
Abstract
Growing with Gratitude (GWG) is a universal prevention program based on positive psychology that aims to prevent anxiety and depression in primary-school-aged children. The mental health of children is a key concern for schools as it has an extensive impact in all areas of life. A cluster randomised controlled trial was implemented in nine primary schools (including 27 classes, n = 537 students) in South Australia to evaluate the program. Classrooms were randomly allocated to either a waitlist control or to the GWG program. Students’ anxiety and depression and wellbeing were measured as outcomes at five time points (baseline, mid-program, post-intervention, and 6-month and 12-month follow-up). There were no significant differences for primary or secondary outcomes between the conditions at any time point. Implementation fidelity was poor across the trial. The GWG program did appear to have some impact on children with clinically significant levels of anxiety and depression at baseline. These findings highlight challenges with implementing prevention programs in primary schools and provide suggestions for future research.
Keywords
The mental health and wellbeing of children is critical as it impacts all aspects of life and can have lasting impacts into adulthood. Primary and secondary schools have been identified as potential locations for children to access programs that address mental health (Humphrey, 2023). The need for intervention in this critical period has already been recognised, due to the rates of mental disorders that are observed in childhood and adolescence. It is estimated that 10% of children worldwide, and approximately 14% of children in Australia experience a mental disorder (World Health Organisation [WHO], 2022; Lawrence et al., 2015). During the COVID-19 pandemic, these rates were estimated to be more than 30% of young people (children, adolescents and college students) who experienced anxiety and depression (Bower et al., 2023). Targeted interventions for primary and secondary school students who are at-risk have been developed (e.g. Barrett et al., 2006; Rapee et al., 2006), but such interventions need accredited facilitators and therefore require resources that many schools struggle to access. Furthermore, targeted interventions can add to stigma experienced when children are removed from class to participate (Hayes et al., 2023). In contrast, universal prevention programs include the whole class or school. Although effect sizes are typically smaller compared with targeted interventions (Hayes et al., 2023), universal preventions are less resource-intensive and can be delivered to children who currently demonstrate symptoms, as well as children without symptoms but who may be at risk of developing mental health issues. By intervening early, future onset may be prevented (Hayes et al., 2023). Teachers are well-placed to deliver universal prevention programs directly to all children in the classroom, and engagement from teachers has been found to be helpful in more seamless integration of programs (e.g. teachers can refer to the program throughout the school day) (Fenwick-Smith et al., 2018).
Positive psychology as a discipline aims to ‘…change the focus of psychology from preoccupation only with repairing the worst things in life to also building positive qualities’ (Seligman & Csikszentmihalyi, 2000, p. 5). There have been criticisms of positive psychology as a discipline (see van Zyl et al., 2024); however, there is a large amount of research in support of the field. For instance, there is evidence to suggest that interventions that utilise positive psychology principles are effective in lowering levels of anxiety and depression in adolescents (Bolier et al., 2013; Carr et al., 2021). The PERMA wellbeing framework includes Positive Emotion, Engagement, Relationships, Meaning and Achievement (Seligman, 2011) and has been found to relate to improved resilience and mental health, as well as to reduced symptoms of mental disorder in primary-school-aged children (Turner et al., 2023). There have been attempts at positive psychology interventions using the PERMA framework in schools (e.g. Fox Eades & Gray, 2017; Francis et al., 2021), a key example is the Penn Resiliency Program (for 9- to 14-year-olds). Research has shown that this program reduced anxiety, depression, and hopelessness (Seligman et al., 2009). However, this program was not specifically designed for primary-school-aged children. The lack of evidence-based preventative programs for primary-school-aged children should be addressed. Children in primary school are at different developmental stages compared to high school and there is a high onset of mental disorders observed across childhood, suggesting the need for specialised programs. Further criticisms of the evidence for positive psychology interventions have included the lack of long-term follow-up and the inappropriate use of control groups. Examples of inappropriate controls include using a ‘negative’ condition, such as listing three grievances in the control compared to three positive experiences as an intervention, which may exaggerate the impact of the positive condition (Dickens, 2017; Wood et al., 2010). The current study aimed to address these criticisms by including longer term follow-ups (6-month and 12-month post-intervention) and including a waitlist control condition.
Growing with Gratitude (GWG; Growing with Gratitude, 2022) is a preventative program for primary school students. It is based on PERMA and positive psychology principles and focuses on five Habits of Happiness: An Attitude of Gratitude, Random Acts of Kindness, Positive Reflection, Well-being Warriors (mindfulness and physical activity) and Operation Home Service (serving and helping others). The program has been running in Australian schools for seven years but has yet to be formally evaluated. Although acceptability and feasibility have not been formally evaluated, informal feedback from the South Australian schools who have been delivering the program for several years suggests that the program is easy to implement and well accepted by staff and students. Each of the concepts addressed by the five Habits of Happiness is supported by research evidence. Gratitude interventions have been found to improve wellbeing and mental health (Brausen, 2017; Emmons et al., 2003; Khanna et al., 2022; Seligman et al., 2005) and acts of kindness are related to life satisfaction (Buchanan & Bardi, 2010), both of which align with the Positive Emotions and Relationships aspects of PERMA. Positive reflection, which involves thinking about good things that have happened, is less represented in the literature; however, it fits into the Positive Emotion aspect of PERMA and is theoretically supported by the broaden and build theory, where continued retrieval of positive resources increases the automatic use of these resources (Fredrickson, 2001). Physical activity and mindfulness have been found to improve mental health and wellbeing (Amundsen et al., 2020; Burton et al., 2009; Kallapiran et al., 2015) and are reflected in the Achievement and Engagement elements of PERMA. Preliminary findings also suggest that service to others (Operation Home Service) increases life satisfaction and wellbeing, for example, among people who volunteer (Meier & Stutzer, 2008), and this Habit is indicative of the Meaning and Achievement aspects of PERMA.
