges by developing mission-driven identities and decentralized governance structures (Giudici et al., 2020). Until now, however, researchers have not explicitly examined one of the unique challenges of health care social franchises: the need to create impact both for the health care service providers (i.e., the nurses running the clinics) and their patients (downstream beneficiaries). This is an important omission because many social franchises engage in impact intermediation, which we define as the propagation of impact across multiple layers of the franchise network that includes the franchisees and downstream beneficiaries (Lawson-Lartego & Mathiassen, 2021; Park et al., 2022). We refer to these as “intermediated social franchises” to differentiate them from micro-franchises in which the creation of downstream impact is not a key priority. The challenge in intermediated social franchises is hence the need to grow while creating significant impact both for the nurses operating franchisee clinics and their downstream health care users (Kistruck et al., 2011). This study seeks to improve current understanding on this topic by addressing the following research question: How do health care social franchises operate effectively to create social impact for disadvantaged rural communities? More specifically, what enables social franchises to overcome agency problems as they seek to extend community health care and create social impact for all beneficiaries?
To answer this question, we conducted a close-up investigation of Unjani Clinic, a South African social franchise that established a network of more than 135 primary health care clinics in rural parts of the country. Unjani’s clinics are operated by professional Black nurses, who strive to extend access to affordable and reliable primary health care to low-income rural communities. Like other intermediated social franchises, Unjani faces the challenge of facilitating impact propagation to ensure the creation of social and economic benefits both for its franchisees and their downstream beneficiaries. The case, therefore, represents a unique but poorly understood phenomenon that warrants deep, qualitative investigation (Gehman et al., 2018).
Given the exploratory nature of our study, we employed an inductive research methodology (Glaser & Strauss, 1967) following the Gioia methodology that provides a systematic guide for identifying deeper structures from qualitative data, with the eventual goal of developing a grounded model (Gioia et al., 2013). Our analysis followed a rigorous and iterative coding process that involved moving between raw data and theory (Locke et al., 2022). The process started with an initial open coding from the raw data, followed by axial coding, before developing aggregate dimensions to explore relationships between key constructs (Saldaña, 2021). The results are developed into a grounded model that depicts a process of impact intermediation in health care social franchises.
The results revealed that the franchisor’s efforts to harmonize and integrate social impact throughout the network gave rise to intermediation problems in the form of mission conflict and impact divergence. These intermediation problems are agency costs, borne mostly by the franchisee nurses, that arise from the franchisor’s need to monitor and coordinate financial and social impact throughout the franchise network. We find that Unjani was able to overcome intermediation problems by nurturing a culture of network stewardship that provided the franchisee nurses with stronger support, autonomy, and ownership, enabling them to create greater impact for patients from disadvantaged rural communities. Integrating stewardship theory (Bacq & Eddleston, 2018; Davis et al., 1997) and agency theory (Jensen, 1986), we propose the concept of network stewardship, which we define as a set of broadly shared values and practices that foster network cohesion and facilitate the pursuit of shared communal responsibilities. The concept of network stewardship uniquely explains how network organizations such as social franchises can overcome agency costs that arise in their pursuit of social and economic objectives.
The study contributes to the literature by unpacking how new organizational forms such as social franchises contribute toward addressing grand challenges (Giudici et al., 2020; Tracey & Jarvis, 2007), particularly the grand health care challenge of extending primary care to vulnerable populations in developing regions (Hefner & Nembhard, 2021). The study extends existing research into social franchising by introducing a grounded model that explicates the process of impact propagation in intermediated social franchises that address inequalities in health care access. Furthermore, the results reveal how agency and stewardship theories can be integrated to generate unique insights on the pursuit of organizational strategies that combine economic and non-economic goals (Bacq & Eddleston, 2018). Overall, the results shed new light on the role of new organizational forms in extending primary health care to disadvantaged communities in developing regions.
Theoretical Background
Inequality in Primary Health Care Access in South Africa
The WHO (2013) defines health inequalities as “avoidable inequalities in health between groups of people within countries and between countries”. In South Africa, which enjoys the unenviable title of the world’s most unequal country (The World Bank, 2023), vast health inequalities inherited from the country’s Apartheid era have led to unjust health outcomes that diverge across people with different socioeconomic status and race/ethnicity (Hussey et al., 2021). The country has the highest number of people living with HIV in the world; approximately 20% of the adult population is HIV positive (Bulled & Singer, 2020). Furthermore, the country ranks fourth globally in the number of tuberculosis infections per capita, which has become the leading underlying natural cause of death (Schröder et al., 2021). The arrival of the COVID-19 pandemic on top of these epidemics has disrupted the functioning of the country’s overburdened health care system, further exacerbating economic and health disparities across different social groups (Eike et al., 2022; Hussey et al., 2021).
South Africa’s health care system suffers from complex challenges that range from shortage of critical resources to poor accessibility (Dookie & Singh, 2012). Poor policy coordination that distorts incentive structures creates a wide variation in staffing levels between facilities, leading to inefficient use of professional staff (Daviaud & Chopra, 2008). These struggles have led to a public health care system that chronically suffers from extreme overcrowding and long waiting times. South Africa’s challenges are emblematic of the difficulties elsewhere in the African continent, which has only 3% of the world’s health workers and less than 1% of the world’s health expenditure despite contributing to 25% of the global disease burden (Mash et al., 2018; Schröder et al., 2021). The onslaught of recent health crises—from tuberculosis to HIV/AIDS and COVID-19—has amplified the urgent need for creating equitable access to primary health care (Benatar et al., 2018). In Africa and other developing regions, there is an evident need to improve health care access in rural areas that, compared with urban areas, suffer from low levels of life expectancy and poor health conditions (Strasser et al., 2016). In the face of a dysfunctional public health care system, local and international actors are turning to innovative approaches for health care that combine entrepreneurial dynamism and social impact creation (Vakili & McGahan, 2016). Among these, social franchising promises to offer the combined benefit of empowering health care professionals from disadvantaged backgrounds and extending health care to remote areas that are typically neglected by existing providers.
How Health Care Social Franchises Create Impact for Disadvantaged Rural Communities
Social franchising is an adaptation of commercial franchising that is increasingly used to create employment opportunities and extend essential services, especially in developing regions. While social franchising shares many similarities with commercial franchising (Table S1 in the Supplementary Material), its distinguishing feature is its focus on social impact (also called social value) rather than mere pursuit of financial profit (Giudici et al., 2020; Kistruck et al., 2011). The literature identifies two broad models of social franchising. The first model, called micro-franchising, involves the use of franchising to generate social benefits to disadvantaged, low-income individuals (franchisees) by creating job opportunities to them. As the micro-franchisees in this model typically come from disadvantaged groups and lack capabilities, the micro-franchisor often does not require them to contribute their own capital or to pay royalties. In the second model of social franchising, the franchisor and the franchisee work in tandem to address an important social problem, such as the provision of primary health care to disadvantaged and rural communities (Asemota & Chahine, 2017; Iddy et al., 2022). We refer to these as intermediated social franchises, which we define as social franchises that seek to provide social impact across multiple layers of beneficiaries in the franchise network, including the franchisees (e.g., the nurses and their assistants) and downstream beneficiaries (e.g., patients and communities at large). To create social impact for downstream beneficiaries, intermediated social franchises facilitate knowledge transfer to the franchisees by providing training, building their managerial expertise, and strengthening their operational efficiency (Cumberland & Litalien, 2018; Iddy et al., 2022).
Intermediated franchises are thus a complex form of social franchise where the franchisee is both a beneficiary and a means for reaching other beneficiaries (Asemota & Chahine, 2017; Lawson-Lartego & Mathiassen, 2021). The franchisees are expected to leverage their local knowledge and social networks, and to abide by mutually beneficial performance metrics, both along social and commercial fronts. For example, Impact Hub is an intermediated social franchise that facilitates the incubation and growth of impact-driven startups with the eventual aim of creating impact for their (future) employees and customers (Giudici et al., 2020). In intermediated social franchises in health care, social impact creation entails the provision of economic and social benefits to the franchisee nurses and the provision of affordable health care services to disadvantaged communities. 1 Although health care social franchises are becoming widespread in Africa and other developing regions (Asemota & Chahine, 2017; Mohiuddin & Yasin, 2023), their ability to improve health care access among the poorest and the most disadvantaged is still debated (Mumtaz, 2018; Nijmeijer et al., 2014). This is in part because replicating standardized clinics could be ineffective to address the needs of communities that suffer from deep, structural problems (McKague et al., 2014). Moreover, as discussed below, the presence of multiple layers of beneficiaries in intermediated social franchises creates additional agency problems.
