
Abstract
Improvements in the health capital of citizens are central to the development of countries. By exploiting steep decreases in antiretroviral drug prices and the subsequent increases in antiretroviral therapy (ART) coverage, we test whether the resulting improvements in the health of the population are associated with the prevalence of entrepreneurial activity and whether entrepreneurial activity strengthens the relationship between ART coverage and a country’s development. Drawing on a sample of 87 low- and middle-income countries (2006–2019), we find that a 1% increase in ART coverage is associated with a 1.5% increase in the number of newly registered limited liability firms; however, there is no significant relationship with (male or female) self-employment. Higher ART coverage is particularly associated with development—as proxied by gross domestic product (GDP) per capita and the Human Development Index—in countries with low levels of new business formation and high proportions of self-employment.
Entrepreneurship is of crucial importance for the economic development of countries (Carree & Thurik, 2010; Van Praag & Versloot, 2007). Entrepreneurs, for instance, contribute to job creation and the commercialization of innovations (Audretsch, 2007, 2018; De Wit & De Kok, 2014). Shifting from the economic contributions of entrepreneurs, several recent studies have found that there is a positive association between entrepreneurship and health (Bradley & Roberts, 2004; Castellano & Punzo, 2013; Stephan & Roesler, 2010; Tetrick et al., 2000; Toivanen et al., 2019). Although switching to entrepreneurship may have a short-term positive effect on health (Nikolova, 2019), health capital particularly influences entry into entrepreneurship (Rietveld et al., 2015, 2016; Yoon & Bernell, 2013). Besides, good health is a critical factor for venture performance (Hatak & Zhou, 2019; Hessels et al., 2020).
Although health is an important consideration for individual-level entrepreneurship, its implications at the country level are seldom studied. Following Crane and colleagues (2016), we focus on generating a synthesis of the literature on health and entrepreneurship by focusing on a specific region of the world, low- and middle-income countries. That is, we refine and adapt prior works on developing countries and telescope away from developed country contexts to study phenomena of country-level health capital in developing country contexts to develop a refined understanding of the value of health capital improvements for entrepreneurship in a country. The refinement based on theory and context is salient given only three studies focusing on the role of health and entrepreneurship (at the individual level) in developing countries: Djankov and colleagues (2005) and Nikolova and colleagues (2012) use health as a control variable, and Rietveld and colleagues (2015) show that the positive relationship between entrepreneurship and health is also present in four Caribbean Basin countries.
The proposed theoretical refinement is important for two reasons. First, compared with developed countries, the average health capital is relatively low in developing countries (Legatum Institute, 2019). Health care infrastructures and access to medical facilities are often limited in developing countries, resulting in lower average health capital among the population. Limited access to affordable health care, lack of social safety nets, and inadequate supportive policies can all contribute to the challenge of maintaining good health while pursuing entrepreneurial endeavors. The stress and uncertainty inherent in sustenance-based entrepreneurship, typical in developing country contexts, can take a toll on the mental and physical well-being of entrepreneurs. When compared with their counterparts in more developed nations, a combination of factors, including limited health care access, necessity-driven entrepreneurship, economic challenges, and insufficient support systems, collectively contribute to the likelihood of worse health outcomes among entrepreneurs in developing countries. While the necessity to examine the health of entrepreneurs in developing countries is evident, it is important to recognize that alterations in health capital within a country often arise endogenously, thereby introducing greater inferential complexity into the relationship between health and entrepreneurship.
Second, the need for theoretical refinement is even more pressing given the Global Entrepreneurship Monitor’s (2020) report on the relatively high prevalence of self-employment in developing countries as compared with developed countries. In developing countries, many individuals start a business out of necessity (because of a lack of employment alternatives) rather than out of opportunity (driven by a profitable business idea; Fairlie & Fossen, 2018). Hence, the average potential of entrepreneurship is relatively low in these countries, which makes the relationship between entrepreneurship and economic development weak or even negative in low-income countries (Hessels & Naudé, 2019; Van Stel et al., 2005).
Considering these two factors, the double-whammy from limited health capital and increased challenges from entrepreneurship call for refinement of our understanding of the role of health capital improvements and the role of entrepreneurial activity on (economic) development. Therefore, in this study, we analyze the impact of exogenously induced improvements in aggregate health capital on the prevalence and nature of entrepreneurship in low- and middle-income countries as well as the role of entrepreneurial activity in strengthening the relationship between health capital and economic development. Our identification stems from the steep drop in prices of antiretroviral therapy (ART) designed to lower the viral load of human immunodeficiency virus (HIV) among those with acquired immunodeficiency syndrome (AIDS). The challenge in the early days was the mutation of HIV to drug-resistant strains; however, in 1996, a three-drug cocktail became the standard prescription that significantly lowered mortality from AIDS (Bor et al., 2013). Initially, the price of the treatment was high, about US$10,000 per patient per year. Between 2000 and 2001, the entry of generic drug makers from India, the subsequent shift in pricing strategy by the pharmaceutical industry, and the Clinton administration’s policy to override ART patent infringements in sub-Saharan Africa drove the prices to US$1,000 per patient per year. With most patients covered for ART in developed countries, low drug prices were a boon to the ones in poorer countries.
We draw on data from the World Bank and the Joint United Nations Programme on HIV/AIDS (UNAIDS) to relate ART coverage to two empirical measures of entrepreneurship. In a sample of 87 low- and middle-income countries (2006–2019), we test for the relationship between ART coverage and a country’s new business density (newly registered limited liability firms) as well as its self-employment rate (Henrekson & Sanandaji, 2020). Due to higher informality in developing countries, new business registrations of firms with employees signify new firms with viable business activities that could be salient to innovation, growth, and economic value creation. The new business density measure captures the creation of new ventures that introduce novel products, services, or business models, leading to market disruption and competitive advantage. In our context, self-employment is primarily an indicator of the prevalence of necessity-based entrepreneurship under challenging economic circumstances. Moreover, extending the analysis of Tompsett (2020) and building on the knowledge spillover theory of entrepreneurship (Braunerhjelm et al., 2010), we also test whether entrepreneurship amplifies the relationship between ART coverage and the development of a country, as proxied by gross domestic product (GDP) per capita and the Human Development Index (HDI).
Our research introduces several novel contributions to the literature. First, we shift our lens from the individual level to the country level, investigating the influence of population-level health capital improvements on entrepreneurial activity. This macro perspective advances the existing literature, which predominantly concentrates on the individual-level interplay between entrepreneurship and health. Within this broader context, our study fills two critical gaps: (a) the intersection of health and entrepreneurship within developing countries, and (b) the exploration of exogenously induced improvements in health capital at the population level. These dimensions collectively augment the business and society literature. Notably, our approach uniquely connects macro-level health considerations with entrepreneurial dynamics, presenting an innovative linkage that, to our knowledge, has not been previously explored.
Second, our examination focuses on the pivotal role of ART coverage as a determinant of entrepreneurial activity. Our findings reveal a compelling correlation—a 1% rise in ART coverage corresponds to a substantial 1.5% increase in newly registered limited liability firms. This result underscores the affirmative impact of ART coverage on the formalized entrepreneurial sector and lends insights for policymakers and practitioners seeking to foster entrepreneurship within low- and middle-income countries. Although we do not uncover a significant association between ART coverage and self-employment, our emphasis on the formalized sector contributes crucial insights to the underexplored dimensions of entrepreneurial pursuits within developing country contexts. This differentiation between limited liability firms and self-employment enriches our comprehension of the entrepreneurial landscape, providing insights into diverse entrepreneurial ventures and their links with health enhancements.
Finally, we delve into the potential moderating role of entrepreneurial activity in the complex relationship between ART coverage and a country’s development—proxied by GDP per capita and the HDI. Our findings suggest that increasing ART coverage is particularly beneficial in countries with low levels of new business formation and high proportions of self-employment. These results suggest that improvements in the health capital of citizens impact the average quality of entrepreneurship in a country, strengthening the association between aggregate human capital and development. We underscore that our effect sizes are modest, reflecting the pragmatic nature of the relationships we explore, especially the fact that very high levels of growth driven by entrepreneurial activity are less feasible in developing country settings.