If the program is effective, there is a need to understand why PERMA impacts mental health and disorders. Two potential factors which may have a role to play in this relationship are resilience and emotion regulation (Djambazova-Popordanoska, 2016; Goldstein & Brooks, 2012; Gülay Ogelman & Önder, 2021; Turner et al., 2023). Resilience, or an ability to bounce back in the face of adversity, is considered a protective barrier against mental disorder (Davydov et al., 2010). Emotion regulation is the moderation of emotions in response to the individual’s environment, whether consciously or unconsciously (Bargh & Williams, 2007; Rottenberg & Gross, 2003). Adaptive emotion regulation strategies have been associated with improved wellbeing, whereas maladaptive strategies can have a negative impact on mental health (Bradley, 2003; Djambazova-Popordanoska, 2016; Kring & Werner, 2004; Ranney et al., 2017). For this reason, resilience and emotion regulation will be measured in the current study and analysed as potential mediators, if the program is effective. Furthermore, gratitude will also be examined to determine what role it might play in impacting mental health and wellbeing.
In GWG, there are nine content lessons ranging from 30–45 minutes and all materials are sourced via an online portal (see Appendix A for an overview). Lessons are delivered by classroom teachers after participating in training on how to use the online portal. The lessons are designed to be engaging for students, typically including a video, discussion about the primary idea, and an activity or game to practise the concept. The lessons vary depending on year level, with different foci for different age groups, so that a student could repeat the program. The program is for Foundation (Australian first year of primary school) to Year 6 (seventh year of primary school); however, this study focused on Years 3–5 as the literature suggests that gratitude is not generally linked to happiness until around 7 years of age, unless it is domain specific (e.g. activities, nature, and material objects) (Nguyen & Gordon, 2020). In addition to the nine lessons, there is a large pool of short activities and games available to facilitators to reinforce the concepts.
It is critical that there is an evidence base for programs that are delivered in schools. The GWG program shows promise, as it is specifically designed for primary school students and is based on well-supported positive psychology principles, as described above. The program is accessible to schools due to the online nature and as it can be facilitated by classroom teachers. Currently, however, there is no empirical evidence on the effectiveness of the program.
The aim of this study was to evaluate the effectiveness of GWG, by assessing whether after completing the program children had increased levels of wellbeing, and reduced levels of anxiety and depression compared with a control condition. The study also aimed to examine resilience, gratitude and emotion regulation as potential mediators of change if the program is effective. We aimed to assess whether any effects of participating in the program would be present immediately post-intervention and whether preventative effects would remain evident 12-month post-intervention.
Methods
Research design and procedure
Ethics approval was granted by the Flinders University Human Research Ethics Committee (SBREC 8386) and the Department for Education South Australia (2019–0022). The trial was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12622000700730). This study was a cluster randomised controlled trial, with random allocation to GWG or control group at the class level (see Figure 1). Participant flow chart.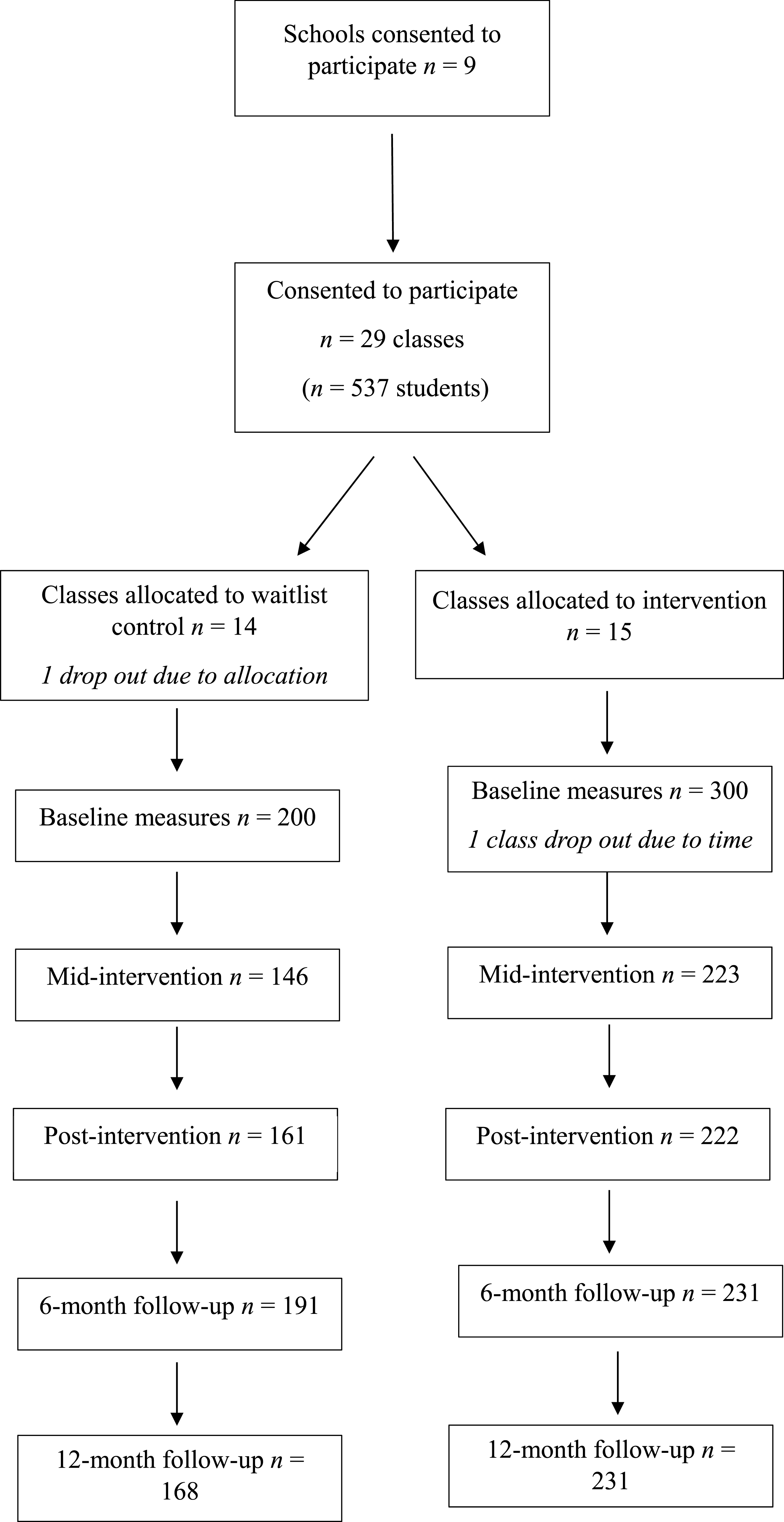