Agency Problems in Social Franchises
Agency theory has been widely used to understand franchise performance because it sheds light on the system of incentives that influence the relationship between the principal (the franchisor) and the agent (the franchisee) (Jensen, 1986). The theory, for example, explains why franchising becomes a preferred scaling strategy over direct ownership, where employee-managers who work for a fixed salary might have a greater incentive to withhold effort (Chirico et al., 2011; Perryman & Combs, 2012). The agency cost of monitoring employee-managers to reduce shirking becomes high when businesses have a global scope and/or are geographically dispersed, making franchising a less costly and more profitable growth strategy (Combs et al., 2011). Agency theory also sheds light on the kinds of agency problems that arise both in commercial and social franchises. The inability of the principal to devise contracts that specify all potential future scenarios creates two types of agency risks: adverse selection and moral hazard. Adverse selection arises when a franchising agreement attracts franchisees whose interests do not align with the interests of the franchisor, and moral hazard happens when franchisees engage in opportunistic behavior at the expense of the franchisor. An example of opportunism is the freeriding problem, where the franchisees cut costs to increase outlet profit at the expense of the franchisor’s brand name and reputation (Perryman & Combs, 2012). These agency problems can be partly redressed through incentive structures that align the interests of the franchisor and franchisees and through monitoring programs that ensure the franchisees’ compliance. However, incentive and monitoring systems are neither foolproof nor inexpensive, especially in developing countries where transaction costs are high and formal contracts are poorly enforced (Lashitew et al., 2022; Volery & Hackl, 2010).
In intermediated social franchises, the need to coordinate economic and social impact across multiple network members creates additional agency costs (Tracey & Jarvis, 2007). Agency theory, with its view of participants as rational and self-interested actors, would suggest overcoming these challenges by refining selection practices, monitoring processes, and incentive structures. However, participants of social franchise networks, especially in health care, are likely to be motivated by non-economic, other-regarding values, such as care and well-being. Managers could thus nurture social capital and network relationships to build trust and align the interests of diverse stakeholders in lieu of stringent monitoring systems that would further increase agency costs and suppress innovation (Bacq & Eddleston, 2018; Chirico et al., 2011; Lawson-Lartego & Mathiassen, 2021). The presence of social objectives in social franchising thus warrants combining multiple theoretical traditions to capture the interaction between rational, extrinsic motives and relational, intrinsic ones. For this reason, we draw on stewardship theory, which was advanced as an alternative, relational approach for understanding principal–agent relationships (Bacq & Eddleston, 2018; Davis et al., 1997; Jones et al., 2007). Stewardship theory recognizes that human behavior can be governed by collective, rather than merely individualist, motives that may have an intrinsic, relational element (Davis et al., 1997). Indeed, stewardship entails placing the “the long-term best interests of a group ahead of personal goals that serve an individual’s self-interests” (Hernandez, 2008, p. 122). Combining agency and stewardship theories is hence highly suitable for our goal of understanding how social franchises coordinate diverse network members to achieve common social and economic objectives.
Research Methodology
This study provides a close-up investigation of Unjani, a South African non-profit organization that has created a network of more than 135 primary health care clinics through a social franchising model. Unjani seeks to improve access to primary health care in South Africa by providing a competitive alternative to the public health care system that is known for its inefficiency and unreliable service quality. By creating a network of clinics owned and operated by professional South African nurses, Unjani extends affordable and reliable primary health care to low-income communities. South Africa’s persistent inequalities in health care access make it an ideal setting for investigating how social franchises can extend primary care to disadvantaged rural communities.
The Case of Unjani Clinic
History and Operational Model
Unjani Clinic was initiated as a pilot initiative to extend primary health care to corporate employees. In 2011, RTT Ltd, South Africa’s largest private logistics company, kickstarted Unjani Clinic to help improve health care access to its 7,000 employees. The goal was to provide affordable primary health care services near RTT warehouses through a chain of small clinic-in-boxes (see Figures S1 and S2 in the Supplementary Material), while also providing full-time jobs to qualified nurses. In 2013, when RTT was acquired by Imperial Group, Unjani was reorganized as an autonomous non-profit corporation. At the time, Unjani operated a network of 15 clinics built in three different formats targeting rural, semi-rural, and peri-urban areas. Unjani currently has its own board of directors and enjoys significant operational autonomy despite its close relationship with the Imperial Group, which continues to cover parts of its financing needs.
Unjani provides technical and financial support for local nurses operating its network of clinics for a period of 5 years, upon which they are expected to “graduate” and become autonomous. The full cost of supporting a clinic for 5 years is estimated to be $1.1 million Rand (around $60,000 USD), 80% of which goes to cover the cost of constructing, installing, and furnishing the facilities. Unjani finances these expenses through donations it collects from corporations, who benefit from tax deductions for their contributions thanks to Unjani’s non-profit status. 2
Unjani Clinic shares a similar business model as other social franchises that provide health care and other social services. Like other social franchises, Unjani Clinic relies on blended finance that includes income from charitable donations and service fees from franchisees (Kistruck et al., 2011; Lawson-Lartego & Mathiassen, 2021). The balance between commercial and charitable income sources diverges widely among different franchises, depending on the ability of the social franchisees to make financial contributions to the franchisor, either as initial capital or as franchise fees. Donor-funded franchisors such as Unjani typically select disadvantaged and low-income individuals as their franchisees and thus do not collect royalties other than service contributions for collective expenses (e.g., advertising fees). On the other hand, for-profit social franchisors, such as the Impact Hub Company, finance themselves through franchise fees (Anderson & Lent, 2019; Lawson-Lartego & Mathiassen, 2021). Regardless of their income sources, all intermediated social franchises contend with the challenge of propagating social impact across multiple layers of the franchise network, which makes Unjani Clinic a highly relevant case for understanding intermediation problems in social franchising.
Social Impact in Unjani Clinic
As of 2022, Unjani has established 135 primary health clinics that served a cumulative of 3.5 million patient visits (Figure 1). The organization sought to achieve four kinds of impact. First, Unjani aimed to empower Black women and reduce racial inequalities by providing them with an opportunity to operate their own clinics. For this reason, Unjani employed as franchisees Black professional nurses who suffered from educational and employment discrimination during South Africa’s Apartheid era. This is apparent from its mission statement, which affirms Unjani’s commitment to “empowering Black women, improving healthcare quality and access, and creating employment in our communities.” Second, Unjani seeks to extend access to affordable health care to low-income, rural communities in South Africa. This is apparent from the fact that the vast majority (88%) of Unjani patients came from rural and semi-rural areas (Figure S3 in the Supplementary Material). The largest share of Unjani’s clinics (113 as of 2022) is also located in rural and semi-rural areas although urban clinics have on average far more patients than rural ones (834 vs. 384 patients per month) (Figures S4 and S5 in the Supplementary Material). The average number of patients per month in rural areas is well above what clinics need to break even (250 per month), highlighting that, on average, Unjani’s clinics operate profitably. Unjani also fixes the maximum price that franchisee clinics can charge for their services to ensure that their services are affordable to low-income users.
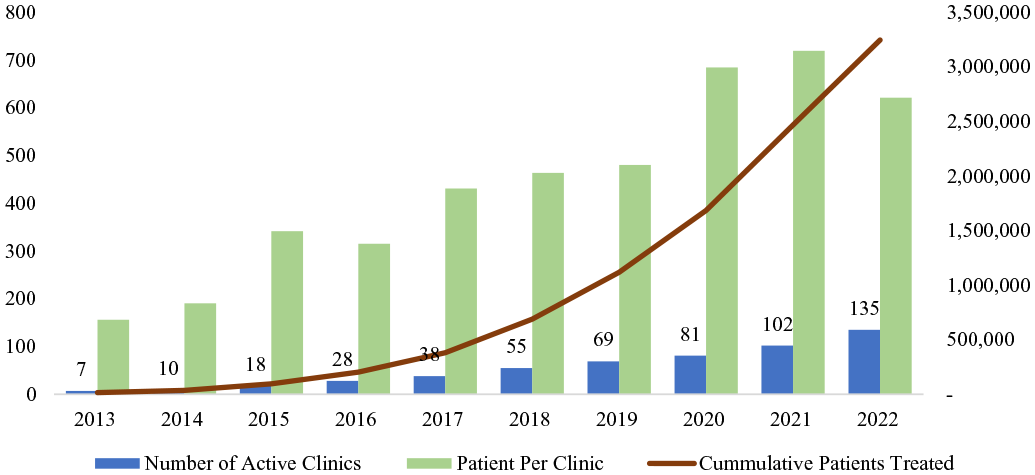
Trends in Number of Active Clinics, Average Patients per Clinic, and Cumulative Number of Patients.