In sum, our research introduces a novel perspective at the intersection of health and entrepreneurship, encompassing macro-level dynamics, ART coverage, and their implications for development. In combination, these multifaceted insights contribute to the broader understanding of the relationships underpinning these dimensions.
Theoretical Background and Hypotheses
HIV is a retrovirus that attacks the immune system, making individuals susceptible to diseases and infections (Fauci, 2003; Fauci & Lane, 2020). One of the challenges with HIV is its relatively long latent period, which can last up to 15 years. During this period, infected individuals may not exhibit any symptoms, but the virus is still actively replicating and damaging the immune system. As the disease progresses, the immune system becomes increasingly weakened, making affected individuals more vulnerable to opportunistic infections and diseases. When the immune system is severely compromised, the individual is said to have AIDS, which is the most advanced stage of HIV infection. The fact that HIV primarily affects prime working-age adults has significant social and economic implications (Barnett et al., 2000; Fauci, 2003; Tompsett, 2020). Many individuals living with HIV are unable to work or face discrimination in the workplace, leading to lost income and reduced economic opportunities. HIV also places a significant burden on health care systems and can have a negative impact on the overall economic development of a country.
ART is a class of drugs that reduces the amount of virus in the body, thereby improving the functioning of the immune system and reducing the risk of opportunistic infections. However, ART is not a cure for HIV and cannot fully eliminate the virus from the body. One of the major challenges in developing effective ART was the rapid mutation rate of HIV, which allowed drug-resistant strains of the virus to evolve quickly. The key breakthrough in ART came with the development of combination therapy, which involves prescribing several drugs in combination to reduce the likelihood of resistance developing. This three-drug cocktail, which became standard in the late 1990s, has been highly effective in reducing viral loads and mortality rates in high-income countries. The dramatic reduction in the price of ART, facilitated by the availability of generic versions, was a crucial step in expanding access to treatment in low- and middle-income countries (Tompsett, 2020). However, other barriers such as lack of infrastructure and trained staff needed to be addressed as well. The international community responded with funding initiatives and other programs to increase access to ART. As of 2014, almost 15 million people in low- and middle-income countries were receiving ART. The coverage varied across countries and efforts were ongoing to address remaining barriers to expand access to the treatment (Mills et al., 2006). Against this backdrop, we develop our hypotheses in the two following subsections on the relationship between health and entrepreneurship and on the moderating impact of entrepreneurship on the relationship between health and development.
Health and Entrepreneurship
A burgeoning body of research focuses on the effects of health on the choice of transitioning into entrepreneurship and the implications of health on economic and noneconomic outcomes from entrepreneurship (Ryff, 2019; Wiklund et al., 2019). Although a detailed review of the literature is beyond the scope of this study, we refer interested readers to some recent literature reviews on this topic (Lerman et al., 2021; White & Gupta, 2020). Broadly, this research can be divided into positive and negative relationships between entrepreneurship on one hand and mental and physical health on the other hand. Earlier studies highlight the benefits of autonomy and self-actualization from entrepreneurship on health (Stephan, 2018). With the entrepreneurial earnings puzzle, or that the self-employed earn significantly less than wage-workers, receiving widespread support (Åstebro & Chen, 2014), the noneconomic benefits to health may be salient. Conversely, entrepreneurship can also exacerbate stress. Significant time demands of entrepreneurship and low survival challenges are associated with sleep problems (Gunia, 2018), worsening physical and mental health (Palmer et al., 2021), higher blood pressure (Stephan & Roesler, 2010), and an increase in allostatic load (Patel et al., 2019). The relatively long working hours in entrepreneurship (Nyström, 2021) also increase challenges to maintaining a good work–life balance (Adisa et al., 2019). To cope with health-related challenges, studies have found support for the role of exercise, mindfulness, and social support in mitigating health outcomes (Murnieks et al., 2020).
The studies on the relationship between health and entrepreneurship vary by the level of analysis, measurements of health, and empirical approaches (Ryff, 2019; Wiklund et al., 2019). Most of the studies draw on self-reports by individuals to test for direct, mediating, and more complex moderated-mediated relationships (Abreu et al., 2019; Nikolova et al., 2021; Uysal et al., 2022). As perceptions of individual health conditions could vary significantly, studies have also used biomarkers (Nicolaou et al., 2021), genetic risk scores (Rietveld et al., 2021), and lab measurements (e.g., body mass index [BMI] and blood pressure; Stephan & Roesler, 2010), among others. Overall, studies on entrepreneurship and health have shown that entrepreneurship can have both positive and negative effects on an entrepreneur’s health, and to mitigate the negative effects, entrepreneurs need to find ways to balance work and life, develop coping mechanisms, and seek out support systems (Wiklund et al., 2020).
Although most of the studies have focused on the individual-level relationship between health and entrepreneurship, studies in aggregated health capital provide further reasons for why this relationship can also be expected to exist at the country level. Following Grossman’s (2017) conceptualization of human capital as an important input to economic growth at the country level (Ke et al., 2011), the association between health and a country’s economic growth has been well documented in the literature (Barro, 1996). Health capital improves productivity (Tompa, 2002), improves human capital (Knowles & Owen, 1995), and lowers health care costs (Stadhouders et al., 2016). Improved health capital increases labor force participation (Cai, 2010), reduces absenteeism (Pauly et al., 2002), and increases productivity through increased work hours (Nie et al., 2015) or improved worker focus and performance (Schultz & Edington, 2007). Indirectly, health capital also increases investments in education and skills, which in turn increases long-term productivity and economic output (Harsløf et al., 2022). To improve health capital, governments can invest in health care infrastructure, medical research, and public health to not only create newer technologies and services to improve health outcomes but to also provide the necessary resilience to more sustainable and inclusive economic growth (Reeves et al., 2013).
Based on these studies, and noting that good health increases the ability to successfully run a business (Hatak & Zhou, 2019; Hessels et al., 2020), we also expect a positive relationship between average health in a country and entrepreneurship:
Entrepreneurship and Development
AIDS represents an epidemic that has created systemic poverty traps in low- and medium-income countries (Goenka et al., 2014; Goenka & Liu, 2020). A higher incidence of AIDS is a retardant to realizing human potential (Arndt, 2006) and is therefore associated with lower human capital stocks and entrenched poverty traps (Conroy et al., 2006). Poverty and disease drive poor health behaviors, which in turn lower labor force participation and worsen the quality of life (Kagee et al., 2011). The malaise from poverty and disease lowers labor force participation, reduces work opportunities, and lowers income (Hecht et al., 2010; Mayston et al., 2012). Increased diffusion of ART represents increased health care expenditures that improve the redistribution of health care expenditures and reduce poverty rates through improved health outcomes, which in turn could foster the development of countries (Mitchell et al., 2009).
Before the availability of affordable ART, the HIV/AIDS epidemic was a cause of death for many people in lower-income countries. However, once generic drugs drove down the cost of ART, coverage expanded rapidly, reaching 14.9 million people in lower-income countries by the end of 2014 (Tompsett, 2020). The expansion of ART coverage coincided with a period of economic growth in sub-Saharan Africa. This “growth miracle,” discussed in Tompsett (2020), refers to a growth pace of 2.1% between 2002 and 2014, compared with a 0.2% growth rate between 1990 and 2001. Although explanations range from economic and structural change and resource and commodities price booms, Tompsett (2020) finds that in the absence of ART growth rates between 2002 and 2014 would have been reduced to 1.4%. Studies have estimated the value of ART-related income gains (Resch et al., 2011; Tompsett, 2020) and/or welfare benefits of mortality reductions (Bor et al., 2013; Forsythe et al., 2019; Lamontagne et al., 2019), suggesting that ART coverage expansion may have played a role in fostering economic growth, by increasing life expectancy and enabling people living with HIV/AIDS to continue working and contributing to the economy (Barbour, 1994).