Schools were recruited via email using a letter and video about the project. A convenience sampling method was used. Schools who consented to participate were asked to nominate Year 3, 4 and 5 classes who would be willing to be involved. It was up to school leadership to decide whether to consult teachers in this process (e.g. give them the option to be involved). Active consent was sought from parents/caregivers for children to participate in the data collection. Classes were randomly allocated to GWG or a waitlist control condition; teachers in the GWG condition received training. Classes allocated to the waitlist control were provided with the program after the 12-month follow-up. Schools were recruited across 2021–2022, with program delivery, baseline and mid-intervention surveys across Term 2 or 3 of 2022. Recruitment was stopped due to the lack of available resources (e.g. time and eligible schools to approach) in Term 2, 2022.
Students completed a baseline survey, mid-program and post-program survey. Students completed follow-up surveys at 6-month and 12-month post-program. Most data were collected via an online survey (Qualtrics) facilitated by the classroom teacher, except for the 6-month and 12-month follow-ups which were facilitated by the first author on paper (as students had changed classes and teachers).
Participants and sample size
Participants were students in Year 3, 4 or 5, and their teachers. No other inclusion or exclusion criteria were applied. Per condition, 18 classes (360 students) were needed to detect an effect (Standardised Mean Difference) of 0.3 with 80% power at the 5% significance level for an ICC of 0.05 and for a correlation of 0.3 between the primary outcome (anxiety and depression scores) post-intervention and baseline value of outcome. The average cluster size is 20 and is assumed to be equal for all clusters.
There were 537 students included in the study. Participants were from nine schools, with 15 classes allocated to the intervention and 14 to the control condition.
Sample characteristics
Nine schools from both regional and metropolitan South Australia were included in the study. This included seven government and two non-government (self-funded/private) schools. The MySchool website reports data about all Australian schools, including a rating of socioeconomic status (SES) called the Index of Community Socio-Educational Advantage (ICSEA). ICSEA has an average score of 1000 with a standard deviation of 100. Two schools had lower than average SES and the remaining schools had an ICSEA rating of 1000 or higher, ranging from 1015 to 1132 (Australian Curriculum, Assessment and Reporting Authority [ACARA], 2023). Two of the schools were classified as outer regional, and all others were metropolitan.
Random assignment method
Classes were assigned to either the prevention or control condition by random assignment. Block randomisation was used, with block sizes of 4, 6 and 8. An online tool was used to produce the sequence (Sealed Envelope Ltd, 2022). The randomisation was completed by a researcher separate to the study.
Masking
Teachers were aware of the random allocation as those allocated to the GWG condition needed to complete training and prepare. Teachers were instructed not to let students or parents know which condition they had been allocated to prior to giving consent so that the decision of whether to be involved was not biased.
Measures
The student survey included the following five scales at all data collection time points.