Third, Unjani sought to reduce the work burden of South Africa’s overcrowded public health system. South Africa’s primary health care system is dominated by the public sector, which serves 84% of the population despite employing only 35% of the doctors in the country (Benatar et al., 2018). Moreover, free health care means limited availability of funding for public clinics, which contributes to poor service quality. Unjani’s goal is to serve 10 to 12 million South Africans who could afford to pay for health care services but end up congesting the public health care system because of a lack of affordable alternatives. Finally, Unjani aspired to improve community well-being by adopting a broad conception of health. This meant, among other things, emphasizing protective health (e.g., nutrition and hygiene) and other aspects of community well-being (e.g., over-drinking and mental health) that are not typically prioritized by public health care institutions. The purpose of our analysis is to understand the factors that enabled Unjani to successfully extend primary health care to rural areas of South Africa and create social impact for multiple layers of beneficiaries.
Data Collection and Analysis
Data Collection
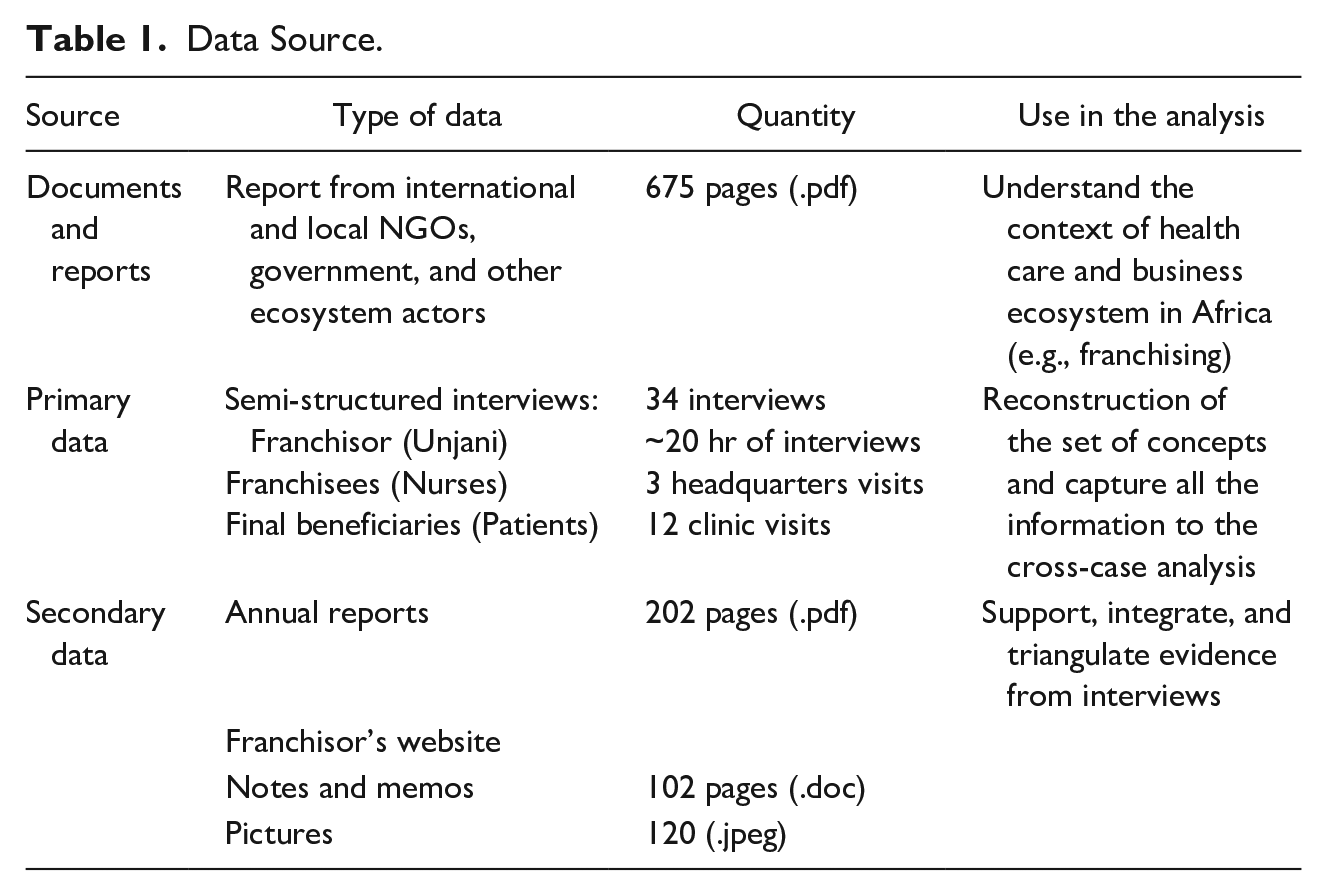
Data collection was preceded by desk research, in which we studied available reports on health care access in Africa. Examination of reports and online resources enabled us to engage with the context of our case study by exploring the challenges of health care access in developing regions (see Table S3 in the Supplementary Material). After this initial assessment, we commenced developing an interview protocol that included questions for semi-structured interviews, which guaranteed a level of flexibility during the interview while avoiding preordained understandings on the topics of interview (Gioia et al., 2013). We covered various topics relevant to the operations of Unjani, its network management strategies, its relationships with local communities, and the coordination of various activities across the network. The first phase of data collection included six interviews with the top management of Unjani addressing the business model of Unjani, its growth path, and challenges in creating impact. In the second phase, we interviewed the franchisee nurses and their assistants (13 interviews) to get a deeper understanding of the problems they experienced in their relationship with Unjani. The third phase involved interviews with downstream beneficiaries (16 patients from the rural communities) with the aim of acquiring a better understanding of their health care experience. In total, we conducted 34 semi-structured interviews.
Through these interviews, we acquired granular understanding of the operations of the clinics, the activities of nurses, their relationships with local communities, and the role of Unjani in developing and managing the network. Moreover, news articles, pictures, and videos were used to complement and corroborate primary data collected through the fieldwork.
Table 1 describes our different sources of data, and Table 2 provides a detailed description of our interviews. Table S3 in the Supplementary Material provides a list of secondary data sources.
Data Source.
Interview Data.
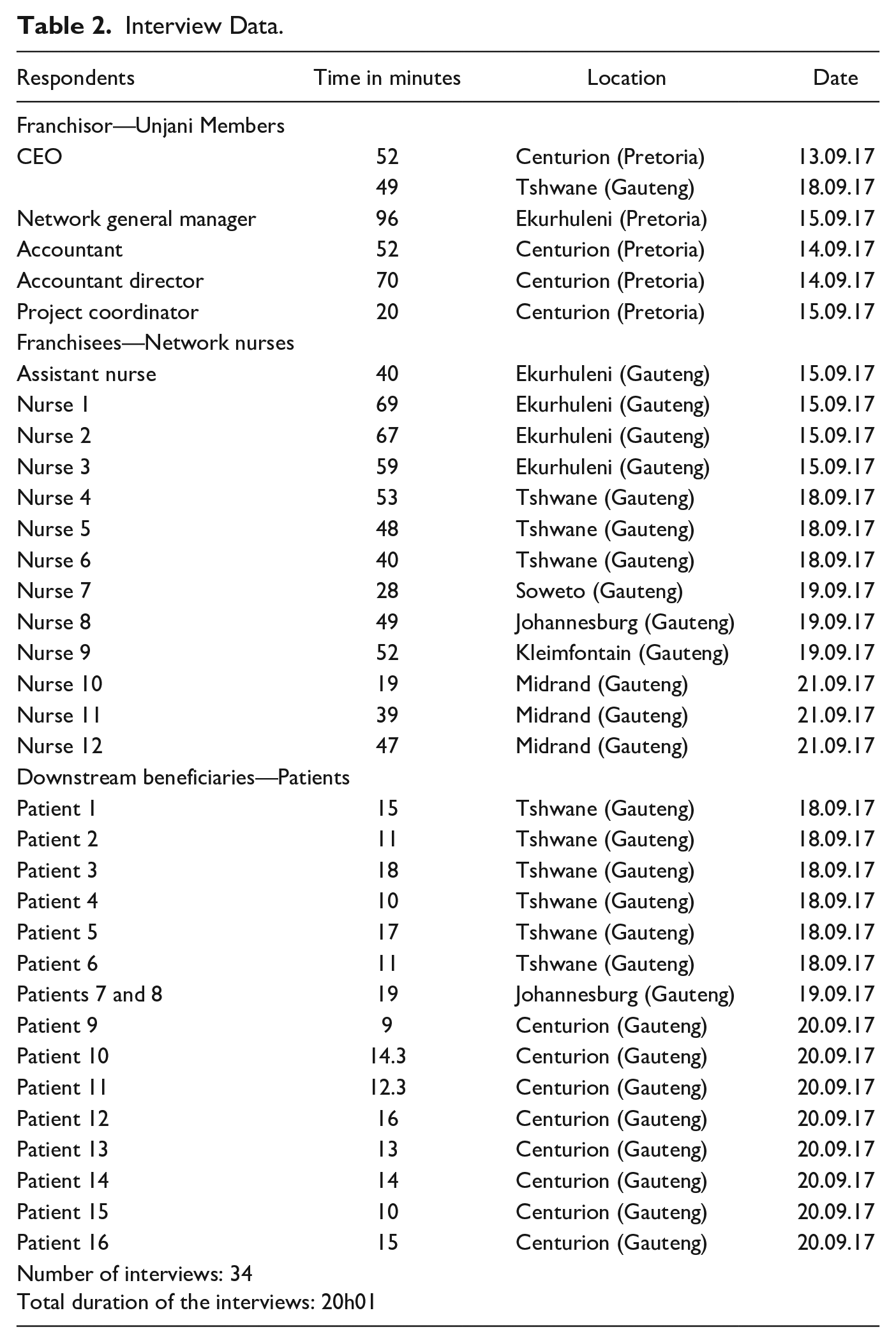
Primary data were collected over a course of 2 months in 2017. The first author spent 3 weeks doing fieldwork, which included conducting field observation at Unjani’s head office and its clinics throughout South Africa. This allowed for an immersive experience of data collection and preliminary analysis through joint reflections with respondents (see Gehman et al., 2018). Among other things, the researcher attended Unjani’s meetings and visited franchisee clinics to understand their operations, their decision-making processes, and their relationships with the franchisees, the patients, and other community members. This was done by adopting best practices of qualitative research to limit social desirability bias (Bergen & Labonté, 2020; Locke et al., 2022). Particularly, we have pre-tested our data collection protocol and interview questions, which enabled us to improve the framing of many questions to avoid social desirability bias. Several interviews were conducted with two or more participants, which helped reduce measurement error by cross-checking responses. This process of actively working on the field and “getting the hands dirty” was essential to ensure a rigorous and empirically grounded qualitative data collection and analysis (Gioia et al., 2013, p. 19). Furthermore, attending meetings and observing the franchisee clinics provided sufficient understanding of the social and organizational dynamics, which reduced the likelihood of being significantly misled during the interviews and subsequent data analysis.