Based on the arguments constituting Hypothesis 1, for Hypothesis 2, we propose that higher entrepreneurial activity would induce a stronger positive association between ART coverage and development outcomes. The moderation effect can be understood through the lens of the knowledge spillover theory of entrepreneurship (Braunerhjelm et al., 2010). This theoretical framework suggests that entrepreneurship triggers a virtuous cycle of knowledge dissemination, fostering innovation, and amplifying economic development (Acs et al., 2009, 2013; Iftikhar et al., 2020). Entrepreneurial activities serve as conduits for the diffusion of knowledge across sectors, catalyzing novel business ideas and technological advancements. The knowledge spillover theory helps to refine our understanding of how entrepreneurship moderates the impact of ART coverage on development. In accordance with the knowledge spillover theory, regions characterized by strong entrepreneurial ecosystems are likely to benefit from an enhanced exchange of information and expertise (Plummer & Acs, 2014). When considered in the context of ART coverage, the extent of entrepreneurship can facilitate the dissemination of knowledge that can strengthen the ART coverage and development relationship. The knowledge spillover theory also highlights that entrepreneurial activities that embody innovation and knowledge diffusion contribute not only to economic growth but also to the creation of an environment conducive to improved health outcomes. As entrepreneurial initiatives proliferate, the dissemination of knowledge in the entrepreneurship milieu can result in the developmental benefits of ART coverage. The knowledge spillover theory also underscores the potential for entrepreneurship to bridge gaps in health care accessibility. By fostering innovation and disseminating health-related information, entrepreneurial activities can contribute to the development of localized solutions that address health care disparities, including barriers to ART access. These solutions can range from innovative distribution methods to community-driven awareness campaigns. Consequently, the synergy between entrepreneurship and ART coverage, as proposed in the moderation hypothesis, finds support in the theory’s premise that entrepreneurship can serve as a conduit for knowledge dissemination and localized problem-solving.
More specifically, we expect that a higher prevalence of entrepreneurship strengthens the relationship between ART coverage and development for the following reasons. First, the proposed moderation effect concerning the interplay between ART coverage and development outcomes aligns with key tenets of development economics (Goenka & Liu, 2020). Empirical evidence substantiates that regions characterized by robust entrepreneurial ecosystems tend to demonstrate a heightened capacity to leverage expanded ART coverage for developmental gains (Malecki, 2018). This alignment underscores the intrinsic interconnectedness between health and economic factors. Entrepreneurial vigor has been empirically associated with amplified labor productivity and heightened consumer demand, in line with established growth theories (Naudé, 2013). Conversely, contexts with subdued entrepreneurial activity may attenuate the developmental impact of ART due to the lack of mechanisms to effectively translate health enhancements into economic advancements.
Second, the essence of entrepreneurial activity surpasses conventional business transactions; it encompasses an ecosystem conducive to innovation, adaptability, and sustainable economic practices. Aligned with Schumpeterian perspectives on innovation-driven growth, within economies nurtured by entrepreneurial activity, the infusion of ART resources harmonizes with ongoing business pursuits. The interplay reinforces a virtuous cycle wherein augmented health conditions, propelled by ART, bolster productivity resulting in a symbiotic nexus between health and development (Bloom et al., 2019). Entrepreneurial activity could help amplify health interventions into holistic development outcomes. In regions grappling with nascent or inadequate entrepreneurial ecosystems, the potential of ART to catalyze development might remain constrained, even in the presence of robust health care endeavors.
Third, the moderation effect extends to mitigating the adverse implications of limited ART access through entrepreneurial resilience (Iacobucci & Perugini, 2021). Entrepreneurship, facilitating economic diversification, is congruent with principles of structural transformation and adaptive economic strategies. In contexts enriched with robust entrepreneurial activity, economic diversification mitigates vulnerabilities stemming from restricted health care access. Entrepreneurial versatility in pivoting economic activities serves to ameliorate the potential repercussions of health-related challenges. Entrepreneurial activity emerges as a safeguard against setbacks arising from constrained ART availability, reinforcing community resilience and amplifying development’s stabilizing efficacy.
Taking together, we expect that
Method and Empirical Material
Sample
The World Bank classifies countries into the categories of low-income, lower-middle, upper-middle, and high-income. We analyze data from 87 low- and middle-income countries from the years 2006–2019. The start year is 2006 because in this year the World Bank formally started collating information on new business activity, and the end year is determined by the availability of other variables included in the models. While it could have been ideal to have data starting immediately after the steep fall in ART drug prices in 2001, the 5-year time lag does allow for capturing the diffusion and impact of ART coverage on entrepreneurial outcomes. Health interventions, like increased ART coverage after falling drug prices (Tompsett, 2020), often require time to manifest and influence societal outcomes because the process of intervention diffusion involves stages such as awareness, acceptance, adoption, and implementation.
Measures
Several empirical measures for entrepreneurship exist, with most of them being only available for more developed countries. Henrekson and Sanandaji (2020) have recently shown that most variation across entrepreneurship measures is accounted for by two distinct factors at country level: one relating to high-impact (so-called Schumpeterian) entrepreneurship and the other one relating to small business activity. In our study, we employ two main dependent variables: (a) the logarithm of new business density per 1,000 population and (b) the proportion of self-employment (% of total employment) that are representative of these two types of entrepreneurship. As ancillary outcomes, we analyze the proportion of self-employed females (% of female employment) and the proportion of self-employed males (% of male employment). The new business density measure captures newly registered limited liability firms only, and thus focuses on relatively larger businesses as most of the firms in low- and middle-income countries choose not to formally register and prefer to stay informal (Oviedo et al., 2009). Self-employment, on the contrary, is the most commonly used measure for entrepreneurship in empirical studies (Parker, 2018) and captures in particular sustenance-based self-employment in low- and middle-income countries. The businesses of self-employed individuals in developing countries are typically small and their owners have limited growth intentions. Data for these entrepreneurship measures are derived from the World Development Indicators provided by the World Bank.
To test Hypothesis 2, we analyze whether country-level entrepreneurship moderates the relationship between ART coverage and development, as proxied by (a) GDP per capita (constant 2017 international dollars), and (b) the HDI. The HDI as collected by the United Nations Development Programme is a summary measure index of life expectancy, education (mean years of schooling completed and expected years of schooling upon entering the education system), and per capita income indicators (Stanton, 2007). Each country scores between 0 and 1 on the HDI.
Our predictor variable, ART coverage is the percentage of people living with HIV who have ART coverage. The ART coverage data come from the Joint United Nations Programme on HIV/AIDS. The percentage of people living with HIV represents the aggregate negative health capital in a country and also represents the aggregate ART coverage necessary to mitigate the negative effects of HIV/AIDS on the health capital of the population. As a robustness check, we use the incidence of HIV in the population (per 1,000 uninfected population). This measure represents the aggregate negative health capital in a country and does not take into account therapy coverage.
As control variables, we include variables capturing the current health expenditure in a country (% of GDP), the logarithm of GDP per capita (constant 2017 international dollars), Foreign Direct Investments (net inflows as % of GDP), the logarithm of population size, the tertiary education enrollment rate, and year dummies. In addition, our fixed effect regressions control for time-invariant country-specific factors because cross-country differences in entrepreneurship appear to be rather persistent over time (Freytag & Thurik, 2007). Note that in the models testing Hypothesis 2, the logarithm of GDP per capita is excluded from the list of control variables because in these models this variable acts as a dependent variable. Throughout our models, we employ robust standard errors.
