
Abstract
Given the escalating concern surrounding mental health issues among school-age children, this study evaluated the benefits, feasibility, and acceptability of the Open Parachute mental health literacy program, designed to foster mental health skills through classroom instruction. This study asked 37 Australian educators, spanning primary to secondary school, to report on their experiences with the Open Parachute program. 50 percent of participants reported the program improved student mental health literacy and support skills, with 89% of educators intending to use the program again and 92% reporting they would recommend it to a colleague, demonstrating high feasibility and acceptability. Educators reported that they observed greater skill use, and gains in emotional regulation and empathy, in primary students compared to secondary school students. The findings of this study provide preliminary evidence for the utility of the Open Parachute program and the potential benefits of universal early mental health literacy instruction in school.
Keywords
Introduction
Child and youth mental health has garnered significant attention in public and academic domains, driven by reports of a continuing decline in child mental wellbeing, exacerbated by the COVID-19 pandemic (Biddle & Gray, 2021; Kauhanen et al., 2023; Madigan et al., 2023). Australian adolescents have expressed significant worries about managing their stress and wellbeing, highlighting the pandemic’s impact on education, mental health, and social isolation as major concerns (Tiller et al., 2020). Worldwide, there is a gap between the demand for mental health services and their accessibility and utilisation across all age groups, influenced by various hindering factors such as constrained resources or insufficient mental health awareness (Malti & Noam, 2008; Wainberg et al., 2017). Amidst the current complexities of modern life (e.g. post-pandemic recovery, climate concerns, and living in a digital era), the significance of mental health literacy for children cannot be overstated.
Mental health literacy refers to the knowledge, beliefs, and abilities that enable individuals to recognise, understand, and effectively respond to mental health concerns and related issues (Jorm et al., 1997). It encompasses various aspects, including understanding the signs and symptoms of mental health conditions, knowing how and where to seek help, reducing the stigma associated with mental illness, and promoting positive mental health and wellbeing practices. Essentially, mental health literacy empowers individuals to make informed decisions about their own mental health and to support others who may be experiencing mental health challenges (Jorm, 2000).
Given that core social-emotional competencies such as empathy, self-regulation, and problem-solving develop significantly across childhood and adolescence (Dorris et al., 2022; Laureys et al., 2022; Xu et al., 2013), it is important to understand how mental health literacy is acquired and expressed at different stages of development. This developmental perspective is essential for designing and evaluating programs like Open Parachute, which aim to promote mental health in both primary and secondary school students.
Using a universal approach, the education system is poised as an ideal environment to deliver mental health literacy to children and adolescents and address the growing mental health challenges faced by today’s youth (Vamos et al., 2020; Whitley et al., 2013). Schools are uniquely positioned to offer mental health literacy not only early in life but also intensively over the course of child development, allowing access to a broad range of students from all backgrounds (Morrison & Peterson, 2013; Seligman et al., 2009). Focussing on mental health literacy within school settings holds promise for fostering enduring positive outcomes in mental, social, and behavioural growth (Ekornes, 2020; Graham et al., 2011; Grové & Laletas, 2020). By equipping a generation with the knowledge and skills to navigate their psychological health, we not only bolster individual wellbeing but also lay the groundwork for healthier communities.
Mental health literacy has become increasingly recognised as an essential component of education in Australia (Marinucci et al., 2022), garnering greater dialogue and attention from parents, teachers, and policymakers. While not explicitly mandated in the national curriculum, several initiatives, resources, and guidelines have been developed to promote wellbeing for children and youth in schools across the country (Australian Government Department of Education, 2023). Given the many competing priorities and time limitations for teachers and school leaders, it is important to prioritise and adopt evidence-based curriculum strategies that are not only effective but also feasible to implement. Moreover, these approaches to addressing child wellbeing and mental health literacy should be practical for teachers to deliver, mindful of their workload constraints and avoiding overburdening them with additional responsibilities.
Given the emphasis on teaching mental health literacy in the education system, educators often bear the responsibility of integrating instruction on mental health topics into their regular classroom instruction. While, in theory, this seems like the best approach to implementation, many Australian teachers report feeling that their training does not equip them to competently deliver mental health literacy, and that other allied health professionals (e.g. psychologists, counsellors, and art therapists) are better trained in this area (Marinucci et al., 2023).
One way to address this concern is to use innovative school-based mental health literacy programs, grounded in clinical psychology, to serve as a platform for nurturing mental health competencies (e.g. emotion regulation, peer communication, and coping skills) through interactive and reflective exploration of mental health-related subjects. These programs are designed to reduce the burden of instructing in these areas on teachers.
The Open Parachute program was designed with these limitations in mind. As described below, the Open Parachute program aims to empower teachers by allowing them to aid in the administration of the curated curriculum content and oversee program delivery without bearing the responsibility of acting as an expert in the content area.
The Open Parachute program is a universal school-based curriculum that teaches mental health literacy skills at a developmentally appropriate level to children and adolescents from Foundation (the first year of formal schooling) to Year 12. The program contains pre-prepared lessons featuring documentary videos showcasing real students sharing their experiences of overcoming struggles, inspiring students to build resilience in their own lives. Open Parachute utilises clinically validated, research-based psychological skill-building exercises, such as class discussions, partner exercises, and journaling to boost resilience, self-awareness, and social responsibility in young people. Simultaneously, it helps increase their connection and systems of support. The variety of teaching modalities (e.g. video instruction, class discussions, partner exercises, and journaling) not only offers diverse avenues and opportunities to consolidate student learning and skill development but also considers the distinct developmental stages of youth, tailoring the program (e.g. videos showcase children of different ages based on year level and verbal content is tailored to age) to align with the varying levels and capabilities of students across different year levels.