Data Analysis
Given the nature of the research questions, data analysis followed an iterative, inductive approach (Gioia et al., 2013; Glaser & Strauss, 1967), with the aim of understanding how Unjani propagated impact in its franchise network to extend affordable health care services to its rural communities. This analysis was done following the Gioia and colleagues (2013) methodology, which provided a systematic and rigorous approach for iteratively analyzing the raw data to develop high-level theoretical constructs. Data analysis proceeded in three steps.
In the first stage, we used an open coding procedure (Gehman et al., 2018) that captured key bottom-up processes from the lived experiences and actions of respondents (Locke et al., 2022). This procedure enabled us to break down the data and identify instances of observation and comparison (Rindova & Kotha, 2001). Open coding helped identify key snippets from the interviews, which were used for developing initial categories using qualitative coding and analytical induction (Brown et al., 2015). Specifically, we reassembled the data by identifying key words of actions and perceptions surrounding the activities of the franchisor and franchisees. For example, we coded the various activities of the franchisor in selecting, promoting, training, and monitoring the franchisee nurses. Similarly, we started to identify problems experienced by the nurses related to lack of motivation, dejection, and prioritization of financial benefits. Initially, we captured these as general problems, but through consultation with the literature and data triangulation, we classified those problems into broader categories (e.g., Mission conflict and Impact divergence). Thus, we aggregated patterns and common themes together by organizing the raw data around first-order codes and second-order themes with similar meanings (Locke et al., 2022; Rindova & Kotha, 2001). After one of the authors coded all the interviews, the other authors followed the same steps and coded the interview transcripts. After the open coding process was done, we conducted an inter-rater analysis to evaluate data consistency and reliability among the initial first-order codes (Saldaña, 2021). We then went back to the literature and started to identify possible linkages between the literature and our emerging codes (e.g., concerning the agency problems with nurses and the stewardship literature). We triangulated data from multiple sources, including internal memos and reports, archival data, annual statistics, and interviews from diverse sources, which improved data reliability and reduced social desirability bias (Bergen & Labonté, 2020).
In the second stage, we systematically compared the first-order categories in light of the relevant literature and grouped them into larger categories based on their similarities and differences. This step of axial coding was done iteratively, going back-and-forth between reading the transcripts, comparing codes, and consulting the literature. This process also enabled us to refine many of our original codes, ensuring greater consistency of coding, leading to an inter-rater reliability of 78%. We then proceeded to collapse the second-order themes to develop aggregate dimensions, which constituted our core theoretical constructs. For example, we aggregated the second-order themes “community-centered selection of franchisees” and “promoting identification with the franchisor mission” into a broader aggregate theme called “harmonizing franchisees and franchisor mission,” because we recognized they were both motivated by the purpose of harmonizing the mission of the franchisor and that of the franchisees. Figure 2 shows the data structure that emerged from our inductive data analysis.
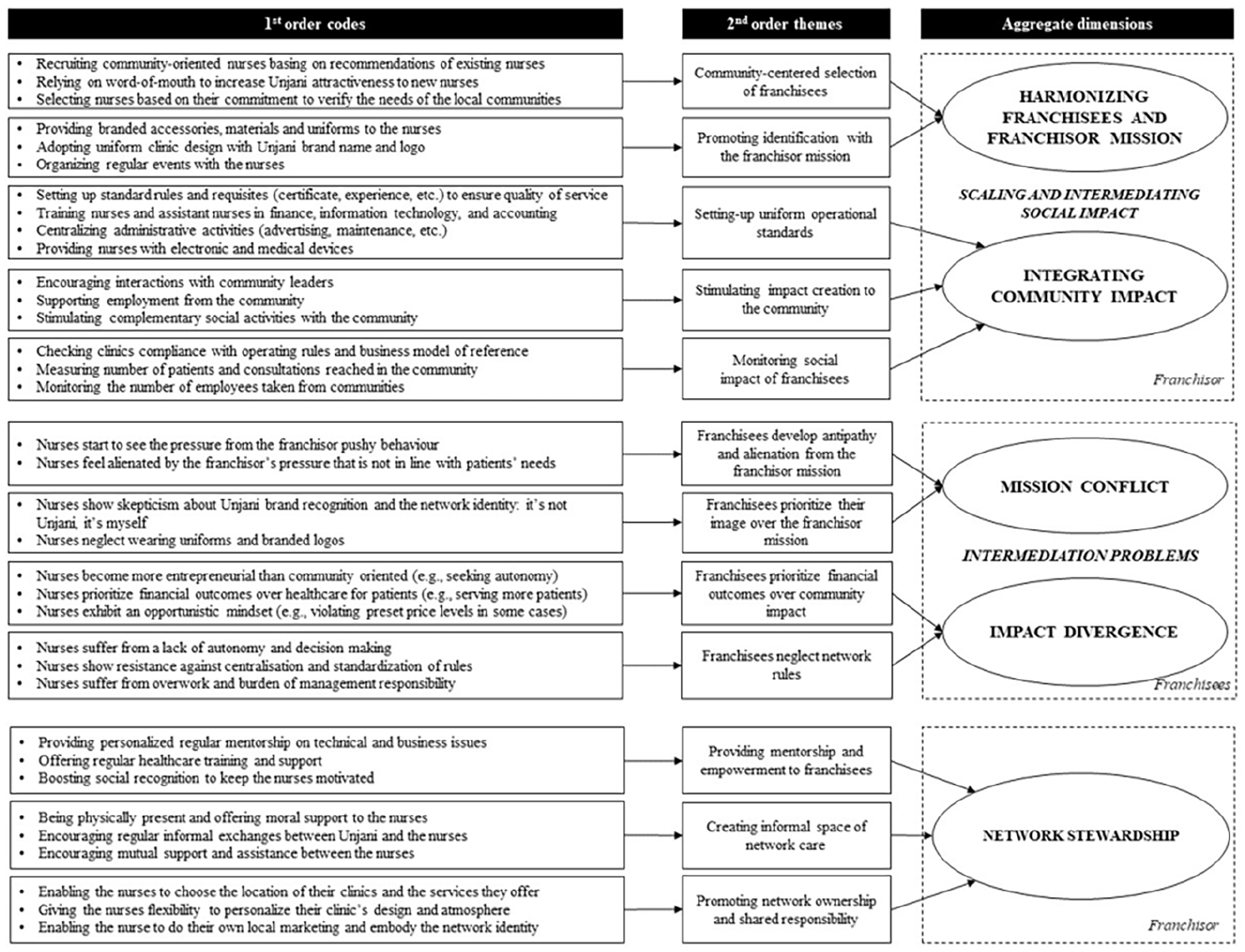
Data Structure.