Stirling Well-being Scale (Liddle & Carter, 2015): This scale measures positive aspects of wellbeing. The measure includes 15 statements scored on a 5-point Likert scale, where 1 = Never and 5 = All of the time. Scores range from 12–60. Example statements include: ‘I think good things will happen in my life’ and ‘I’ve been in a good mood’. It was specifically chosen due to the low burden on time and the use of positive wording, as opposed to a focus on mental health deficits (measured below). The scale has been reported to have good internal, construct and external reliability for 8- to 15-year-olds, and not to be impacted by ceiling effects (Liddle & Carter, 2015). In this study at baseline, internal consistency for this scale was good with a Cronbach’s alpha of .88.
Revised Child Anxiety and Depression Scale – Short Version (RCADS-25; Ebesutani et al., 2012): The scale includes 25 statements scored on a 4-point Likert scale, where 0 = Never and 3 = Always. A higher score indicates higher levels of anxiety and depression, and this scale was selected to ensure a strong measure of anxiety and depression was included. Example statements include: ‘I feel sad or empty’, ‘I have no energy for things’ and ‘I worry that something bad will happen to me’. The scale includes subscales for separation anxiety disorder, social phobia, obsessive-compulsive disorder, panic disorder, generalised anxiety disorder and major depressive disorder. The RCADS-25 has strong structural, convergent and discriminant validity, as well as reliability (Ebesutani et al., 2012). RCADS produces a raw total score (sum of all items) which was used for analysis. It also produces a T-score which demonstrates clinical cut off points, a T-Score >65 is considered borderline and >70 represents the clinical range for symptoms of anxiety and depression (Chorpita et al., 2000). Cronbach’s alpha for this measure was .85 at baseline.
Child and Youth Resilience Measure Revised (CYRM-R; Jefferies et al., 2019): The CYRM-R is a measure of resilience that includes 17 statements, scored on a 5-point Likert scale, where 1 = not at all and 5 = a lot. There are separate versions for 5–9-year-old and 10–23-year-old respondents. An example statement for the 5–9-year-old version is: ‘Do you share with people around you?’ The analogous statement in the 10–23-year-old version is: ‘I cooperate with people around me’. Scores range from 17–85, with a higher score indicating higher levels of resilience. The CYRM-R has been found to have good reliability and validity for children and adolescents (Jefferies et al., 2019). At baseline, Cronbach’s alpha for this measure was .82.
The Gratitude Questionnaire-Six Item Form (GQ-6; Froh et al., 2011): The GQ-6 includes six statements scored on a 7-point Likert scale, where 1 = strongly disagree, 4 = neutral and 7 = strongly agree. Example statements include: ‘I have so much in life to be thankful for’. Items three and six are reverse scored. A higher score indicates higher levels of gratitude. The GQ-6 has been found to demonstrate good validity and reliability in adolescent settings (Froh et al., 2011). Cronbach’s alpha for this measure was poor at baseline (.57); however, McDonald’s omega (McDonald, 1999) was acceptable at .74.
Emotion Regulation Questionnaire for Children and Adolescents (ERQ-CA; Gullone & Taffe, 2012): The ERQ-CA includes 10 statements, scored on a 5-point Likert scale, where 1 = strongly disagree, 3 = half and half and 5 = strongly agree. Example statements include: ‘When I want to feel happier, I think about something different’ and ‘I control my feelings by not showing them’. The scale includes two subscales; six items for cognitive reappraisal (CR) and four items for emotion suppression (ES). Scores range from 6–30 for the CR scale and 4–20 for the ES scale, with higher scores indicating greater use of the strategy. The scale has demonstrated good reliability and validity in child and adolescent samples (Gullone & Taffe, 2012). Cronbach’s alpha was acceptable for the cognitive reappraisal (CR) subscale, and was .84 at baseline; however, the Cronbach’s alpha for the emotion suppression (ES) scale was lower at .67 (omega of .68) and for this reason was not included in the model.
Intervention
Classes allocated to the GWG condition received the Growing with Gratitude program, delivered by their classroom teacher in either Term 2 or 3 of 2022. Classes in the control condition received the standard Australian curriculum, which includes some personal health topics but no specific wellbeing program or curriculum. GWG includes nine (30–45 minute) lessons (see Appendix A) and, in this study, teachers were asked to deliver one lesson per week. There are also short (5–10 minute) activities to reinforce the Habits, which students complete three times a week. Teachers facilitating the program received 30-minutes of online training from the program director, a manual describing research requirements and timelines (including when each lesson should be delivered in the term), as well as access to the first author and program director via email for any questions or support. Only limited training was provided as the lessons are written in an easy-to-follow lesson plan format, with which teachers are familiar.
Implementation fidelity
Teachers of classes allocated to the GWG condition completed a weekly implementation fidelity survey for the 9 weeks that they administered the program. The survey asked teachers to report on: whether they had completed the weekly lesson; which, if any, aspects of the lesson were not completed; how many short activities were completed (these were not reported due to overall low levels of use); and for any relevant comments about implementing the program.
Attrition
One class withdrew from the study prior to the baseline measures being collected due to being allocated to the control condition. One class in the GWG condition withdrew due to time constraints after completing the baseline measures and the first two lessons. There were also large fluctuations in survey response rates due to student absences. Students who were absent on the day that surveys were completed were not able to be followed up due to logistical issues. Absences were generally high over the time the surveys were completed, due to students contracting COVID-19. Completion rates for the surveys were 74% for the mid-intervention survey, 77% for post-intervention, 84% for the 6-month follow-up and 80% for the 12-month follow-up. See Figure 1 for the number of participants who completed each survey.