As curriculum content is delivered by peers and clinical psychologists via documentary videos, the Open Parachute program curriculum is designed to be supervised by teachers without requiring them to deliver the key content themselves. This differs from the usual models of mental health content delivery in school settings, which involve training teachers to learn and convey mental health literacy content and skills to students (Franklin et al., 2012; Jones & Bouffard, 2012). Further, by providing core content via video, the Open Parachute model of delivery may be more acceptable to teachers for whom additional training may not be feasible given current workloads, and who may vary in their familiarity and comfort with teaching and discussing mental health literacy with students. The video format and pre-prepared skill-building exercises can also help build teacher confidence in coping with student mental health challenges, providing a framework for responding to students and creates a common skill base for students to manage their own mental health. The video format and pre-prepared lesson content also support standardised delivery across classrooms.
The Current Study
The primary goal of this study was to investigate educators’ experiences with implementing the Open Parachute program. Specifically, the study aimed to: (1) evaluate whether South Australian teachers perceive the program to have benefits for themselves and their students, (2) explore whether educators’ responses vary based on their educational setting (primary versus secondary school contexts), (3) investigate feasibility and fidelity when delivering the program in full, and (4) assess the acceptability of the program from the educators’ perspective.
Methodology
Recruitment Process
Participants were recruited via convenience sampling from a group of Year 2 to 12 teachers and school leaders (e.g. principals, deputy principals, and leadership staff) in government sector schools that delivered the Open Parachute program in South Australia, Australia. Information regarding the study was sent to a contact in the school leadership team (e.g. Head of Wellbeing or Wellbeing Leader) at 30 schools who had delivered the Open Parachute program during the 2022–2023 academic year. All schools had agreed to be contacted to provide feedback on the Open Parachute program when they elected to deliver the program in their schools. 1
The lead school contact was asked to distribute the study information to all teachers and school leaders involved in delivering the program. Of the 30 schools contacted, 15 schools confirmed the distribution of study recruitment materials, and 13 schools participated in this study. Participation at the school and educator level was voluntary and did not impact enrolment in the Open Parachute program or access to Open Parachute resources. The participating schools were mainly located in Adelaide with two schools located in the surrounding areas. After responding to the study recruitment materials and providing consent, teachers and school leaders were sent an online survey. . Participants were sent the survey at the end of the academic year and post-intervention, November 2023 to January 2024. Participants were provided with two tickets to an Australian Football League game as a token of appreciation. This study was approved by the University of Calgary Conjoint Faculties Research Ethics Board (REB23-0722) and followed the recommendations for international research outlined by the Australian Government, in collaboration with the National Health and Medical Research Council, Australian Research Council and Universities Australia (2023).
Participants
Demographics of Respondents
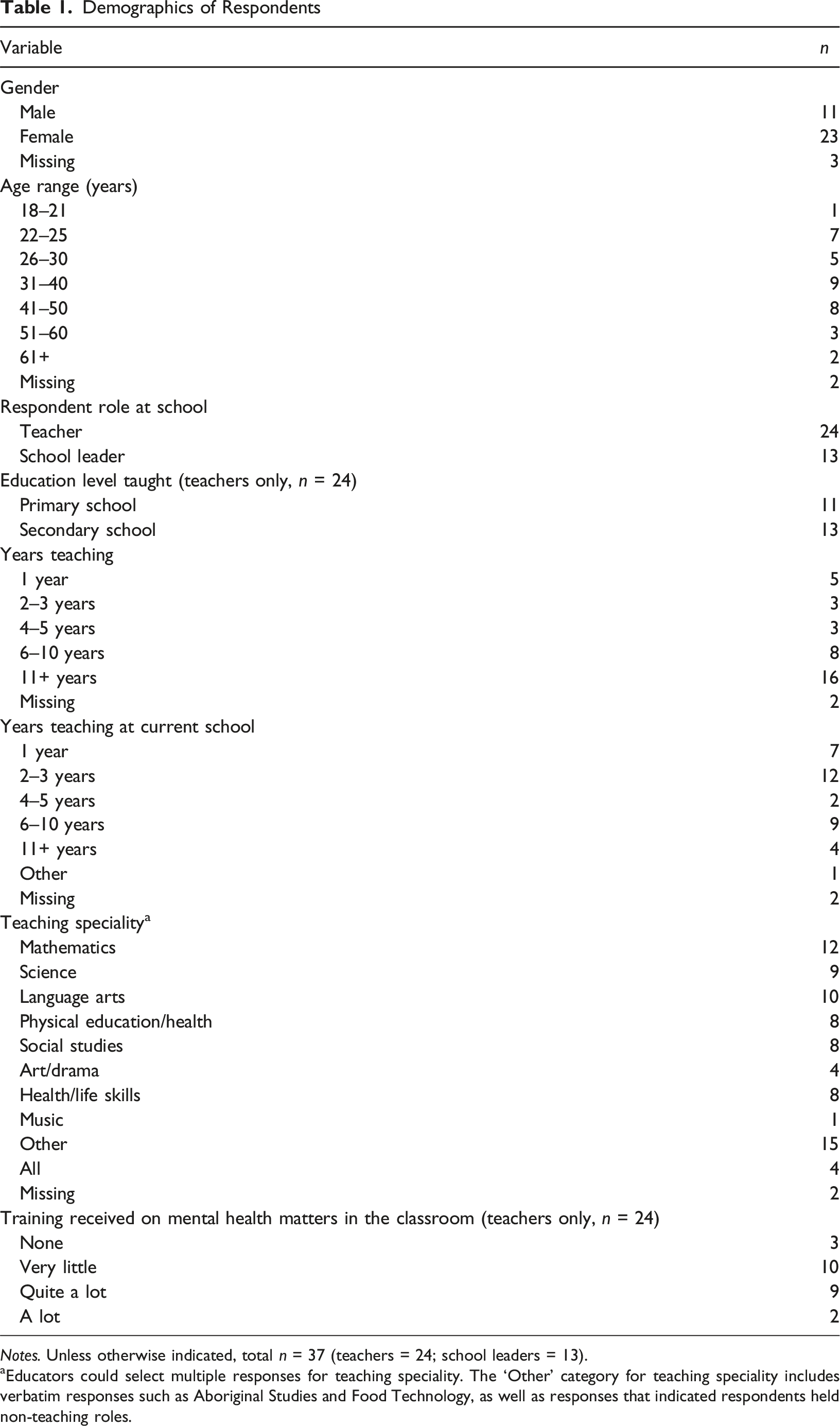
Notes. Unless otherwise indicated, total n = 37 (teachers = 24; school leaders = 13).
aEducators could select multiple responses for teaching speciality. The ‘Other’ category for teaching speciality includes verbatim responses such as Aboriginal Studies and Food Technology, as well as responses that indicated respondents held non-teaching roles.