Results
Table 1 provides the descriptive statistics of the analysis sample. In total, there are 697 country-year observations from 87 countries (that is, we have an unbalanced panel). The poorest country (in terms of GDP per capita) in our data is the Democratic Republic of the Congo (2016, US$1,056), and the richest country is Oman (2006, US$37,369). Importantly, the number of newly registered businesses per 1,000 population ranges between 0.01 (Laos, 2008) and 20.09 (Botswana, 2016), and the proportion of self-employment ranges between 3.97% (Belarus, 2014) and 95.10% (Niger, 2018). ART coverage is lowest in Senegal (2006) and highest in Cape Verde (2018). From 2006 to 2019, mean ART coverage increased from 12% to 59%.Table 2 presents the correlations among the variables included in the models. Interestingly, the number of newly registered businesses per 1,000 population and the proportion of self-employment are negatively correlated (–0.520).
Descriptive Statistics of the Analysis Sample.
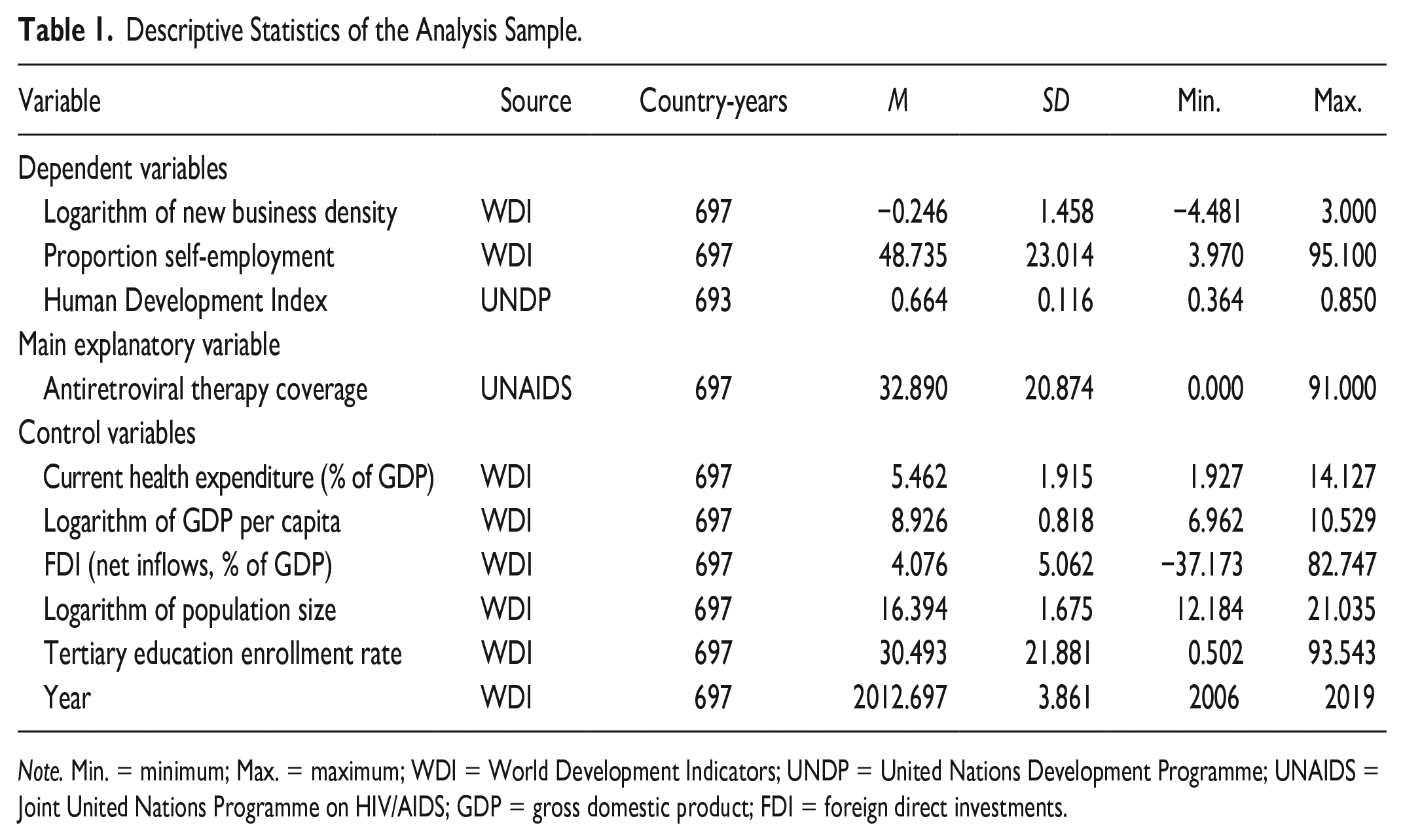
Note. Min. = minimum; Max. = maximum; WDI = World Development Indicators; UNDP = United Nations Development Programme; UNAIDS = Joint United Nations Programme on HIV/AIDS; GDP = gross domestic product; FDI = foreign direct investments.
Descriptive Statistics of the Analysis Sample (Correlations).
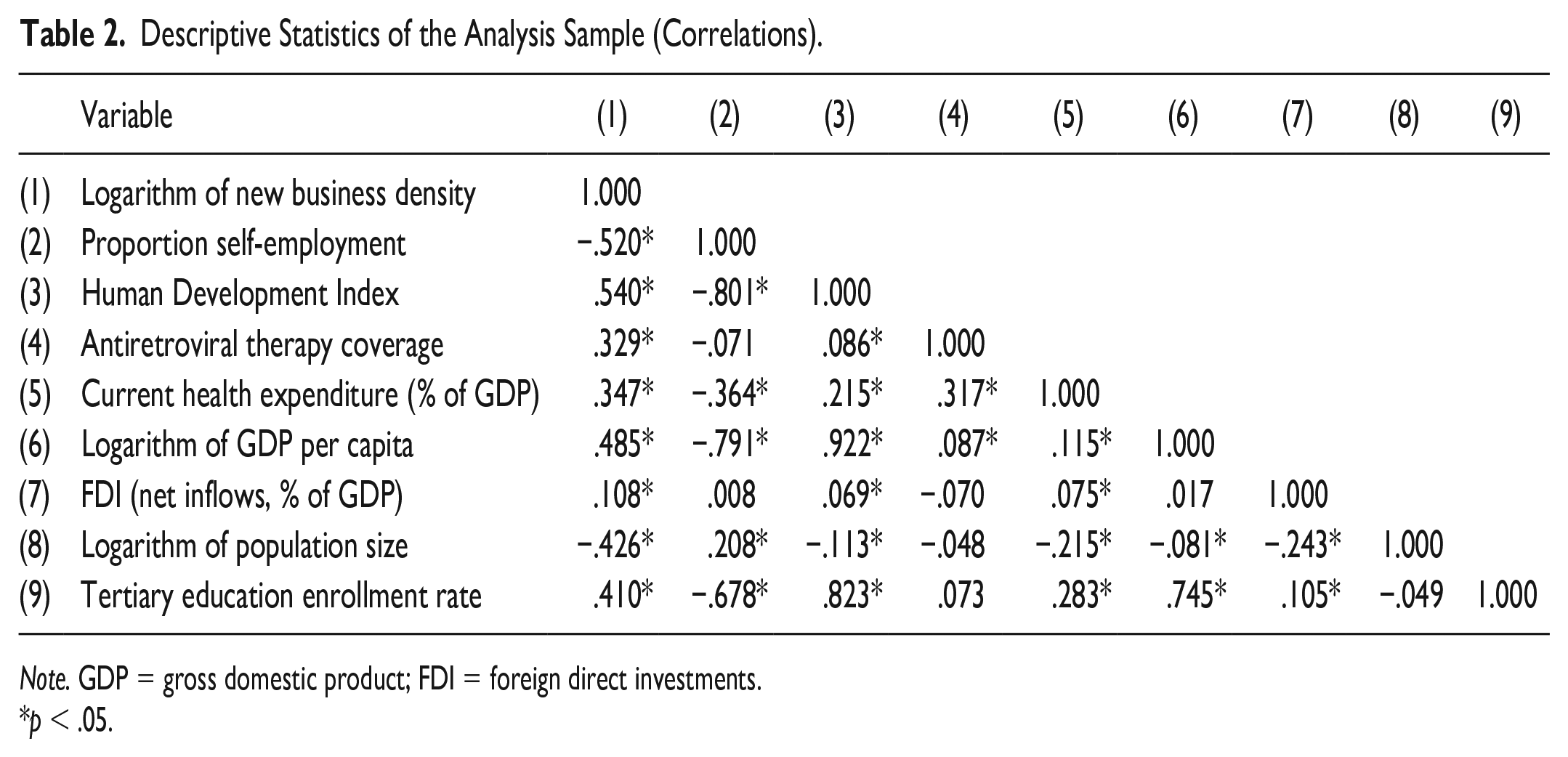
Note. GDP = gross domestic product; FDI = foreign direct investments.
p < .05.