Statistical methods
A constrained Longitudinal Data Analysis (cLDA) model was applied to each outcome. In the cLDA model, the baseline value is included together with the post-baseline values and a constraint of a common baseline mean outcome score across treatment groups was applied to the model. The benefit of the cLDA model is that we included students that had either a baseline measurement or follow-up measurement. This means all the information collected was used in the analysis and did not require a complete case analysis. The model was applied to the outcome scores by treatment (GWG, Control) and included a random effect of class, which accounted for clustering at the class level in the model. The follow-up age was used where the baseline age was missing (n = 64). School and class effects were confounded for schools where only one class participated, this led to convergence problems when school was taken into account in the analysis; therefore, clustering only at the class level in the model was accounted for in the model. Effect sizes for the mean difference were approximated by dividing the marginal mean differences between groups by the pooled standard deviation at baseline.
Results
Baseline characteristics
Baseline age of participants ranged from 8 to 10 years (M = 8.84, SD = .05) in the GWG condition, and 7–10 years in the control condition (M = 9.27, SD = .06). The GWG condition included 161 girls (50%), 144 boys (45%) and 14 (4%) preferred not to say. The control condition had 98 girls (49%), 93 boys (46%) and 10 (5%) preferred not to say. Using the RCADS T-score, 18 participants (5%) were in the borderline range and 17 (5%) in the clinical range in the GWG condition at baseline. Among the control condition, five (2%) were considered borderline and eight (4%) were above clinical cut offs.
Outcomes
Mean Outcomes at Each Timepoint for GWG and Control Conditions.
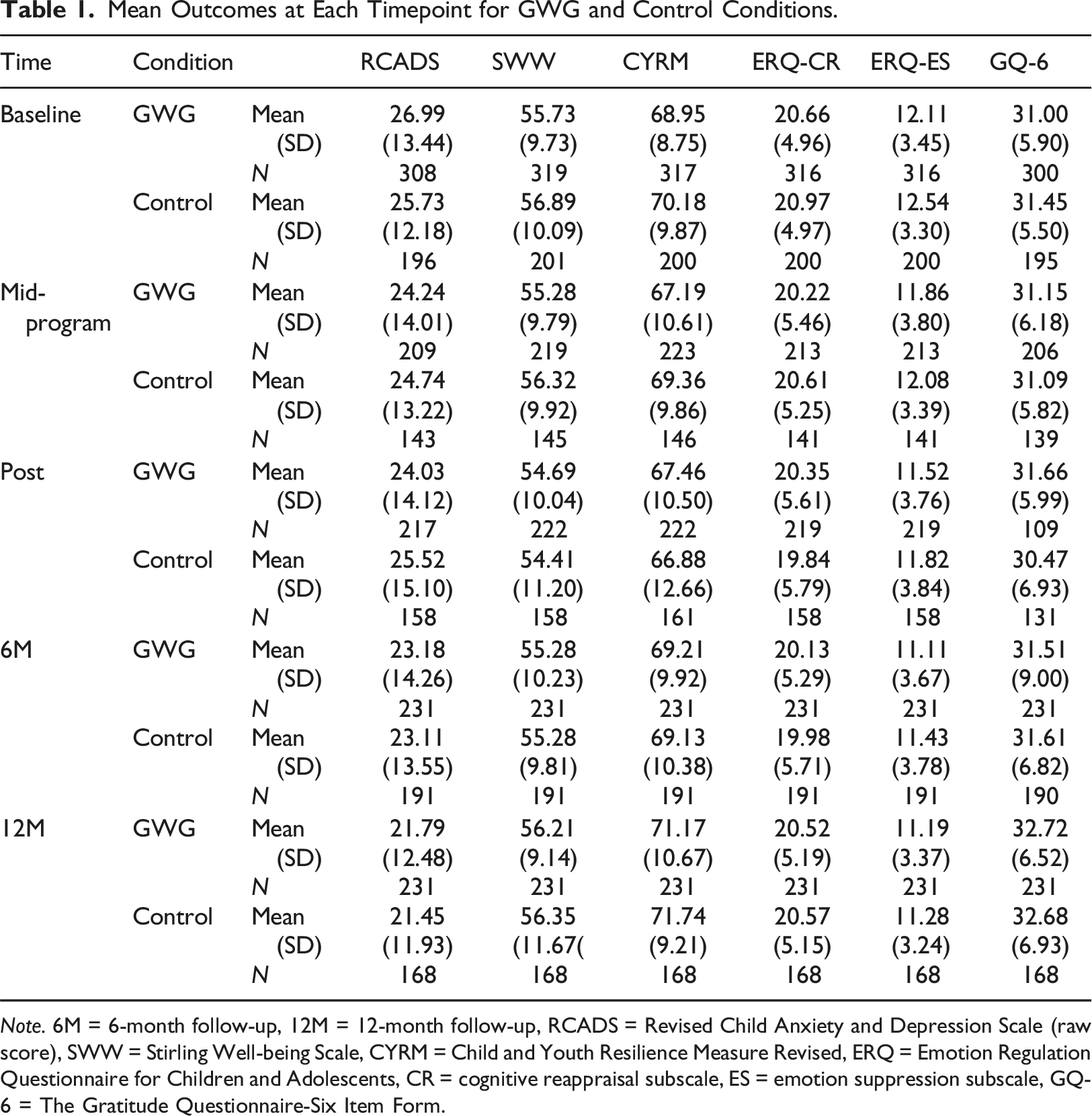
Note. 6M = 6-month follow-up, 12M = 12-month follow-up, RCADS = Revised Child Anxiety and Depression Scale (raw score), SWW = Stirling Well-being Scale, CYRM = Child and Youth Resilience Measure Revised, ERQ = Emotion Regulation Questionnaire for Children and Adolescents, CR = cognitive reappraisal subscale, ES = emotion suppression subscale, GQ-6 = The Gratitude Questionnaire-Six Item Form.