The third stage involved a close-up examination of the relationships between the constructs to develop a theoretical model that defines the link between the second-order themes and aggregate categories (see Gioia et al., 2013). This step enabled us to develop novel insights and connections, for example, between intermediation problems and the solutions offered by what we labeled as “network stewardship.”
Findings
We studied Unjani Clinic to understand how intermediated social franchises extended health care services for disadvantaged rural communities. Figure 3 depicts a grounded model of impact intermediation in health care social franchising that depicts theoretical linkages between key constructs (Gehman et al., 2018; Glaser & Strauss, 1967; Locke et al., 2022). This section presents the results closely following the model in Figure 3, with the aid of selected quotes and illustrative examples. 3 The Supplementary Material contains an additional data table with illustrative quotes for each construct (Supplementary Table S4).
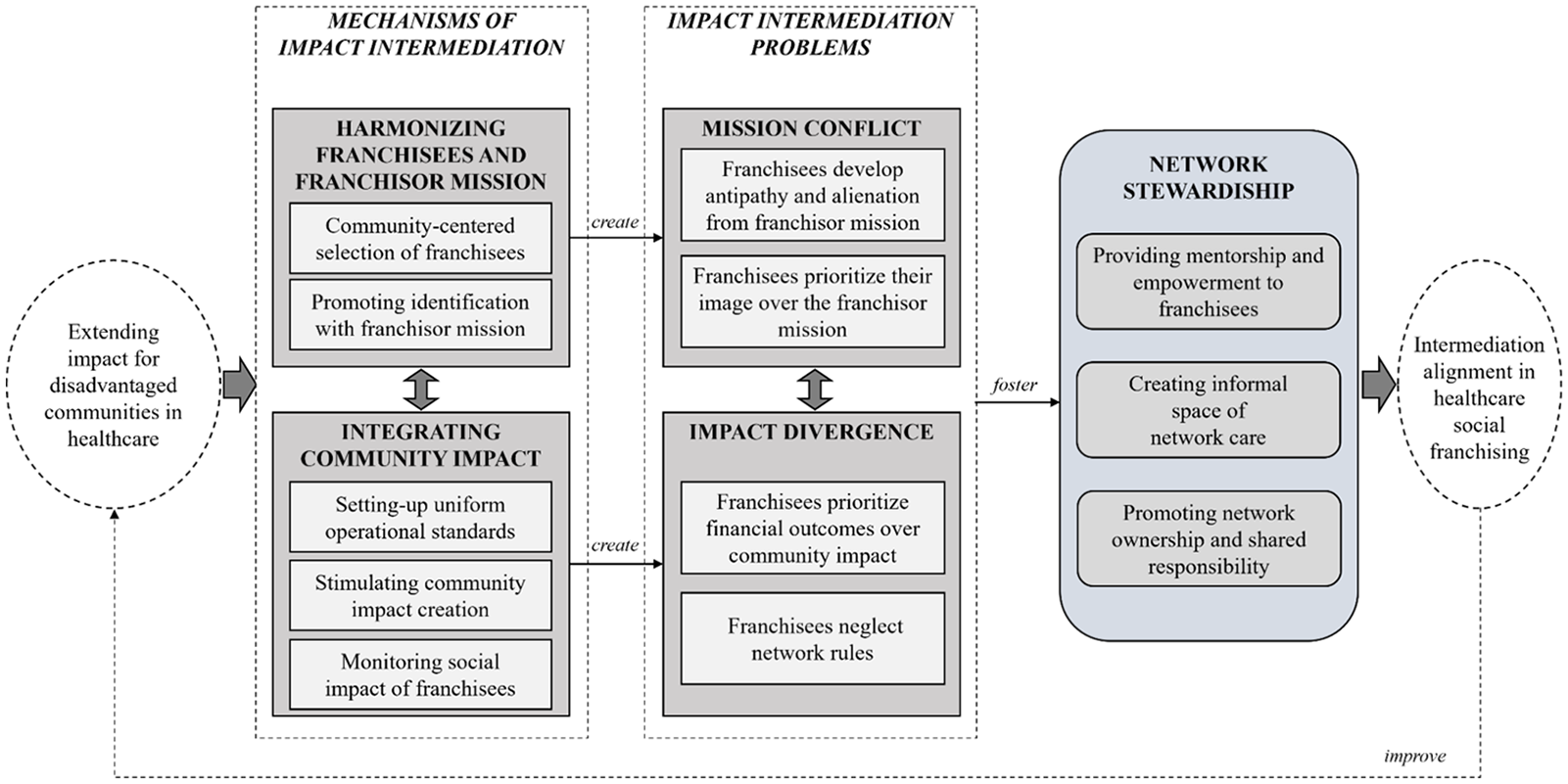
A Grounded Model of Impact Intermediation in Health Care in Intermediated Social Franchises.
We start by presenting the mechanisms of impact intermediation in Unjani Clinic, which entail various harmonization and integration practices designed to coordinate social impact at multiple layers. We subsequently describe what we call intermediation problems (mission conflict and impact divergence), before finally explaining how Unjani overcame these challenges by fostering network stewardship.
Mechanisms of Impact Intermediation
To create impact for the franchisee nurses, their patients, and the community at large, Unjani introduced various mechanisms of impact intermediation. Data analysis revealed two critical coordinating practices: (a) harmonizing the mission of the franchisees and the franchisor and (b) integrating community impact into the franchise network.
Harmonizing Franchisees and Franchisor Mission
From the outset, Unjani sought to ensure that its franchisees shared its mission of empowering nurses and providing affordable and quality health care services to low-income patients. Unjani tried to create a harmonized mission through a community-centered selection of franchisee nurses and through practices that promoted identification with its mission.
Community-Centered Selection of Franchisee Nurses
To ensure that the nurses shared its mission of creating community impact, Unjani selected nurses that have an interest to serve their respective communities. This is clear from the following comment by the CEO of Unjani: We leave the decision on where the clinic should be open to the nurse. We’ve seen good outcomes from that because nurses who are parts of a community want to give back to that community. Our nurses want to go to their villages and provide services. (Lynda, CEO)
To filter among the applicants, Unjani sought the recommendations of other nurses that were already members of its network. Candidates applied to join the network after hearing positive news from other nurses, leading to the selection of like-minded nurses that share an interest in community service.
The selection process required applicants to interview 200 community members to identify the health care needs of the targeted community. In addition to establishing market demand, this task was used to test the commitment to the nurses: “It is a very good practice because many of the nurses fall out at the survey stage. It becomes too much work for them to do 200 surveys” (Lynda, CEO). Unjani also conducted comprehensive interviews with the nurses to ensure that the values and expectations of the nurses were aligned with those of the franchise network. This relatively complex selection process was designed to ensure that only capable and committed nurses were able to join the network, which reduced the risk of adverse selection and associated agency costs.
Promoting Identification with the Franchisor’s Mission
Once the nurses were selected, they were expected to adopt uniform standards and work procedures that were designed to increase their identification with the overall mission of the franchisor. The franchisor, Unjani, adopted a uniform branding strategy that embodies its own brand, from the design of the clinics to the packaging of accessories, and the uniforms worn by the nurses. According to Unjani’s network manager, the intention was to ensure that “the clinics look the same in terms of color, brand, where the posters are, and what the nurses wear . . . It is a brand.” Uniform branding enabled the patients to easily recognize the clinics and to expect comparable, high-quality services. These harmonization practices enabled Unjani to create a shared identity around its network, thus imprinting its mission upon the franchisee nurses.
Integrating Community Impact
Our analysis identified three ways through which Unjani integrated community impact in the franchisee clinics: setting-up uniform operational standards; stimulating impact creation to the community; and monitoring the social impact of franchisees.
Setting Up Uniform Operational Standards
Unjani took several measures to ensure that the franchisee clinics provided a service of relatively high quality. First, Unjani recruited nurses that have sufficient skills to provide high-quality health care. For example, the nurses were required to have a minimum of 5 years of experience. Unjani further provided additional training programs that were designed to enable the nurses and their assistants to operate their clinics effectively. These programs included, inter alia, training in financial management, information technology, and accounting. Unjani’s training program for new nurses was designed to help them “understand how the Unjani network operates, what the rules are, and what the processes, standards and operating procedures are, so that everyone operates in the same way” (Sue, General Network Manager).
Finally, Unjani centralized administrative activities, such as maintenance, advertising, and acquisition of medical stock. It also provided the clinics with a standard set of electronic and medical devices for the delivery of critical health services. Standardization enabled a uniform health care service, ensuring that patients in different clinics received the same quality of care. Moreover, uniform operational standards improved the efficiency of coordinating clinics by optimizing the cost of operating the clinics. Finally, uniform standards facilitated the replicability of the franchise model since new clinics could easily plug into the existing system.