Intervention
The Open Parachute program was developed by a team of clinical psychologists and educators, led by Dr Hayley Watson, a clinical psychologist specialising in children and adolescents, and Bridget Kamp, an experienced classroom teacher with two decades of teaching experience in various educational contexts, including public, international, and alternative schools.
The development of the program was grounded in evidence-based psychological frameworks, including Cognitive Behavioural Therapy (CBT), Dialectical Behaviour Therapy (DBT), Acceptance and Commitment Therapy (ACT), Mindfulness-Based Stress Reduction (MBSR), and Narrative Therapy. These frameworks were chosen based on their strong empirical support for promoting mental health and emotional wellbeing in young people (Beaudoin et al., 2016; Hayes et al., 2006; James et al., 2020; Rathus & Miller, 2015; Vohra et al., 2019). The program’s content was designed with developmental psychological principles in mind, ensuring that the materials and activities were age-appropriate and aligned with the cognitive and emotional needs of students at various stages of development.
The program was first launched in 2018 across Canadian, American, and Australian schools. Based on informal feedback, positive impacts on students were reported, and feedback was collected from both students and teachers to inform further refinement of the program. Since then, the program has undergone repeated internal pilot testing across schools in these three countries, with ongoing adjustments made based on the feedback from teachers, students, and school leaders (McArthur, 2024; McArthur et al., 2024). Currently, the program is being delivered to approximately 300,000 students annually worldwide. Each year, the team incorporates new feedback from end-users to enhance the accessibility and feasibility of the program materials.
The Open Parachute program is offered to schools through the South Australian Department of Education’s approved wellbeing program list. Schools select the program as part of their internal review process, and they are provided with the option to trial the program before committing to full implementation. Schools that choose to implement the program receive training for their staff and ongoing support from the Open Parachute team throughout the academic year.
For the current study, the Open Parachute intervention consisted of approximately 30 classes, each lasting 12 to 35 minutes delivered weekly or bi-weekly (depending on the scheduling needs of each school). The classes comprise overarching unit topics (e.g. Worries, Anxiety & Resilience; Bullying & Addictive Patterns; Overcoming Challenges; Self-Esteem; Understanding Mental Health; Self-Image & Stereotypes), with seven topics for Year 2 through Year 9, eight topics for Year 10, six topics for Year 11, and five topics for Year 12. The format of each lesson was as follows: (1) students were introduced to the lesson topic (e.g. ‘How can I help myself with negative thoughts’) and are provided with vocabulary if required; (2) students were shown a video of a peer sharing a personal story related to the lesson content, that also features psychoeducation from a clinical psychologist on the topic area; (3) students engaged in skill-building exercises supervised by their teacher; (4) students in Year 4 through 12 completed an ‘exit ticket’, a brief quiz to determine their level of learning from the lesson. The exit tickets were designed to help teachers understand which concepts may need further follow-up. Not all teachers choose to provide exit tickets to their students.
Measures
Demographics
Educators were asked to report on their: (1) gender (male, female, self-identify as (please specify), and prefer not to answer), (2) age range (1 – 18–21 to 7 – 61 or older), (3) the number of years they have been actively teaching (1 – 1 year to 5 – 11+ years) , (4) years of employment at their current school (1 – 1 year to 5 – 11+ years), (5) area of teaching speciality, (6) the year level they taught (later grouped as primary or secondary), and (7) how much training they have received on mental health matters in the classroom, either in initial teacher education and/or ongoing professional development (1 – none to 4 – a lot).
A large number of educators (16) had taught for more than 11 years, with 8 teaching 6–10 years, 3 teaching 4–5 years and 2–3 years, respectively, and 5 teaching for 1 year. Prior to the intervention, over half of the teachers (13) reported having little prior training on mental health matters in the classroom (see Table 1).
Perceived Benefits of Open Parachute to Educators
To gather information on the perceived benefits of the Open Parachute program for teachers, educators were asked to report on a 5-point Likert scale (1 – not at all to 5 – a lot): (1) if after completing the Open Parachute program they were more interested in learning about mental health in a school setting, (2) if they thought other teachers at their school were more interested in learning about mental health in a school setting, (3) if the program improved their understanding of youth mental health challenges, (4) if they experienced greater connection to their students, (5) if they felt more self-aware about their own thoughts and actions, (6) if they felt the program improved their knowledge and skills in the area of mental health literacy, (7) if they felt the program improved their comfort level when discussing mental health topics in the classroom, (8) if they felt the program improved their confidence in supporting students, (9) if they felt the program helped them identify challenges that students were facing, (10) if they felt that the program helped them resolve student disruptions/disagreements more easily in class, and (11) if they felt the program helped them with classroom management of student behaviour.
Perceived Benefits of Open Parachute to Students
To gather information on the perceived benefits of the Open Parachute program for students, educators were asked to report on a 5-point Likert scale (1 – not at all to 5 – a lot): (1) if they saw their students use the skills they learned in the Open Parachute program, (2) if their students were better able to communicate with peers/adults, (3) better able to soothe their own emotions, (4) better able to problem-solve personal/peer/school-related challenges, (5) more self-aware about their own thoughts and actions, (6) showed more empathy for others, and (7) showed more skills to support their mental health. Lastly, educators were asked if they thought the Open Parachute program benefited students (0 – not at all to 10 – very much).