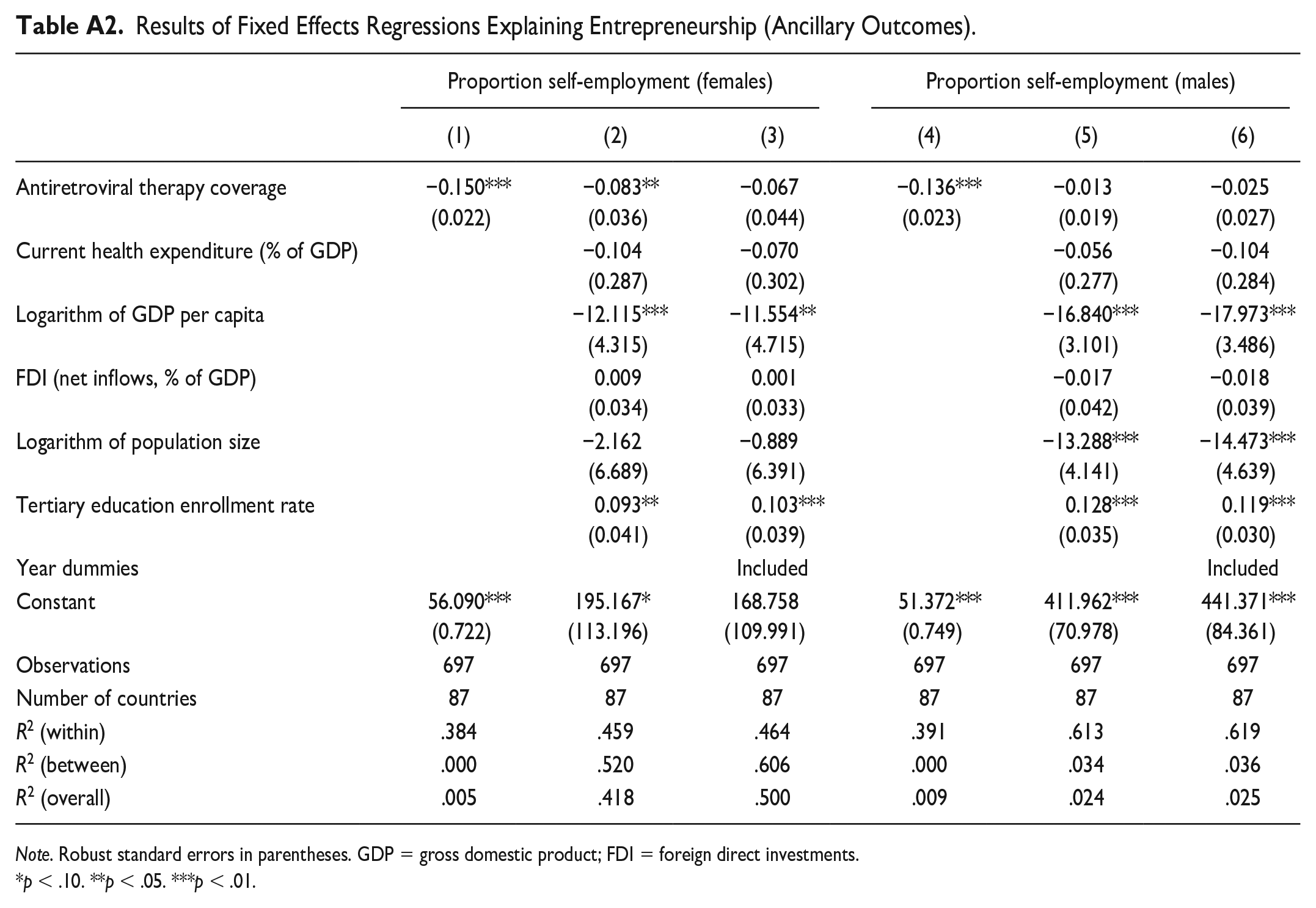
Table 3 contains the first set of empirical results. To address misspecification bias, we provide regression results for a model without control variables, a model with control variables, and a model with control variables and year dummies. In line with Hypothesis 1, we find that in Models 1 to 3, there is a significant positive relationship between ART coverage and the new business density measure. Effect sizes are relatively similar across these models; in Model 3, the most complete model, a 1% increase in ART coverage is associated with a 1.5% increase in the number of newly registered limited liability firms. Employing the incidence of HIV in the population (per 1,000 uninfected population) as the main explanatory variable leads to a similar conclusion: As expected, Table A1 in the appendix shows that there is a significant negative relationship between this variable and new business density (even though the analysis sample is somewhat smaller). In Model 4, we find a negative relationship between increased ART coverage and self-employment, but the inclusion of the control variables (Models 5 and 6) renders the ART coefficient insignificant. This relationship is also insignificant when we consider the proportion of self-employment among females and males separately (Table A2 in the appendix).
Results of Fixed Effects Regressions Explaining Entrepreneurship.
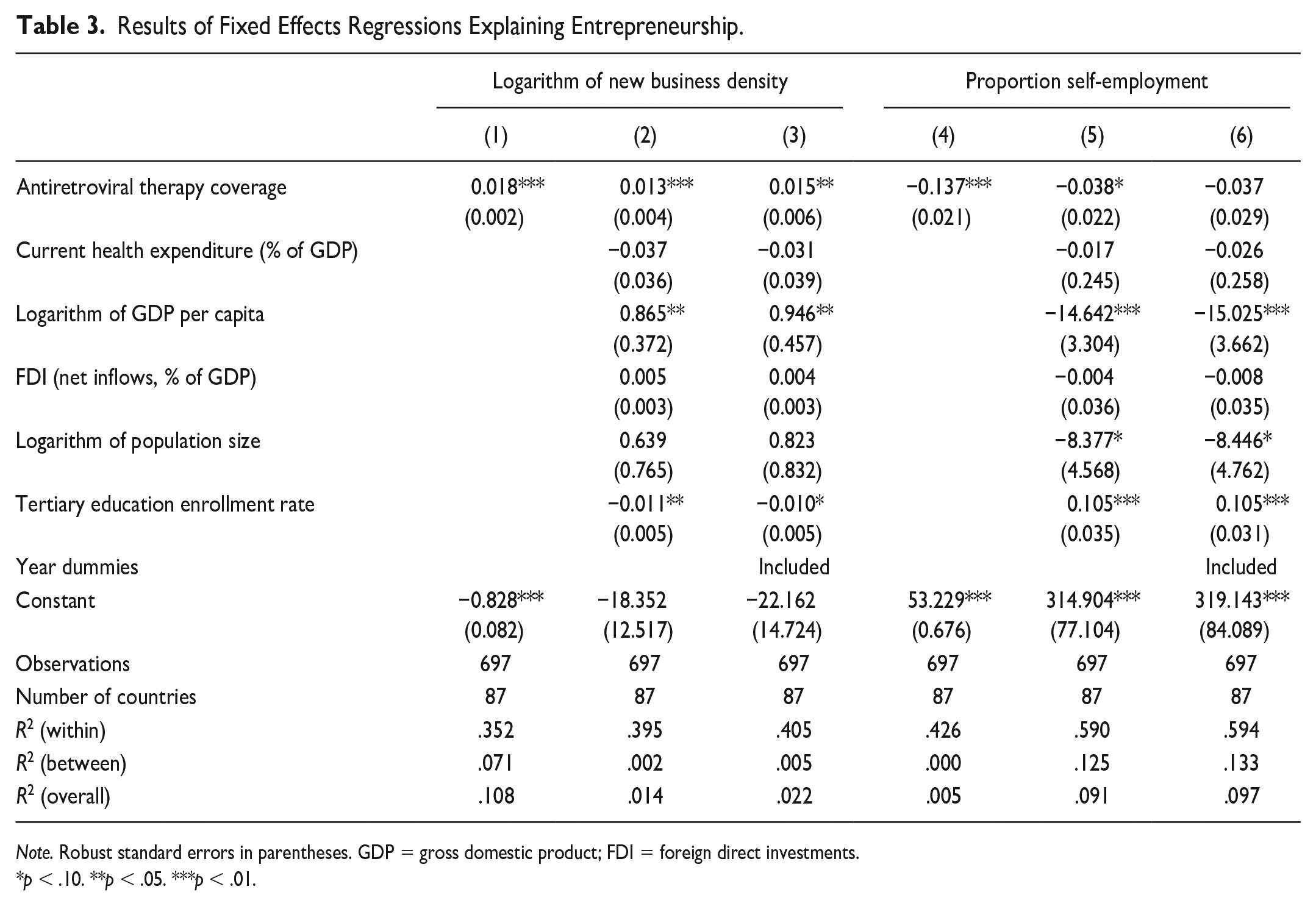
Note. Robust standard errors in parentheses. GDP = gross domestic product; FDI = foreign direct investments.