Constrained Longitudinal Data Analysis (Baseline to Post-intervention).
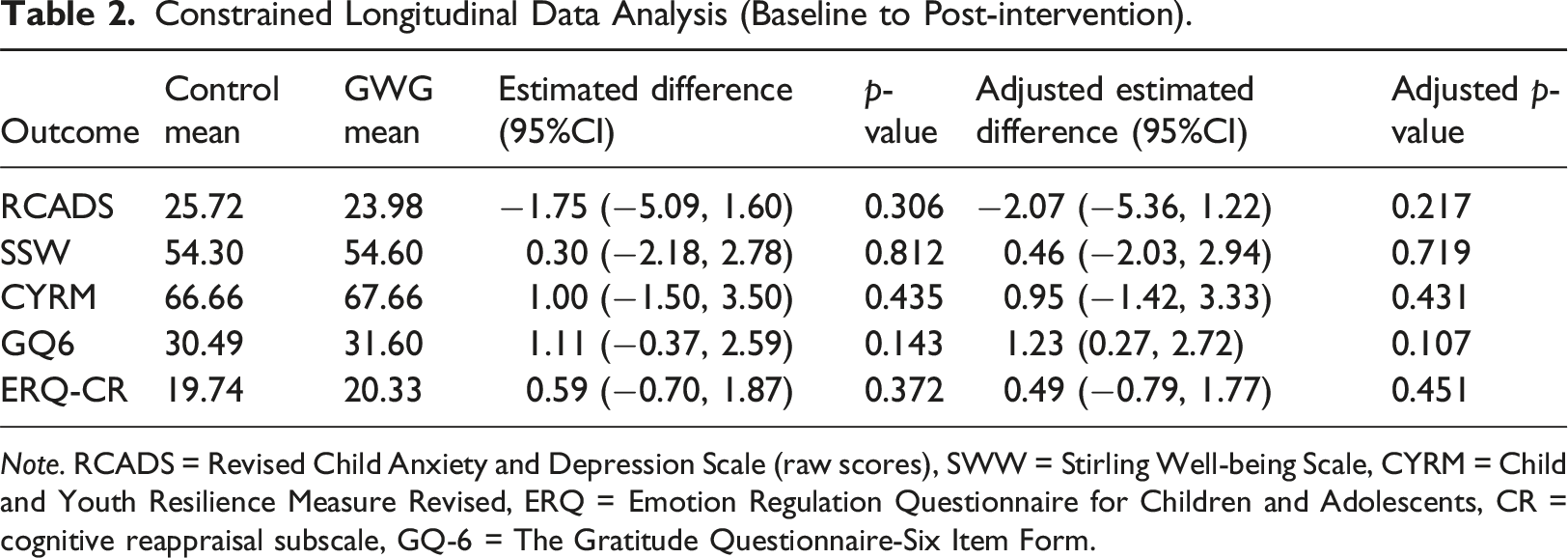
Note. RCADS = Revised Child Anxiety and Depression Scale (raw scores), SWW = Stirling Well-being Scale, CYRM = Child and Youth Resilience Measure Revised, ERQ = Emotion Regulation Questionnaire for Children and Adolescents, CR = cognitive reappraisal subscale, GQ-6 = The Gratitude Questionnaire-Six Item Form.
Implementation fidelity
Lessons Reported Complete by Teachers.