Feasibility and Program Fidelity for the Open Parachute Program
With regards to the administration of the Open Parachute program over the course of the academic year, teachers were asked to report on: (1) on average how much time they spent preparing for the Open Parachute lessons (1 – 5 to 10 minutes to 5 – more than 30 minutes), (2) how prepared they felt to run the Open Parachute program (1 – not at all to 5 – a lot), (3) how closely they followed the exercises in each Open Parachute lesson (1 – not at all to 5 – a lot), (4) whether they omitted any units (1 – yes to 2 – no), and (5) if they omitted units, what units they omitted.
Acceptability of the Open Parachute Program
To measure the acceptability of the program, educators were asked to report on: (1) whether running the Open Parachute program helped them/their team in their role as a teacher (1 – not at all to 5 – a lot), (2) how likely they would be to recommend the Open Parachute program to a colleague (0 – I would not recommend this program to 10 – I would definitely recommend this program), and (3) if they thought the Open Parachute program would have a greater impact if students could complete it again next year (1 – not at all to 5 – a lot).
In addition to the self-developed items designed to assess acceptability of the Open Parachute program, and consistent with other studies evaluating school-based interventions (Emonson et al., 2022), eight items (e.g. ‘The open parachute program… fits well within the daily school routine’) were adapted from the Toybox-study (Androutsos et al., 2014; Manios et al., 2014) to assess educators’ perceptions of the Open Parachute program experience and implementation (see Table 5 for these items). Educators indicated on a 5-point Likert scale how much they agreed with each statement (1 – strongly disagree to 5 – strongly agree). Each item was interpreted independently based on descriptive data.
Data Analysis
Descriptive statistics were used to explore sample demographics and intervention feasibility and acceptability. Independent samples t-tests were used to compare primary school (Years 2–6) and secondary school (Years 7–12) results. Effect sizes were calculated using Cohen’s d and interpreted with standard cut-offs (<0.20 – very small; 0.20–0.49 – small; 0.50–0.79 – medium; >0.80 – large; [Cohen, 1988]). All analyses were conducted using SPSS v.29 (IBM Corp, 2022).
Results
Perceived Benefits of Open Parachute to Educators
After completing the Open Parachute program, 31 teachers and school leaders were interested in learning more about mental health in a school setting, with only 4 indicating ‘a little’ and 2 indicating ‘not at all’. All respondents (37) indicated that after implementing the Open Parachute program, they believed other teachers at their school were more interested in learning about mental health in a school setting, with responses ranging from ‘a little’ to ‘a lot’.
Perceived Benefits of the Open Parachute Program for Teachers, Classroom Teachers’, and School Leaders’ Responses
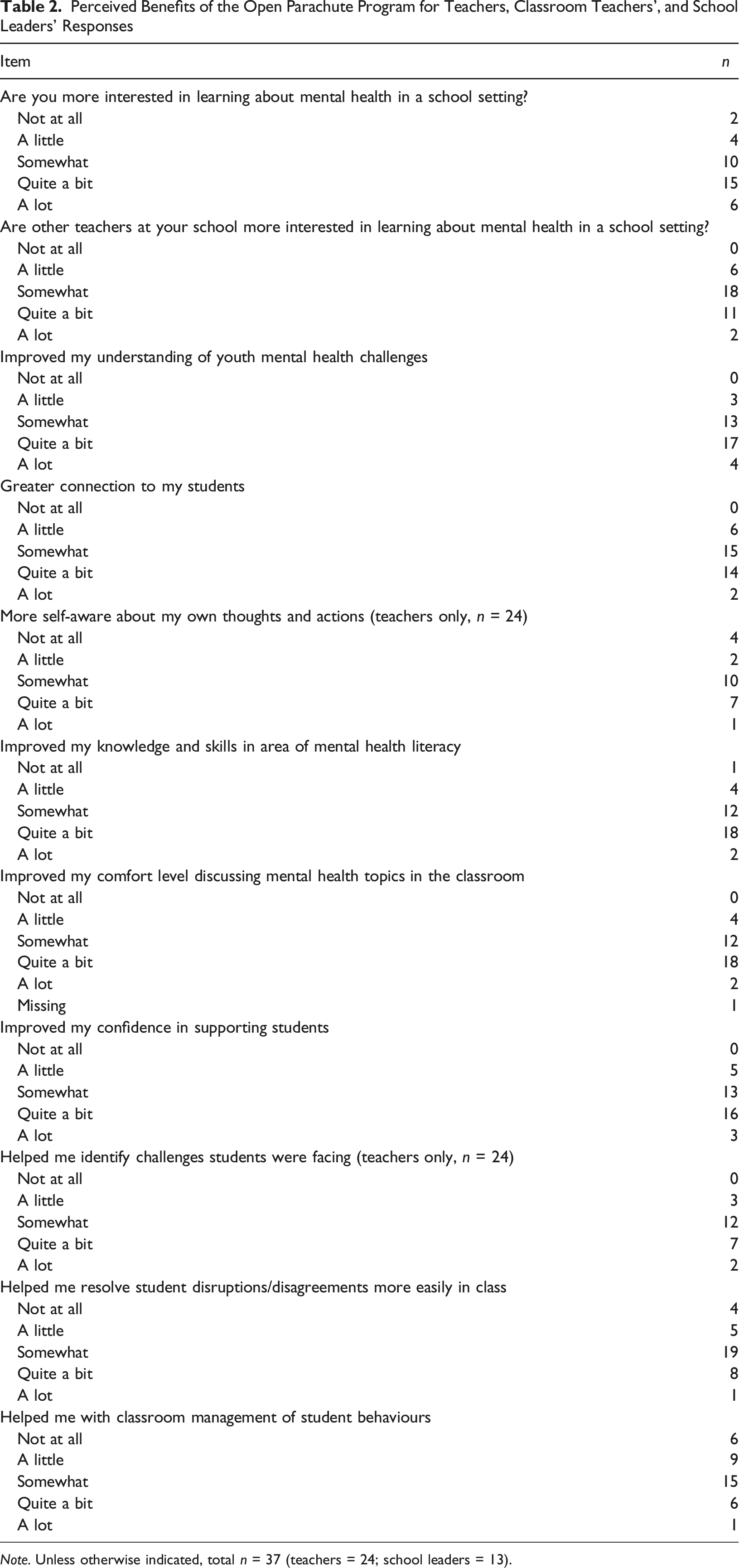
Note. Unless otherwise indicated, total n = 37 (teachers = 24; school leaders = 13).