Stimulating Impact Creation to the Community
To advance community-level health outcomes, Unjani encouraged its nurses to work closely with other community members, identify local needs, and adapt their services accordingly. This is illustrated by the following quote: The community could say, we have got a lot of alcohol abuse problems . . . The clinics will then take measures and work closely with community leaders to create awareness about the problem. (Lynda, CEO)
Unjani encouraged the nurses to participate in various social activities to identify community needs and provide solutions. For example, some of the nurses led gardening initiatives to promote and teach healthy eating practices while earning additional income by selling vegetables.
Monitoring the Social Impact of Franchisees
Unjani regularly assessed its clinics to check their compliance with operating rules and standards. The nurses submitted monthly financial reports and their accounting books were audited at least once a year. The CEO explained additional efforts to monitor the network’s social impact: “We measure and follow up the number of patients that we have helped through each clinic. We also have a research program to understand the qualitative impact on the patients” (Lynda, CEO).
These monitoring practices were designed to ensure that the nurses complied with the operational rules created to maximize impact for all targeted beneficiaries. In other words, these practices were intended to facilitate impact intermediation by ensuring that the franchisee nurses provided high-quality service to their patients and communities, while also meeting the minimum technical requirements for the financial and technical sustainability of their respective clinics.
Intermediation Problems
The various harmonization and integration practices presented above enabled Unjani to coordinate social impact at multiple levels. However, our analysis revealed that these practices had an unintended adverse effect on the personal and professional lives of the nurses that operated the franchisee clinics. In particular, the nurses experienced mission conflict and impact divergence due to tight coordination processes that were intended to facilitate impact intermediation.
Mission Conflict
Franchisees Felt Antipathy and Alienation
Unjani’s efforts to imprint its mission on the network through various coordination processes were perceived by some nurses as too pushy. They expressed their feeling of displeasure: “If you are not attending all the time [events and meetings], they will be like ‘You are the bad child who is always missing . . .’ Sometimes you just go down to accommodate them” (Nina, Nurse). Furthermore, some nurses questioned the appropriateness of Unjani’s involvement in their clinics while lacking sufficient knowledge about the needs of their communities. The following quote indicates this sentiment of irritation and alienation: Most of the time, you must do this and this and this. That’s stuff that the network is supposed to make. But I know my clinic and my patients better than them, I know my clinic’s needs. I just feel this is unfair. (Mary, Nurse)
Franchisees Prioritize Their Image Over the Franchisor’s Mission
Some nurses expressed skepticism toward the value of the Unjani Clinic brand. They felt that the value of their clinics came from their own personal recognition and not from the franchise network’s image: The name exists because we exist. . . . In this area when you talk about Unjani, they know me. So, the name [of Unjani] does not really affect me if I leave [the network]. Because they want me, not the name. (Nina, Nurse)
Some nurses tended to value their own image over Unjani’s and did not always meet Unjani’s branding requirements. They ignored the requirement to wear Unjani uniforms and were critical of the policy: “I don’t think is necessary. We left the government facility because of that. I am against this strictness!” (Gwen, Nurse).
The negative feelings of some nurses toward Unjani rules suggested mission conflict, which emerged from a gap between the values and goals of the network and those of the nurses. Some nurses were in effect moving away from the common mission of Unjani and asserting their own goals as individual clinic owners.
Impact Divergence
Franchisees Prioritize Financial Outcomes Over Community Impact
Because the clinics must achieve financial sustainability, Unjani attached importance to the business success of the nurses: “We told them: By the end of the year, you need to get to 300 patients a month, then you are sustainable and you break even financially” (Sue, Network General Manager). If the business acumen of the nurses was always valuable, it was problematic in some cases. The entrepreneurial orientation of some nurses appeared to be too strong as it took over their focus on health care service provision, as can be noted from this quote: “I like selling things. I like selling products. I like doing business” (Nina, Nurse). Some of the nurses started to develop very ambitious growth plans for their clinics: I still see the potential for the number to grow. I am looking to have another sister who can take the other room to provide full consultation, which may mean we double the numbers. (Lucia, Nurse)
Some nurses exhibited strong entrepreneurial mindset and expressed a desire for autonomy: “What I like is to be the boss of myself!! . . . I always wanted to be an entrepreneur . . . I am learning so many business skills” (Veronica, Nurse). For Unjani, increasing the number of patients per clinic was a way of amplifying its impact. However, the threshold of opportunistic behavior was rather thin. Indeed, some nurses, out of a desire to boost their profits, violated some of Unjani’s rules that were meant to maximize the impact created for communities. For example, Unjani received complaints from patients that a few nurses charged higher prices than the official rate. Lynda (the CEO) explained: “They were charging above network rates, which means they could see fewer patients for the same amount of money [. . .] That’s against network rules.” Unjani was insistent that these violations decreased the network’s social impact that was stipulated in its mission. Sue underlined: “our goal is about serving the community, isn’t it? It is not to earn money.” Unjani’s clear mission statement explains why some nurses were reluctant to express their views regarding what should be an acceptable practice in their clinics: “The solution for me is to keep quiet. Because whenever you charge [consultation price], it is like you are problematic . . . I’d rather stay quiet until I finish my 5 years” (Veronica, Nurse). In this case, the nurse was looking forward to graduating from and leaving the social franchising program in 5 years.
Franchisees Neglect Network Rules
Along with these opportunistic practices, some nurses decreased their engagement by abandoning some network rules and, in one case, leaving the network. The nurses resisted the centralization and standardization of rules: “I just have to comply, comply, comply” (Mary, Nurse). They underscored their perceived lack of autonomy: I don’t want to report to somebody that tells me: Why did you not submit on time? Why is your financial summary like this? Why is this and this, etc. I am not a child, I am an adult, I just want to be independent. (Veronica, Nurse)
The nurses thought it unfair to be constrained by network rules and secure Unjani’s approval for major decisions. They were also unhappy that Unjani did not consult them before making key decisions that affected their clinics: “it happens that you are just being given no choice but being told how this is going to be like” (Nina, Nurse). For example, the nurses were critical about the acquisition of a customer relationship management system that did not meet their expectations. Some of them expressed frustration: “Sometimes I don’t feel like I am an equal partner to Unjani. I feel like I am an employee and not an employer” (Mary, Nurse). Some nurses that had a sense of independence developed distrust toward Unjani and showed anxiousness about the potential consequences of non-compliance: I don’t feel like I am in a private practice where I am working for myself. Because, if I don’t comply with things, I will get non-compliance letters that make me uncomfortable. I am scared of what will happen. Are they going to take the clinic? What are they going to do? That is scary. (Veronica, Nurse)
The nurses neglected the rules mostly because they wanted entrepreneurial autonomy to take their clinics where they wanted to. However, some of them also showed negligence because they felt overwhelmed by overwork and managerial responsibility: “when it comes to human resources and medicine ordering that’s too much for me!” (Mary, Nurse). This pressure came from having to run their own businesses while also complying with complex network rules: “I feel like sometimes some of reporting is not really necessary, it just workload for you” (Nina, Nurse).
The problems of impact divergence are consistent with the mission conflict challenges discussed earlier. These mutually reinforcing intermediation problems threatened the quality of care provided to end-users as well as the sustainability of the entire social franchise model. They undermined the relationship between Unjani and the nurses and reduced the network’s attractiveness to new nurses, potentially decreasing its ability to create community impact.
Network Stewardship for Overcoming Intermediation Problems
Our analysis revealed that Unjani responded to the problems of mission conflict and impact divergence by gradually building a culture of network stewardship that would soften some of its rigid and complex practices. Unjani pursued various policies to empower the nurses, develop their sense of ownership, and nurture a sense of shared responsibility toward their clinics.
We identified three strategies that enabled Unjani to relax the rigidity of its coordination mechanisms that gave rise to the intermediations problems discussed earlier: (a) providing mentorship and empowerment to franchisees, (b) creating informal spaces of network care, and (c) promoting network ownership and shared responsibility. We aggregated these practices into an aggregate dimension of “network stewardship” because they enabled the franchisees to build a shared network culture. Network stewardship thus nurtured a sense of purpose and belonging that enhanced the franchisee’s commitment to creating social impact to their communities.
Providing Personalized, Regular Mentorship and Empowerment to Franchisees
To mitigate the prevalence of mission conflict and impact divergence, Unjani complemented its strict monitoring practices with regular personalized mentorship and empowerment efforts for the nurses. In addition to the standardized training session offered to the nurses at the start, Unjani provided complementary coaching and technical support on demand: “I normally ask them what I need to cover and see what the field visit for the day is” (Sue, Network General Manager).