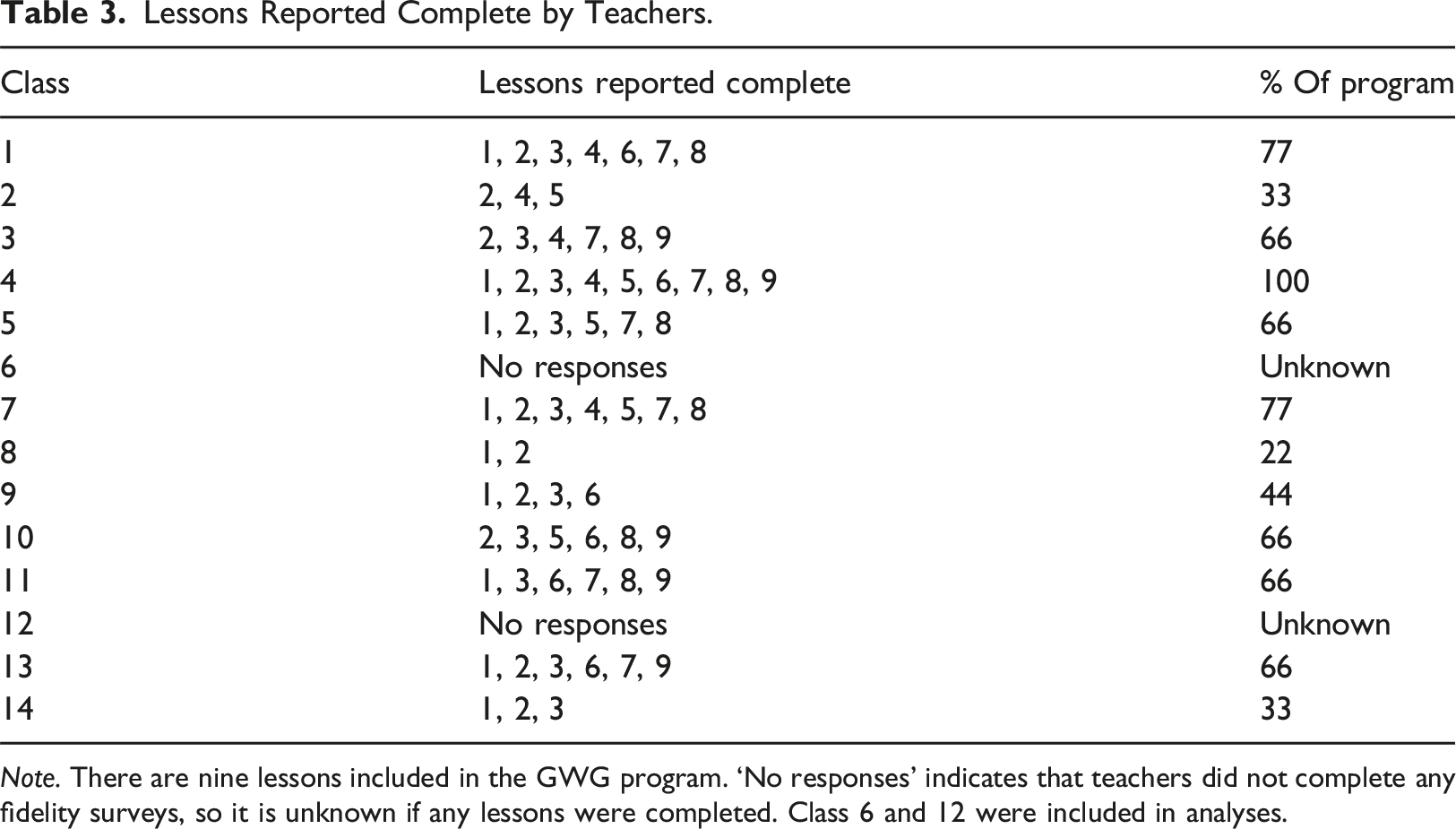
Note. There are nine lessons included in the GWG program. ‘No responses’ indicates that teachers did not complete any fidelity surveys, so it is unknown if any lessons were completed. Class 6 and 12 were included in analyses.
Clinical significance
RCADS provides a cut-off point, using participant age and gender, which informs whether their score is indicative of clinical anxiety or depression (a T-score >65 is borderline and a T-score >70 is above the clinical threshold; Chorpita et al., 2000). The program did appear to benefit participants who were above clinical cut offs on the RCADS at baseline. In the GWG condition participants who were borderline or above the RCADS cut-off score had a mean RCADS T-score of M = 71.42 (SD = 5.46) at baseline and M = 60.13 (SD = 12.08) post-intervention. The clinical subgroup in the control condition had a mean RCADS T-score of M = 73.86 (SD = 6.08) at baseline and M = 66.25 (SD = 8.39) post-intervention. Among participants in the GWG condition, 11.67% were above the borderline threshold at baseline and 7.79% at 12-month follow-up (a 3.88% change). In the control condition, 6.5% were above the borderline threshold at baseline and at 12-month follow-up (no change). This only includes participants for whom we had a baseline score (for both conditions).
From baseline to 12-month follow-up, 17 participants moved to below a clinically significant score (from >65 to below) in the GWG condition compared with only five in the control condition. Of the group who were initially above borderline or clinical threshold, 48.5% recovered in the GWG condition, compared with 38% of the control condition.
Discussion
This study was a cluster randomised controlled trial, evaluating the effectiveness of the program Growing with Gratitude in nine South Australian primary schools. In this study, the program was not effective in decreasing anxiety and depression or improving wellbeing. It is worth noting, however, that implementation fidelity was poor, meaning it is difficult to make definitive statements about effectiveness. Considering this, the program was also not effective as a prevention as there were no significant differences between the conditions at 6- or 12-month follow-ups and effect sizes were negligible at these time points. The program had no impact on secondary outcomes (resilience, gratitude, and emotion regulation). We did not explore gratitude, resilience and emotion regulation as potential mediating variables due to the lack of evidence of effect of the program for the main outcomes of anxiety and depression and wellbeing. Overall, the findings from our study are contradictory to the findings that positive psychology interventions have an impact on children’s anxiety, depression and wellbeing outcomes. There were several findings from this study that are worth discussing and that have implications for future school research.