p < .10. **p < .05. ***p < .01.
Table 4 provides the main empirical results constituting our moderation analyses (Hypothesis 2). The table includes the results for the two outcome variables: GDP per capita and the HDI. The coefficients for ART coverage are positive in all models without interaction effects (Models 1, 3, 5, and 7), but only statistically significant in the HDI models. Regarding the entrepreneurship variables, we observe that all coefficients are significant in these four models with the number of new businesses being positively associated with development and the proportion of self-employment negatively associated with the two outcome measures. The interaction effects are significant in Models 2, 4, and 8. Due to the scale of measurement of the interaction variables, the point estimates seem small in Table 4. To assess the effect sizes, we therefore present the interaction effects in Figure 1. In the four subpanels, we focus on the slope and direction of the relationship in countries with the highest and lowest prevalence of the respective entrepreneurship measure.
Results of Fixed Effects Regressions Explaining Development (Moderation Analyses).
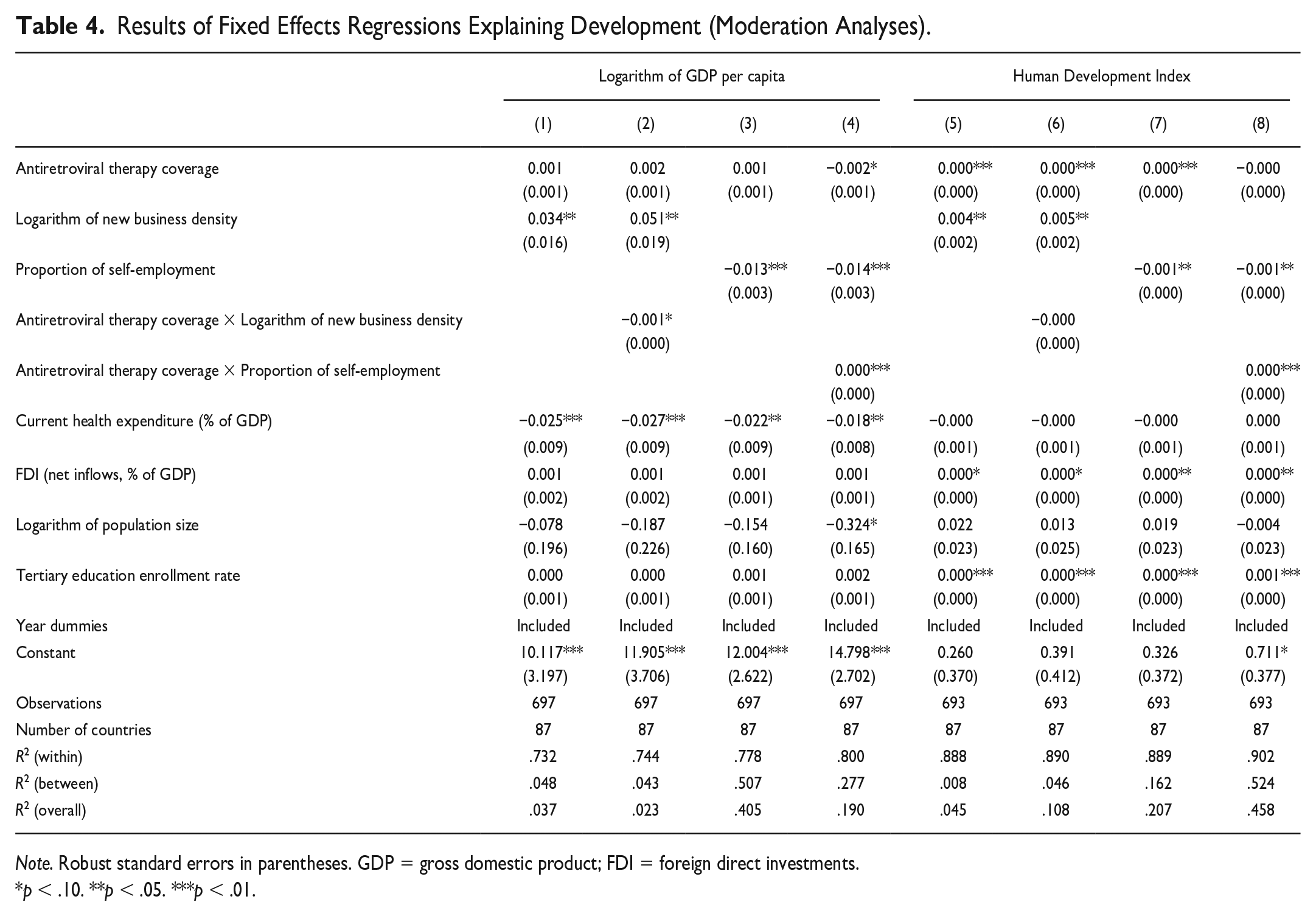
Note. Robust standard errors in parentheses. GDP = gross domestic product; FDI = foreign direct investments.
p < .10. **p < .05. ***p < .01.