An analysis of the relationships between demographic factors and educator benefits found an inverse relationship between years of active teaching experience and increased connection to students (r = −.470, p = .027), and improved comfort level when discussing mental health topics in the classroom (r = −.604, p = .003) after delivering the Open Parachute program. These findings suggest the Open Parachute program was more beneficial to educators who are earlier in their career.
Perceived Benefits of Open Parachute to Students
When asked to rate how much they thought the program benefited students on a scale from 0, ‘not at all’ to 10, ‘very much’, teachers and school leaders provided individual scores that resulted in an average rating of 7.59 (SD = 1.50), suggesting strong endorsement of the program. Overall, 30 teachers reported observing students using the skills they learned in the Open Parachute program, ‘somewhat’ or ‘quite a bit’.
Perceived Benefits of the Open Parachute Program for Students, Classroom Teachers’, and School Leaders’ Responses
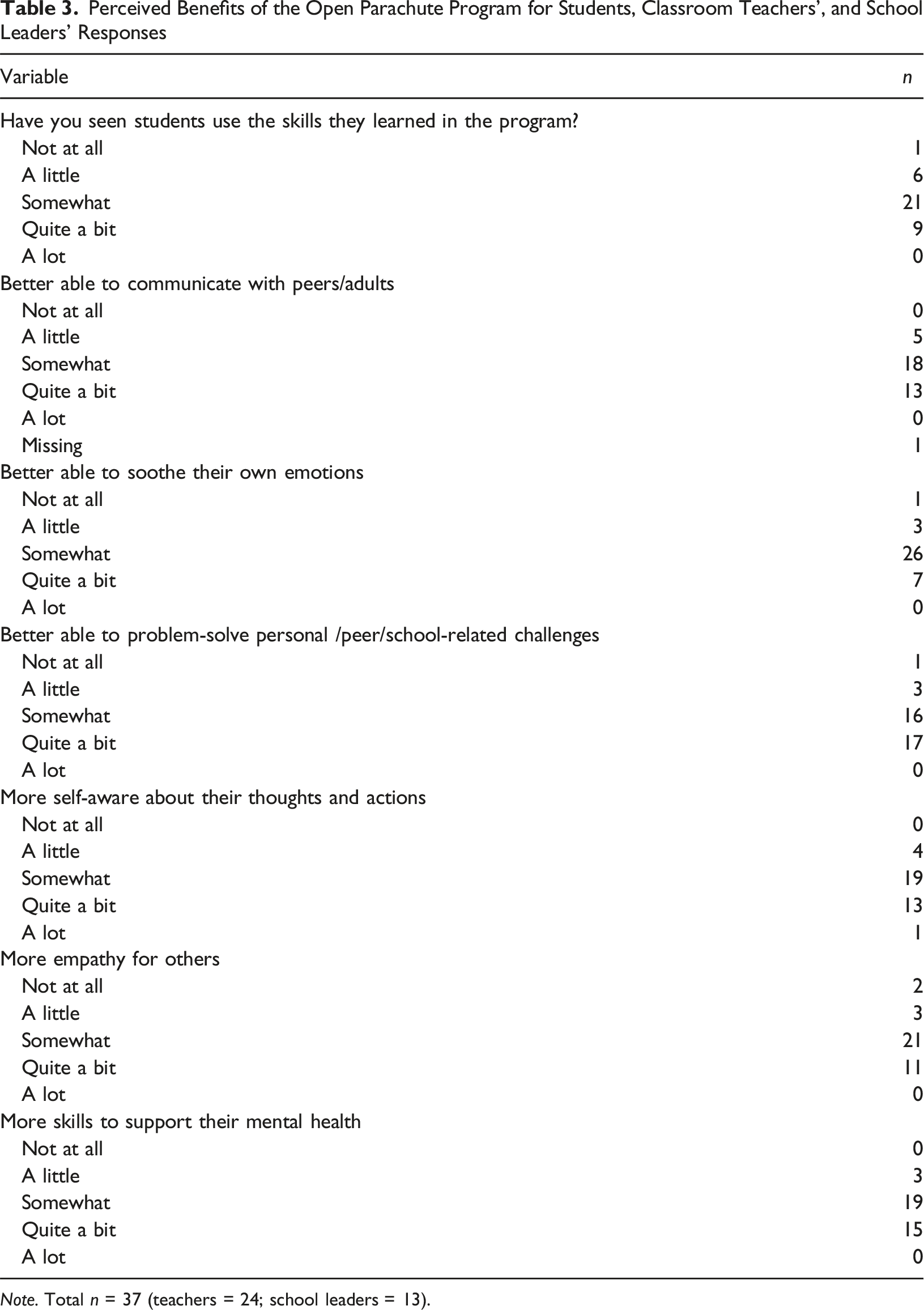
Note. Total n = 37 (teachers = 24; school leaders = 13).