On finance and management topics, Unjani’s internal staff provided training to the nurses. Constant engagement that fostered a close, informal relationship between Unjani’s staff and the nurses enabled Unjani to provide on-demand support in lieu of formal monitoring. Sue commented: “I try to go and see them every month just to push them, to see what they’re doing, and check if there is anything we can assist them.”
Moreover, Unjani regularly invited external speakers to train the nurses on various health-related topics. One of the nurses concurred: “You don’t just stay qualified, you upgrade, and you update yourself. Through the network, they give us this chance” (Naomi, Nurse).
To encourage the nurses to improve their performance, Unjani also created awards for nurses that achieved the year’s best results. Instead of creating rivalry, this award system seemed to motivate the nurses. Many nurses in fact indicated that seeing others’ accomplishments gave them confidence that they too could achieve the same level of performance. For the winners, prizes were valuable because they enabled them to get social recognition from Unjani and other nurses, boosting their morale and commitment to the franchise network.
Regular training and mentorship enabled the nurses to improve their knowledge and skills, while competitive prizes improved their motivation. Most of the nurses appeared very grateful: “I would not be successful without being mentored . . . I would not be here if I tried to do that alone” (Petra, Nurse). The mentorship and personalized support were especially valued by nurses who lacked confidence in their business competencies. One of the nurses, Petra, explained: “Having your own clinic is not about seeing patients, you need someone to help you, like a mentor. Unjani is in a sense like a mentor to me.” In sum, the provision of regular mentorship and empowerment seems to enable the nurses to overcome the risk of mission conflict and impact divergence.
Creating Informal Space of Network Care
Unjani developed informal spaces of network care with and among the nurses, which led to strong emotional bond and trusting relationships that enabled them “to be close, like a family” (Sue, Network General Manager). For example, Sue made unplanned courtesy visits and sent text messages to cheer up the nurses. This kind of friendly spontaneous support seemed to boost the confidence of the nurses: Unjani even calls us champions. They create a positive attitude about us . . . It is a good feeling. You wake up every day looking forward to doing something because people appreciate what we are doing. (Nina, Nurse)
This informal relationship did not prevent Unjani from preserving formal communication with the nurses when necessary: “I speak to Lynda if I have anything I have to tell, I can phone her or write an SMS or WhatsApp. If it is more an official thing, then I write an email” (Terry, Nurse).
The trusting relationship between the nurses and Unjani staff appeared useful for improving the clinics’ service quality. Indeed, the nurses felt free to make suggestions for improving the quality of health care. The culture of open dialogue also enabled Unjani to support the nurses based on their demands, which improved their well-being and enhanced their ability and willingness to deliver high-quality health care.
The nurses also developed an informal space of care among themselves. Unjani introduced the nurses to each other, and “from there, they just built their own relationships” (Sue, Network General Manager). Through their own WhatsApp group, the nurses exchanged advice and information for improving their knowledge and practices: “We always share each other’s expertise. Sometimes my colleague will tell me how I do this, and other times I am able to tell them . . . in terms of how we work” (Gwen, Nurse). The nurses also used their network to provide emotional support for one another: “We use this WhatsApp group to motivate each other, share good news and sad news, and just to support one another” (Nina, Nurse). Sue explained that this was indeed one of the reasons why Unjani created the WhatsApp group: “I don’t want them to feel lonely. . . . When they start having a friendship, they have that cohesion.” It is interesting to note that Unjani staff did not join this group as members, preferring to give the nurses their own space.
This caring environment improved social cohesion so that the nurses felt comfortable with each other—something we were also able to observe during the field visit. The presence of sound working relationships between the nurses further strengthened their professional collaboration. For example, nurses of the same neighborhood created special outreach events together without relying on Unjani’s support. The network of care that the nurses developed among themselves, and by extension with the franchise network, directly influenced their commitment to deliver quality health care to their patients and their communities. Overall, creating an informal space of care nurtured a positive relationship between the nurses and with the franchisor, overcoming some of the intermediation problems.
Promoting Network Ownership and Shared Responsibility
We observed that Unjani afforded a level of flexibility to the nurses to facilitate a feeling of ownership and shared responsibility toward their clinics, the network, and their community. For example, Unjani at a later stage introduced policies that allowed the nurses to choose which services to offer based on the needs of their communities: In terms of the services I offer, if I don’t want to do pregnancy tests, I am not doing it. They [Unjani] are not going to say “no, this is a service that your community wants.” If I don’t want to see pregnant women, they are ok with that. (Nina, Nurse)
Unjani also allowed the nurses to adjust the standardized clinic layout. Many nurses adapted the design of their clinics to make it more comfortable to their patients and to meet their own needs. As the clinics were made from refurbished containers, the freedom to personalize them allowed the nurses to convey reassuring messages to their patients: When the patients come in, they see that the place is clean. They sit comfortably [. . .] They are welcome with a smile. They really feel welcomed. (Gwen, Nurse)
This freedom enabled the nurses to differentiate themselves from others by decorating their clinics in a manner that reflected their own identities, which seemed to reinforce their passion for their jobs: “They [the patients] come here because it is a quiet environment. So, it is not about the number for me, it is about the impact I create. . . . I want to change people’s life” (Naomi, Nurse).
Unjani also allowed the nurses to conduct complementary marketing activities at a local level, such as awareness-raising campaigns, along with a degree of implementation leeway. For instance, they could choose the media and the content they wanted to display although Unjani conducted oversight to ensure brand uniformity. The CEO corroborated the value of this flexibility: “It is really about the community clinic, not necessarily about the brand. We don’t do big marketing campaigns around Unjani, it is all around the individual clinic that we advertise.” The freedom to make personal adaptations enabled the nurses to nurture a sense of connection with their local communities. The nurses developed a local identity that, supported by the personalization of their clinics, enabled them to maintain distinct relationships with their patients: Sometimes, they [the patients] come all the way because they’ve built a relationship. They value their relationship with you, they trust you and then they will come, they will travel because they feel comfortable with you [. . .] That is the unique element that differentiates you from person to person, from clinic to clinic. (Gwen, Nurse)
By letting the nurses develop and express their own identities, Unjani indirectly enabled them to develop a sense of responsibility toward their clinics and the whole network. Greater autonomy and flexibility enabled the nurses to develop a close affinity with their patients and their communities. For the nurses and their communities, Unjani was no longer seen as an impersonal and overweening franchisor, but as a responsible and empathetic network of nurses embedded within the communities they serve. The nurses started to embody the mission of the network and to develop a sense of collective responsibility, identifying with the interests of the communities for whom they were creating social impact. These changes created stronger mission alignment between Unjani and its nurses, resolving intermediation problems that undermined the pursuit of shared communal responsibilities.
Discussion and Conclusion
Persistent inequality in health care access constitutes a major, complex grand challenge (Park et al., 2022; Vakili & McGahan, 2016) that requires innovative organizational forms and scalable solutions (Dorado et al., 2022; Ometto et al., 2019). Intermediated social franchises offer one pathway for extending access to health care, but there is scant evidence on how these organizations reconcile their diverse goals, which include creating impact to franchisees (nurses) and downstream beneficiaries (patients in rural communities).
Using rich qualitative data, this study has developed a grounded model that depicts how health care social franchises ensure that their franchisees get economic and social benefits while also extending health care access to a greater number of downstream beneficiaries. Our model has several unique features. First, it provided evidence of the complexity of impact intermediation in social franchises (Giudici et al., 2020; Kistruck et al., 2011), which requires complex processes to harmonize the franchisor’s and franchisees’ mission and to integrate community impact throughout the network. This study is among the first to theorize about the challenges arising from the “dual loci” of extending social impact in intermediated social franchises.
Second, we observed that these complex organizational processes give rise to intermediation problems in the form of mission conflict and impact divergence. From the viewpoint of the franchisor, complex coordination processes are vital for ensuring the creation of economic and social impact across multiple beneficiaries. The costs of intermediation, however, are mostly borne by the franchisees (nurses), who must abide by complex and restrictive operational standards. Our grounded model reveals that intermediation problems can be detrimental for the propagation of social impact as they introduce conflict between the franchisor and the franchisees, potentially leading to instability and mission drift (André & Pache, 2016; Ometto et al., 2019). Such problems can ultimately undermine the network’s goal of providing quality health care to a broad beneficiary base, such as patients from rural disadvantaged communities.