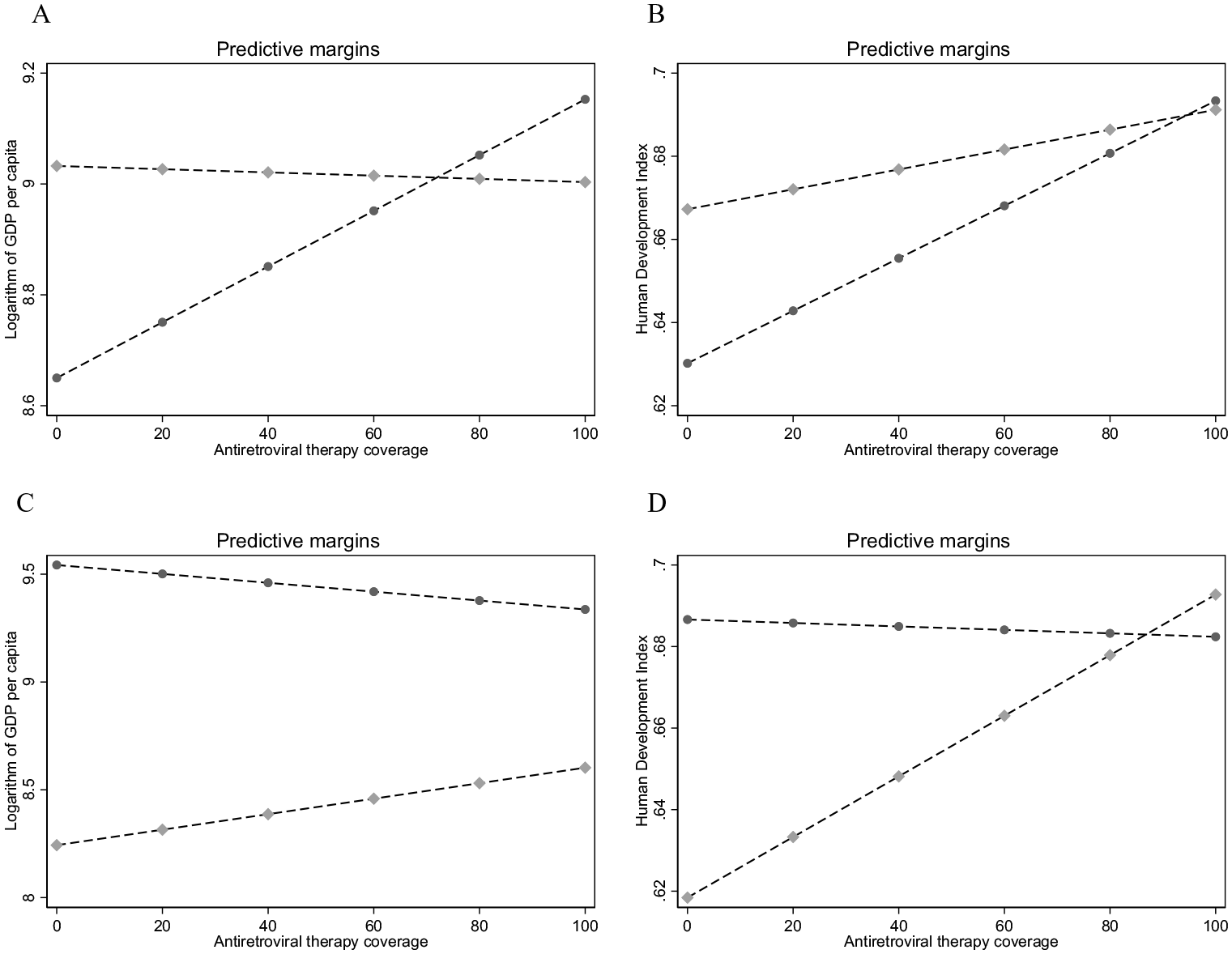
Interaction Plots Visualizing the Results of Fixed Effects Regressions Explaining Development (Table 4). The Dashed Line with Circles (Diamonds) Represents the Observed Minimum (Maximum) in the Analysis Sample (see Table 1) for the Respective Entrepreneurship Measure. (A) Logarithm of New Business Density. (B) Logarithm of New Business Density. (C) Proportion of Self-Employment. (D) Proportion of Self-Employment.
Results in light of Hypothesis 2 can be interpreted as follows. The moderation plot in the top left corner of Figure 1 (Panel A) suggests that the positive relationship between increasing ART coverage and GDP per capita holds mostly for countries with the lowest levels of new business density. In contrast, regarding the proportion of self-employment (Panel C), in countries with the lowest self-employment rates, we find a negative relationship between ART coverage and GDP per capita and a positive relationship in countries with the highest proportion of self-employment. Here, the marginal effects at higher proportions of self-employment are always below these at lower levels of self-employment. For the HDI (Panels B and D), we observe similar patterns, although the interaction between ART coverage and new business density does not significantly explain GDP per capita (Panel B, Model 6 in Table 4). In Panel D, the predicted HDI level in countries with the lowest and highest proportion of self-employment coincide at an ART coverage level of 72%. Thus, higher ART coverage seems especially effective for development in countries with low levels of new business formation and high proportions of self-employment.
In contrast to Panels A, C, and D of Figure 1, in Panel B we find a positive relationship between increasing ART coverage and the HDI irrespective of the level of new business formation. ART coverage may not only improve the distribution of entrepreneurial opportunities and creative destruction but also prime collective human capital lifted out of AIDS malaise improving the overall HDI. For example, organizations focusing on community development, education, and health care, although they might not generate substantial economic output that significantly influences GDP, can have a direct and meaningful impact on human development. Such aspects, often challenging to quantify in economic terms, may hold immense value for societal progress and well-being (i.e., the HDI) irrespective of the level of new business formation.
Discussion and Conclusion
In our sample of 87 low- and middle-income countries from the years 2006–2019, we find that ART coverage is positively associated with the number of newly registered limited liability firms but not significantly associated with the proportion of self-employment (supporting Hypothesis 1). While limited liability firms are relatively larger businesses than the typical businesses run by self-employed individuals, these results coincide with the conclusions of earlier individual-level studies indicating that good health enhances entrepreneurial ability and performance (Hatak & Zhou, 2019; Hessels et al., 2020) such that the average quality and size of businesses at country level increases with higher aggregate human capital (Van Praag & Van Stel, 2013).
Given the high prevalence of sustenance-based entrepreneurship in low- and middle-income countries (Global Entrepreneurship Monitor, 2020), lack of support for an association between ART coverage and self-employment may indicate that individuals with improved health seek and find traditional employment, a mode of living that provides relatively more stable wages (Lucas, 1978). Such employment might, for instance, be found in the newly established limited liability firms, and this dynamic may offset the positive individual-level selection into entrepreneurship also found in lower-income countries (Rietveld et al., 2016). Moreover, those with poorer health may undertake self-employment and due to limited human capital continue doing so after receiving ART. Future studies could parse out these alternate labor market dynamics for individuals with and without ART coverage. Due to the stigma associated with HIV and the chances of potential discrimination, we believe in particular qualitative studies could shed further light on labor market participation decisions for those receiving ART because self-reported individual-level data may be subject to reporting bias.
Related to Hypothesis 2, the improvements in GDP per capita and the HDI resulting from improvements in ART coverage are more salient in countries with lower levels of new business formation and high proportions of self-employment. While against Hypothesis 2 at first glance, these results align with ART coverage leading increased levels of entrepreneurial quality. When people are healthy, they are more productive and can contribute more to their communities and economies. Following Lucas (1978), they engage less often in necessity-based self-employment but rather opt for more stable income as workers in a large formalized business. With increasing ART coverage, countries with low new business formation can improve the quality of life for their population, leading to better health and well-being. In contrast, countries with high levels of new business formation may not benefit as much from increased ART coverage and development, as they may already have well-developed health care systems and infrastructure in place. In addition, these countries may have more resources and capacity to address the social and economic determinants of health, which can also impact health outcomes. Therefore, the notion that countries with low new business formation benefit the most from high ART coverage is a plausible one, albeit that marginal effects are small.
It is important to note that the results in our study should be understood as associational rather than causal. When outcomes are observed only after an event, establishing a causal relationship between the treatment and outcomes can be challenging due to potential endogeneity, including omitted variable biases. The diffusion process of health interventions across a country involves various stages, including awareness, acceptance, adoption, and implementation, making it challenging to fully deal with these potential biases. In our study, we accounted for potential confounding factors and conducted robustness checks to enhance the interpretation of the effects. Moreover, acknowledging boundary conditions of our study, we focus on examining the relationship between improvements in health capital and the moderating effect of entrepreneurial activity within the context of low- and middle-income countries. We have selected a specific group of countries to understand the dynamics of entrepreneurship in environments where economic and health care challenges are particularly prevalent. While our research primarily investigates the impact of ART coverage on entrepreneurship, the boundary conditions of our theory may constrain the generalizability of our findings to different health issues or interventions or developing countries with significantly different HIV prevalence profiles after the fall of ART drug prices. Overall, the boundary conditions of our theory are contingent upon the nature of the health intervention, the specific country context, and the focus on formal entrepreneurial activity.