Perceived Benefits of the Open Parachute Program for Students, Comparison of Average Responses of Primary and Secondary Classroom Teachers
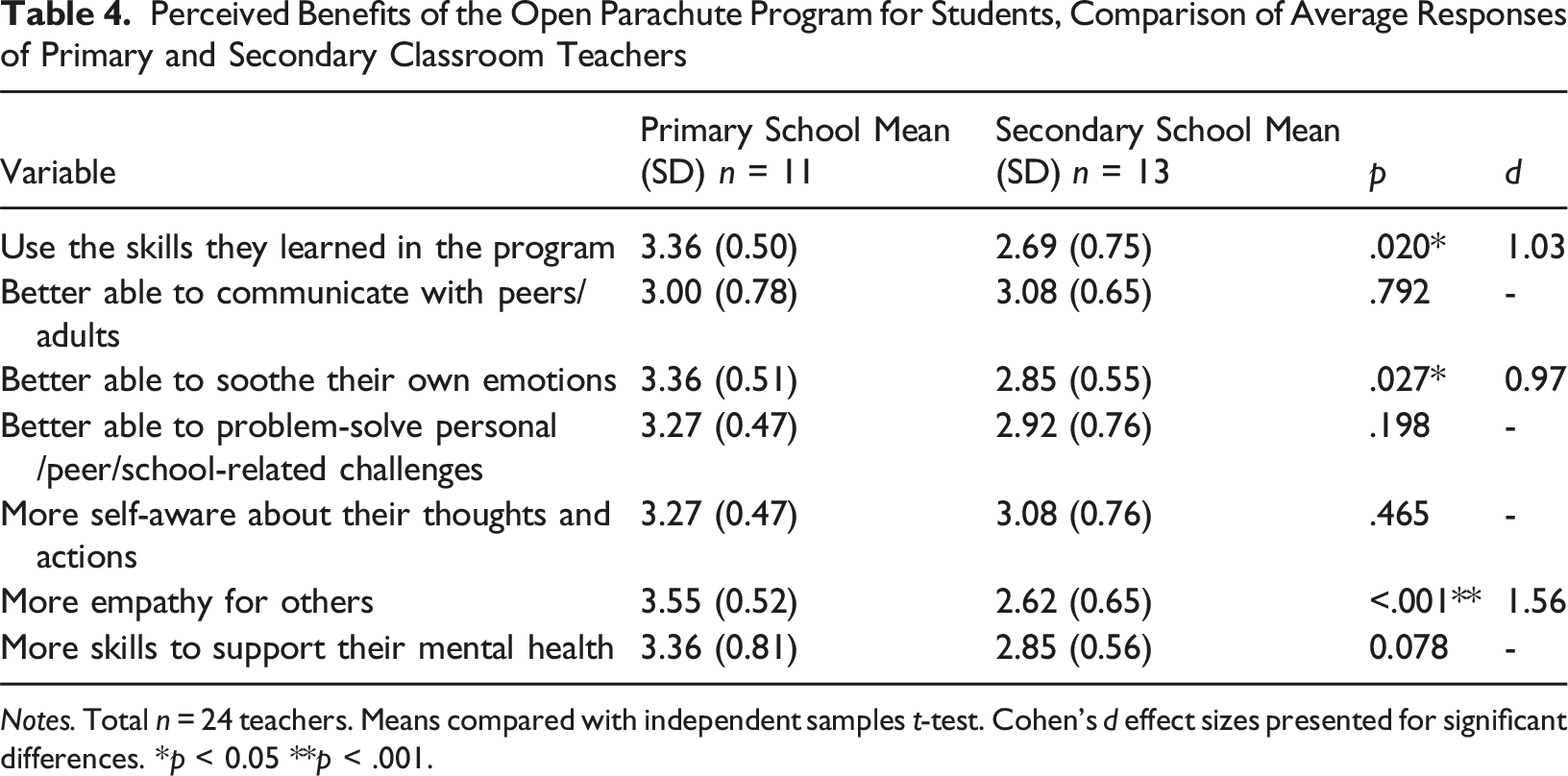
Notes. Total n = 24 teachers. Means compared with independent samples t-test. Cohen’s d effect sizes presented for significant differences. *p < 0.05 **p < .001.
Feasibility and Program Fidelity for Open Parachute
The amount of time teachers spent preparing for lessons varied, with 8 teachers reporting that they spent more than 30 minutes prepping for each lesson, whereas 6 spent 5 to 10 minutes, and the remainder of teachers fell somewhere within this range. Overall, most teachers (13) felt very well prepared to run the Open Parachute program, whereas 9 felt somewhat prepared, and 2 did not feel well prepared. There was no significant relationship between time spent preparing and feeling prepared to run the Open Parachute program. When asked how closely the Open Parachute lessons were followed, 18 of the teachers indicated ‘a lot’ or ‘quite a lot’, and 6 said ‘somewhat’. No teachers endorsed ‘not at all’. Overall, 18 teachers delivered the full program (approximately 30 classes), and 6 teachers omitted at least one lesson. Based on an open-ended response asking which units were missed, teachers either omitted lessons due to time constraints, or they chose to omit units with more difficult topics (e.g. grief and trauma).
Acceptability of Open Parachute
Most teachers, 13, reported that running the Open Parachute program helped them ‘quite a lot’ or ‘a lot’ in their role as a teacher, with 9 reporting ‘somewhat’ and 2 reporting ‘a little’ or ‘not at all’. Most school leaders (7) reported that running the Open Parachute program helped their team in their roles as teachers ‘quite a lot’ or ‘a lot’, with 4 reporting ‘somewhat’ and 2 reporting ‘a little’.