Third, the model shows how social franchises overcome the problems of mission conflict and impact divergence by developing network stewardship, which we define as a set of broadly shared values and practices that foster network cohesion and facilitate the pursuit of shared communal responsibilities. Network stewardship enabled actors to develop a shared identity (Giudici et al., 2020; Iddy et al., 2022), which was enacted through mentorship and empowerment, informal spaces of network care, and network ownership. These stewardship practices were critical for overcoming intermediation problems that prevail in health care social franchises, enabling them to extend social impact both for the franchisee (nurses) and the downstream beneficiaries (patients from disadvantaged communities). Our rigorous grounded model contributes to the growing stream of literature in social franchising and offers rich practical insights to health care systems as discussed below.
Intermediation Problems in Health Care Social Franchises
We contribute to the emerging literature on social franchising by documenting the challenges of creating social impact in what we called intermediated social franchises. Existent literature has highlighted the nature of agency problems in social franchises (Kistruck et al., 2011; Tracey & Jarvis, 2007), which compounds the problems of identity conflict and mission drift that beset social enterprises in general (Battilana & Lee, 2014; Ciambotti et al., 2023; Ometto et al., 2019; Ramus & Vaccaro, 2017). The literature points to the role of governance mechanisms for improving the ability of social franchises to achieve scale (Giudici et al., 2020) and navigate trade-offs between social and commercial goals (Ometto et al., 2019; Smith & Besharov, 2019). Our research extends this literature by examining the unintended effects of complex coordination processes that seek to optimize social impact and commercial profit in intermediated social franchises. We found that formal organizational mechanisms to harmonize and integrate mission across the franchisor, the franchisees, and downstream beneficiaries eventually gave rise to intermediation problems in the form of mission conflict and impact divergence. Against the grains of the recent literature that underscored fine-tuning organizational designs to advance social impact (Ometto et al., 2019; Smith & Besharov, 2019), our results point to the potential limits of elaborate organizational structures for coordinating social impact.
Our results indicate how idealistic goals in health care social franchises could end up creating new agency costs that overburden the nurses operating the franchisee clinics. Most of the nurses in Unjani Clinic’s network came from the public sector hoping for a less burdened and financially rewarding alternative to employment in the low-paying and inefficient public health care system. Yet, price ceilings and service restrictions reduced their financial returns while heavy and stifling oversight led to a sense of alienation, dejection, and antipathy. Lack of autonomy to decide on their own operations also undermined the ideals of maximizing community welfare. These problems threatened the integrity of the franchising network, as they incentivized the nurses to prioritize their own individual brands over the network brand and to maximize their own financial profit at the cost of community impact. While our results are broadly in line with the importance of decentralized governance for overcoming these problems (Giudici et al., 2020; Iddy et al., 2022), they underscore that informal governance systems can be especially valuable for reducing these kinds of agency problems.
A parallel to our results is the recent challenge of heightened workload and infection risk among nurses during the COVID-19 outbreak (Li et al., 2020). Health care professionals had to endure social isolation, loneliness, and sleep disturbances in the face of significant exposure that vastly increased their infection risk (Krishnamoorthy et al., 2020). In South Africa, where the health care system was already strained by perpetual epidemics, more than 40% of nurses in a study were screened positive for higher levels of post-traumatic stress disorder (Engelbrecht et al., 2021). This recent evidence points to the dilemma faced by social franchisors, who seek to introduce additional duties of community care among health care professionals who are already underpaid and overburdened.
Network Stewardship for Mitigating Intermediation Problems in Social Franchises
Our results, nonetheless, point to the importance of nurturing network stewardship to create a supportive franchise network. Among other things, network stewardship enables the franchisor to find ways for extending community health care without overtaxing the nurses. In times of crises like COVID-19, a stewardship culture that is anchored on mutual care, reciprocity, and a commitment to a shared cause can afford greater flexibility (Hernandez, 2012). By blending agency and stewardship theories, our integrative analysis unpacks how a stewardship culture can help circumvent mission conflict and impact divergence that bedevil intermediated social franchises. A culture of network stewardship supported the professional and personal development of the franchisees and gave them greater decision-making autonomy, reducing the need to rely on cumbersome formal organizational processes. Such a culture enhanced ownership and commitment by promoting the development of distinct network values and the identification of network members with these values. It also enabled organizational members to obtain a sense of fulfillment through the success of the whole network rather than the success of their individual clinics. Network stewardship facilitated the pursuit of shared communal responsibilities among diverse members of the social franchise network, thus mitigating identity conflict and mission drift that often jeopardize the pursuit of hybrid goals (Battilana & Lee, 2014; Ciambotti et al., 2023; Ometto et al., 2019; Ramus & Vaccaro, 2017). These results point to the importance of attending to the higher-order psychological and social needs of network participants to advance the pursuit of shared communal responsibilities in social franchises.
Practical Implications
The study has several managerial implications for organizations that seek to attenuate health care inequalities by extending access to affordable primary health care for disadvantaged, rural communities. The analysis reveals the need to pay attention to the distribution of agency costs among network actors in intermediated social franchises, which may not be borne equally by all involved stakeholders. Our case demonstrates how extensive harmonization and integration practices meant to reduce the franchisor’s agency costs had the unintended effect of stifling the franchisees. Managers of social franchises, therefore, need to be cautious to avoid intermediation problems that could end up undermining the incentive of network members.
We identified at least three pathways through which managers of social franchises can develop network stewardship. First, the franchisor can offer mentorship to improve the professional and personal development of the social franchisees. In Unjani, consistent regular support and mentorship enabled the nurses, who came from disadvantaged backgrounds, to succeed in their new roles as entrepreneurs and social service providers. Second, social franchisors can create a space where the franchisees could develop an informal network of care. The experience of Unjani shows that this practice improved the emotional resilience of nurses who worked under severe pressure, enhanced knowledge and information sharing, and facilitated the development of a culture of reciprocity and care. Finally, franchisors could promote network ownership and shared responsibility among the franchisees by offering them greater autonomy and flexibility. A culture of network stewardship founded on these practices can enable a more flexible and adaptive social franchise network. The result of the study also offers implications for policymakers in the health care sector on the kinds of social franchises that can successfully extend primary health care access. The distribution of grants and funding schemes, for instance, could be geared toward social franchises that maintain a stewardship culture or otherwise reduce the agency costs borne by the franchisees.
Limitations and Future Research Directions
First, while our case study method is uniquely suited for understanding emergent, complex phenomenon through context-rich analysis, it is not amenable to generalization. Despite our best efforts to glean insights that are analytically generalizable across different contexts, they could nonetheless reflect key environmental factors, such as culture and institutional structures, that are unique to South Africa. For example, the importance of network stewardship could reflect the collectivist nature of African cultures (Manning et al., 2017), which calls for greater caution in the interpretation and generalization of our findings.
Second, while qualitative methodologies are suitable for answering why and how questions (Gehman et al., 2018), they could suffer from limitations such as social desirability bias and data reliability issues. While we have taken several measures to reduce these risks, additional empirical research is needed to validate and/or extend our results, for instance through theory-testing studies that use quantitative methodologies.
Third, while focusing on impact intermediation for the sake of concision, we might have left out other factors that are relevant for the creation of social impact among social franchises. For example, we have not focused on the revenue model of the social franchise, market competition, and other related contingencies. Future research can extend our findings by addressing how, for example, the financial autonomy of the social franchise or its legal form (for-private or non-profit) influences its ability to create impact and scale its operations.
Finally, while our analysis suggests that network stewardship can serve as a means for overcoming agency problems in intermediated social franchises, the efficacy of this mechanism could depend on other contingencies. For example, network stewardship could have diminishing importance after the number of franchisees reaches a certain point because managing relationships could become overly burdensome. Additional comparative analysis is needed to gain insight into the conditions under which network stewardship facilitates successful creation of social impact. Overall, we hope that the study will inspire and enrich future research into new, innovative organizational forms that can help overcome health inequalities by extending health care access to disadvantaged communities.
Supplemental Material
sj-docx-1-bas-10.1177_00076503241255479 – Supplemental material for Addressing Health Care Inequality Through Social Franchising: The Role of Network Stewardship in Impact Intermediation
Supplemental material, sj-docx-1-bas-10.1177_00076503241255479 for Addressing Health Care Inequality Through Social Franchising: The Role of Network Stewardship in Impact Intermediation by Constance Dumalanède, Giacomo Ciambotti and Addisu A. Lashitew in Business & Society
Footnotes
Acknowledgements
The authors are grateful to the handling Guest Editor, Jill Brown, for her exceptional guidance during the review process. They are also thankful to three anonymous reviewers for their highly constructive feedback that helped us substantially improve the manuscript. Constance Dumalanède would like to express her deepest gratitude to the management team of Unjani, especially Lynda Toussaint and Sue Hoosain, for their warm welcome and unreserved support during her fieldwork. The authors would also like to thank track organizers at EGOS 2023—Pilar Acosta, Joel Bothello, and Stefanie Habersang—as well as several participants of the conference for their constructive feedback.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.