The present study expands the existing literature about health and entrepreneurship in three important ways. First, we focus on health and entrepreneurship associations in low- and middle-income countries, a currently underresearched space in the literature. The large disparities in health as well as the nature of necessity-driven entrepreneurship in these countries make it important to add to the few studies analyzing this relationship in developing countries (Djankov et al., 2005; E. Nikolova et al., 2012; Rietveld et al., 2015). Second, we provide country-level evidence about the relationship between health and entrepreneurship rather than individual-level evidence. As health policies and health care systems are developed at the country level, our study adopts a particularly policy-relevant unit of analysis. Third, we provide evidence about the relationship between health and entrepreneurship by exploiting steep decreases in antiretroviral drug prices and the subsequent increases in ART coverage and general health in low-income countries. Where Tompsett (2020) shows that ART coverage expansion led to growth in GDP per capita, we analyze whether entrepreneurship amplifies such effects on the development of a low- or middle-income country.
Our study also falls squarely into the paramount challenge that requires concerted efforts from various sectors, including entrepreneurship as a driver of economic growth in meeting the grand challenges (Park et al., 2022). The 2030 United Nations’ Sustainable Development Goals (SDGs) explicitly recognize the significance of health as a grand challenge and emphasize the need for collaborative action to address it. While research on the relationship between business and health has primarily focused on areas like occupational health, health care organizations, and health regulations, the impact of macro-level improvements in health on entrepreneurial activity is also an important consideration for policymakers. Through our study, we aspire to contribute to an interdisciplinary approach that bridges the gap between business and public health research. By elucidating how business activities intersect with health, we aim to provide valuable insights and recommendations for scholars interested in advancing the 2030 Agenda and the SDGs related to health and well-being. By exploring this vital intersection, we seek to generate knowledge that can inform evidence-based practices and policies, ultimately fostering improved health and other outcomes for individuals, communities, and society as a whole.
Our findings also have limitations. First, the nature and effectiveness of the health intervention itself can play a significant role. In our study, we have focused on ART coverage as a specific health intervention aimed at addressing the HIV/AIDS epidemic. Therefore, the applicability of our findings to other health issues or interventions may differ, as the mechanisms linking health capital and entrepreneurship can vary across different health care contexts. Second, the broader socioeconomic and cultural contexts of low- and middle-income countries need to be considered. Factors such as economic conditions, institutional environments, social norms, and access to health care can shape the relationship between health capital and entrepreneurship within specific country contexts. Third, we acknowledge that our study focuses on formalized new business registrations and self-employment as measures of entrepreneurial activity. This choice of outcome variables sets a specific boundary condition, limiting our analysis to the formal sector of the economy. Informal entrepreneurship and other forms of entrepreneurial activity, which may be influenced by different factors and exhibit distinct relationships with health capital, are beyond the scope of our study. We acknowledge the need for further research to explore the boundary conditions and generalizability of our findings to different health issues, diverse developing country contexts, and a broader range of entrepreneurial activities.
Nevertheless, within these boundary conditions, we present relevant findings regarding the interplay between health and entrepreneurial activity in low- and middle-income countries. These results resonate with the urgent call articulated by Park and colleagues (2022) for deeper explorations of the role of businesses in addressing significant health challenges and achieving the ambitious SDGs set by the United Nations. Through our study, we make a contribution to the theoretical framework by shedding light on the relationship between health and entrepreneurship among others by delving into an important distinction within entrepreneurial activity: While the link between ART coverage and limited liability firms is statistically significant, we observe no such relationship with self-employment. The empirical evidence we present thus underscores the impact of health on formalized entrepreneurial activity with high impact (Henrekson & Sanandaji, 2020). These findings demonstrate the transformative potential of accessible health care in fostering vibrant business ecosystems and reveal health as a potential driver of entrepreneurial activity.
Building upon the theoretical positioning presented by Park and colleagues (2022), our study thus serves as a tangible bridge between the domains of business and public health. By merging the disciplines of business and public health, we inform policy interventions that foster entrepreneurship as a catalyst for both economic growth and the advancement of population health, and an impeller in meeting the “grand challenge of human health.” That is, by providing empirical support for the positive impact of ART coverage on formalized new business registrations and acknowledging the importance of these for economic development (Carree & Thurik, 2010; Van Praag & Versloot, 2007), our findings may also inspire future studies analyzing the conditions under which businesses articulate, engage, and implement multilevel actions affecting the health outcomes of external stakeholders, such as customers and local communities. In doing so, the insignificant results we find for the relationship between ART coverage and self-employment may prompt both scholars and policymakers to recognize the diverse manifestations of entrepreneurship in tailoring studies and interventions.
Building upon these findings, future research could delve into the mechanisms through which increased ART coverage facilitates the growth of new businesses in contexts characterized by low levels of new business formation and higher proportions of self-employment. Future studies could encompass several dimensions. Better health outcomes could translate into increased participation in skill development and training programs, ultimately boosting the overall human capital of the country. Studies can also investigate how higher ART coverage correlates with new businesses attracting the resulting pool of higher skilled and more capable employees. Determining whether healthier entrepreneurs, with better access to treatment, are more inclined to pursue innovative strategies and create value-added enterprises is worth examination. At the macroeconomic level, the interaction between higher ART coverage and increased new business formation could impact the broader labor market by shifting employment patterns, with a potential movement of workers from traditional sectors to new and more productive ventures. Investigating the long-term socioeconomic effects of improved health conditions in terms of upward mobility, poverty reduction, and enhanced quality of life, thereby driving sustainable economic development is also an important consideration for future studies.
In conclusion, the nuanced relationship between entrepreneurship, ART coverage, GDP per capita, and the HDI underscores the multifaceted nature of entrepreneurship’s impact on development. While its effects on economic growth might take time to materialize, entrepreneurship’s moderating influence on development components highlights its potential to drive holistic societal advancement. Our results also underscore the need to assess development outcomes comprehensively, taking into account both economic and noneconomic dimensions of progress.
Footnotes
Appendix
Results of Fixed Effects Regressions Explaining Entrepreneurship (Ancillary Outcomes).
| Proportion self-employment (females) | Proportion self-employment (males) | |||||
|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | |
| Antiretroviral therapy coverage | −0.150***
(0.022) |
−0.083**
(0.036) |
−0.067 (0.044) |
−0.136***
(0.023) |
−0.013 (0.019) |
−0.025 (0.027) |
| Current health expenditure (% of GDP) | −0.104 |
−0.070 |
−0.056 |
−0.104 |
||
| Logarithm of GDP per capita | −12.115***
|
−11.554**
|
−16.840***
|
−17.973***
|
||
| FDI (net inflows, % of GDP) | 0.009 |
0.001 |
−0.017 |
−0.018 |
||
| Logarithm of population size | −2.162 |
−0.889 |
−13.288***
|
−14.473***
|
||
| Tertiary education enrollment rate | 0.093**
|
0.103***
|
0.128***
|
0.119***
|
||
| Year dummies | Included | Included | ||||
| Constant | 56.090***
|
195.167*
|
168.758 |
51.372***
|
411.962***
|
441.371***
|
| Observations | 697 | 697 | 697 | 697 | 697 | 697 |
| Number of countries | 87 | 87 | 87 | 87 | 87 | 87 |
| R2 (within) | .384 | .459 | .464 | .391 | .613 | .619 |
| R2 (between) | .000 | .520 | .606 | .000 | .034 | .036 |
| R2 (overall) | .005 | .418 | .500 | .009 | .024 | .025 |
Note. Robust standard errors in parentheses. GDP = gross domestic product; FDI = foreign direct investments.
p < .10. **p < .05. ***p < .01.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.