Teachers’ and School Leaders’ Perceptions of the Open Parachute Program Experience and Implementation
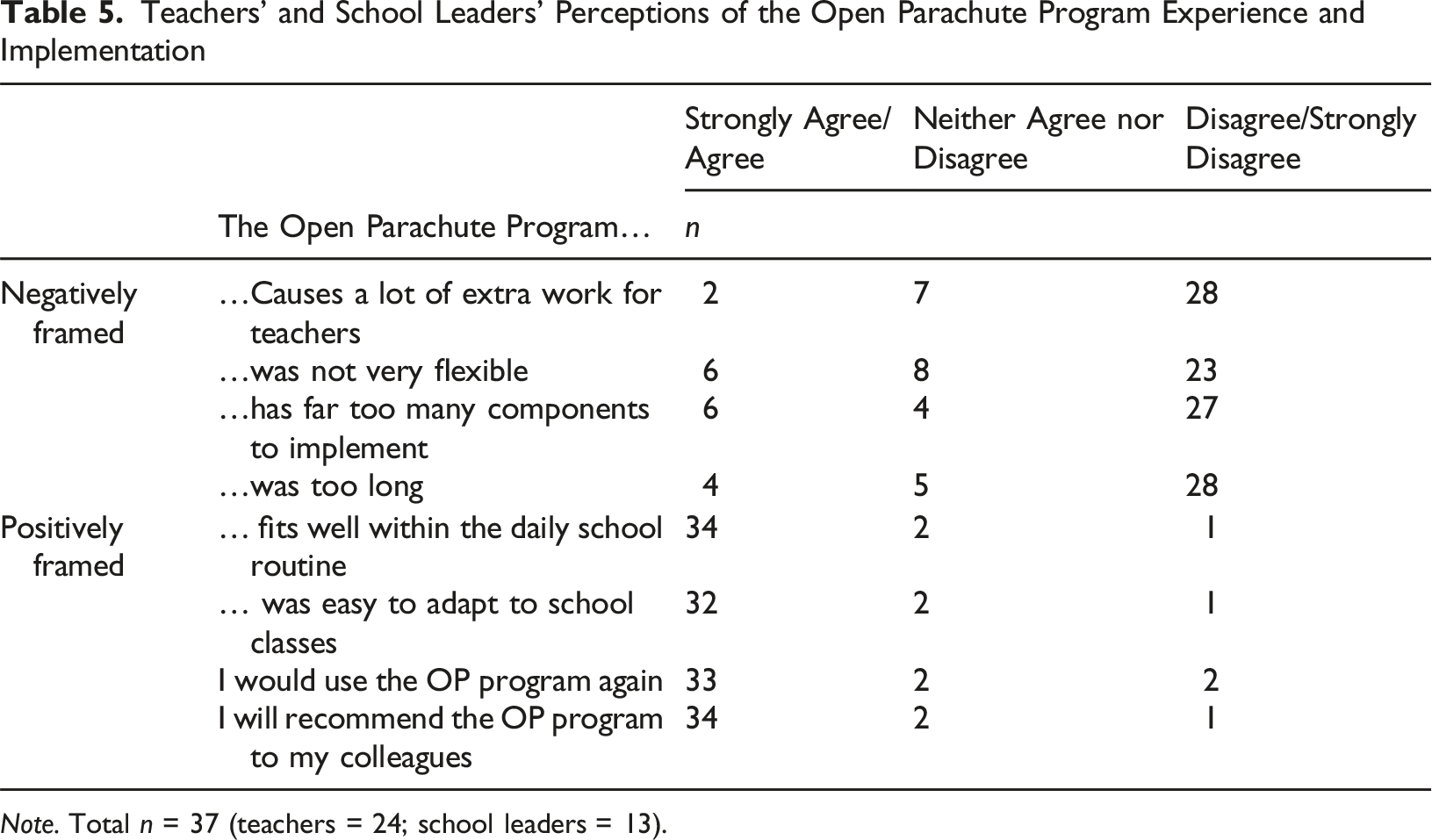
Note. Total n = 37 (teachers = 24; school leaders = 13).
Importantly, the majority of teachers and school leaders (32) ‘agreed’ or ‘strongly agreed’ that the Open Parachute program ‘was easy to adapt to school/my class’. This suggests that many teachers and school leaders were able to tailor the program to meet their class and school demands. A small portion of teachers and school leaders (6) ‘agreed’ or ‘strongly agreed’ that the program ‘was not very flexible’, suggesting that improvements can be made to the Open Parachute program to increase flexibility in the delivery of the program to meet teacher and school leader demands (Table 5).
When asked if they would use Open Parachute again, 33 teachers and school leaders ‘agreed’ or ‘strongly agreed’, suggesting strong uptake of the program. Most teachers and school leaders (27) felt the Open Parachute program would have a greater impact if students could complete it again next year by indicating ‘quite a bit’ or ‘a lot’. Similarly, 34 teachers and school leaders ‘agreed’ or ‘strongly agreed’ that they would recommend the Open Parachute program to colleagues (Table 5). When asked to rate on a scale from 0, ‘I would not recommend’ to 10, ‘I would definitely recommend’, teachers and school leaders reported on average a mean score of 8.19 (SD = 1.41), suggesting strong endorsement of the program.
Discussion
This study evaluated the feasibility, acceptability, and perceived benefits of the Open Parachute program, designed to bolster mental health literacy among school-age children through classroom instruction. The program featured a curriculum requiring minimal preparation and training for school educators, employing evidence-based educational strategies to address growing concerns about mental health. Findings from this study revealed initial success based on teacher-reported perceived benefits observed for both teacher and student outcomes. While the program’s implementation was found feasible and acceptable, according to the respondents, suggestions for enhancing flexibility were also noted. Overall, this study provides encouraging evidence endorsing initial use of the Open Parachute program in both primary and secondary school educational settings within Australia.
Perceived Benefits of the Open Parachute Program
In terms of perceived benefits, this group of educators reported a range of positive outcomes associated with the program. Many felt that the Open Parachute program improved their understanding of youth mental health challenges, enhanced their connection with students, and increased their confidence in supporting student wellbeing. These findings are consistent with prior research indicating that school-based mental health programs can enhance teacher competence and comfort in addressing mental health issues alongside educating students (Emonson et al., 2022). Additionally, many educators reported enhancement of their own mental health literacy and increased self-awareness about their own thoughts and actions, likely contributing to a more supportive and nurturing classroom atmosphere. These outcomes provide early evidence supporting the Open Parachute program as a possible mechanism to enhance instructional efficacy and encourage a more holistic method to supporting students in managing their mental health within a classroom setting.
In parallel, educators also reported benefits for students participating in the Open Parachute program. Just over a quarter of the educators reported that students demonstrated improved skills in communication, emotion regulation, problem-solving, and empathy. These outcomes highlight the program’s potential to foster mental health literacy among students, equipping them with essential skills to navigate social and emotional challenges effectively. Notably, there were differences in perceived program impact between primary and secondary school levels. Primary school teachers reported greater improvements in students’ ability to soothe their own emotions and show empathy compared to their secondary school counterparts. This distinction underscores the developmental nuances that must be considered when implementing mental health interventions across different age groups.
Feasibility and Fidelity when Implementing Open Parachute
The feasibility and fidelity assessment of the Open Parachute program from the perspective of teachers highlighted several important considerations. The majority of teachers reported a high level of adherence to the program’s structured lessons, with 75% indicating they followed the exercises closely. This suggests that the program content was generally delivered as intended.
Although the preparation time varied among teachers, with 35% spending over 30 minutes per lesson and others less, the overall preparedness to deliver the program was notably high. This readiness is crucial for ensuring that teachers feel equipped to engage effectively with the curriculum content. Furthermore, while some units were occasionally omitted due to time constraints or the sensitivity of the topics (e.g. grief and trauma), the overall structure of the program was perceived as manageable and well-suited to the classroom environment.
Overall, these findings suggest that the implementation of the Open Parachute program was manageable for teachers. This underscores the program’s user-friendliness and provides initial support for its feasibility for facilitation. Furthermore, the high level of reported fidelity suggests a heightened likelihood that students from the classes involved in this study received similar instruction in mental health literacy skills through the Open Parachute program.
Acceptability of Open Parachute
The acceptability of the Open Parachute program was another critical aspect assessed in this study with 92% of educators indicating they would recommend the program to colleagues. Additionally, 89% of educators expressed a willingness to use the program again. This high level of endorsement underscores the perceived value and utility of the program in offering mental health literacy programming to students.
Moreover, the program’s adaptability emerged as a significant factor contributing to its acceptability. The majority of educators agreed that the program integrated smoothly into daily routines and did not impose excessive workload burdens. This aligns with previous research emphasising the importance of program fit within existing school operations to optimise implementation success (Androutsos et al., 2014; Manios et al., 2014). Further, a vast majority of teachers and school leaders agreed that the program was easy to adapt to their specific classroom and school contexts and could be seamlessly integrated into the school curriculum. This adaptability is crucial to ensure that interventions resonate with diverse educational settings and can be tailored to meet the unique needs of students and teachers alike. While most teachers and school leaders found the program flexible and easy to adapt, a small minority noted concerns regarding the program’s inflexibility, suggesting opportunities for enhancing adaptability to better meet the diverse demands of teachers and classrooms. Nevertheless, this study demonstrated that many teachers and school leaders successfully implemented the Open Parachute program to address their classroom and school needs.
Limitations and Future Directions
While this study found promising results supporting the Open Parachute program, several limitations should be acknowledged. First, the data collected relied on a single informant and was self-reported – that is, teachers and school leaders reported on program benefit for their students. As participants may provide socially desirable responses or misreport their behaviours and experiences, future considerations could include multi-informant methods and objective measures to fully capture student and teacher experiences and outcomes. Further research could explore longitudinal impacts of the Open Parachute program on both teachers and students, examining sustained benefits and potential areas for program refinement.
Second, there was an absence of pre-program measurements, which presents a challenge in fully determining the program’s impact. For a more comprehensive evaluation, future implementations can incorporate both pre- and post-assessments. Additionally, the study did not include a control comparison group. Future program implementations could consider using a randomised controlled trial or a quasi-experimental design to better understand the effects of the Open Parachute program and enable comparisons between program users and non-program users.
Third, all participating schools were South Australian government primary and secondary schools. Of the 30 schools initially approached, only 13 responded, which may indicate issues related to non-response, as well as the potential limitations of a small sample size. As such, the findings of this study may primarily be applicable to government schools in South Australia, rather than generalisable to Australian schools more broadly. Further research is needed to explore the effectiveness of the program in other school sectors, such as Catholic and independent schools, as well as in other jurisdictions, and with larger sample sizes.
Fourth, while we measured adherence to the program, future research should focus on better understanding program fidelity. In addition, it would be beneficial to gather qualitative data on any adaptations or amendments teachers may make to tailor the program to their specific classroom needs. This could provide valuable insight into how the program is implemented in practice and the potential impact of such modifications.
Lastly, investigating the cost-effectiveness of scaling the Open Parachute program across diverse school settings would provide valuable insights for policymakers and educators seeking to prioritise mental health literacy within educational curricula.
Conclusion
This study demonstrated that the Open Parachute program, a curriculum-based program designed to encourage mental health literacy education, was both feasible and acceptable in a South Australian school setting. The findings highlight its seamless integration into existing curricula, ease of use, and high fidelity through consistent adherence to the intended delivery of the program. The program facilitated interest and discussion in mental health literacy among teachers, school leaders, and students, receiving strong endorsement. Overall, the findings underscore the Open Parachute program’s potential to support teachers in fostering mental health literacy while navigating the complexities of educational settings. By addressing the critical need for effective mental health education in schools, initiatives like the Open Parachute program have the capacity to promote long-term positive outcomes for both students and educators, thereby contributing to healthier and more supportive school environments.
Footnotes
Acknowledgements
We acknowledge and thank the teacher and school administrative staff participants who took part in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
Brae Anne McArthur reports a relationship with Open Parachute that includes research consulting and advising. All other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.