Adherence to the program was a major issue in this study, with only three of the fourteen classes completing more than 70% of the program. This is a possible explanation for the lack of effectiveness of the program. The low rate of implementation fidelity could reflect the current school climate and wider issues facing teachers. It is well established that there is a plethora of competing demands on teachers, causing it to be a burdened profession (e.g. Crump, 2005; Heffernan et al., 2022). It has been suggested that teachers are generally positive about delivering such programs, but that there are issues with available resources (Graham et al., 2011). This was apparent in the teacher feedback that was received in this study, with time and competing demands being cited as the most common reason for incomplete lessons.
It has also been observed that greater stress in teachers relates to lower adherence in the delivery of evidence-based programs (Ouellette et al., 2018). At the time this program was delivered, teachers were particularly impacted by COVID-19. Teacher stress increased during the pandemic (Kotowski et al., 2022) which may have had an impact on the delivery of GWG in this study. While it remains true that teachers are well-placed to deliver universal prevention, there are challenges in how this is carried out practically.
In the context of this study, it is possible that greater support was needed throughout the program delivery for facilitators (e.g. follow-up training or mentoring). It is worth noting, however, that there was a large amount of communication between researchers and teachers during the program delivery (such as emails for key milestones, reminders to complete fidelity surveys, etc.). It appears teachers wanted to deliver the program but that other factors (e.g. time and competing curriculum demands) inhibited their capacity, rather than uncertainty about program delivery.
Even considering the low dosage students received, there did appear to be improvement in mean scores (on the RCADS) for participants who were above the clinical cut off at baseline. By post-intervention in the GWG condition, the mean RCADS of this subgroup dropped below the clinical range, while this was not true for the control condition. This points to the possibility that the program was beneficial for those who presented with symptoms of anxiety and depression at baseline. No formal analyses could be performed due to subgroups being statistically underpowered, but this raises the possibility that the program may be more effective for at-risk children.
The benefit found for students above clinical cut offs could point to ceiling effects, or perhaps that the program is better suited as an intervention tool. Previously it has been demonstrated that targeted interventions are more effective for depression than universal prevention (Werner-Seidler et al., 2017), but as discussed, there are issues with targeted interventions in the school context (e.g. stigmatisation and cost). For this reason, better strategies are needed to support children who are at-risk, that are not resource intensive and stigmatising. For example, introducing GWG as a stepped care tool, as the first step prior to targeted intervention.
Research in the field of implementation science has brought forward some suggestions for improving the delivery of programs in schools, which could benefit teachers and students, and address some of the issues found in this trial. These include assessing the readiness of the school itself as well as the needs of that school community, finding a school champion for the program, and adapting and tailoring the program in partnership with the specific context (Cook et al., 2019). The focus of these recommendations is to customise program delivery to the unique school community which, while challenging for the research context, is perhaps the most appropriate way to address the reality that programs in schools need to be suited to the school, teachers and students.
Limitations
There are several limitations to this work to highlight. School attendance impacted the participation in data collection; there was very little genuine attrition, but high absences due to illness. Additionally, there was a lower number of classes recruited than planned, therefore subgroups were underpowered. Schools were recruited during the COVID-19 pandemic, further complicating this process. Classes were randomly allocated to GWG or to the control group, however, the classes allocated to the control were typically smaller which may have limited the results. There were, however, no statistically significant differences in response rates between the conditions. Schools in the study included different socioeconomic areas, school types (independent and government) and locations (regional and urban), but it is important to mention that the sample was a sample of convenience which may limit the generalisability of the findings. One of the potential limitations of GWG is the number of topics included across the Five Habits. The program may benefit from refining the focus to a smaller number of the Habits to allow time to develop the related skills. Finally, allocation occurred at the classroom-level rather than school-level, increasing the risk of contamination (as children interact within their school more than between schools), as school-level allocation requires many more schools which was not feasible in this research.
Future directions
The GWG program was not effective in this trial; however, there are gaps in this field of research that have become clear. Primarily, there is an urgent need for better support for teachers in implementing universal programs, especially when they are tasked with mental health support for students. Schools have been identified as key locations for addressing mental health concerns, and teachers are well-placed to deliver evidence-based content (e.g. Humphrey, 2023); however, teachers cannot do so effectively with the current level of support and resources provided to them. Ensuring adequate support for teachers is a concern for school leadership, researchers and policy makers. Furthermore, even when given support, teachers’ own levels of stress impacts the delivery of such programs (Ouellette et al., 2018). Future work needs to consider how teachers’ mental health can be addressed, considering initial findings that teacher mental health and wellbeing has an impact on various student outcomes (e.g. Maricuțoiu et al., 2023; McLean et al., 2023; Ouellette et al., 2018). The reasons for poor fidelity is this study are not clear; thus, future research would benefit from gathering further qualitative data from teachers on the strengths and weaknesses of the program and how implementation could be improved from their perspective.
This trial also provides scope for the GWG program to be reimagined as focussing on children who are currently demonstrating symptoms of anxiety and depression. Such adaptations might include applying GWG as a stepped care tool, though this approach requires further investigation. It could also be beneficial to include parent/caregiver and teacher reports of children’s functioning as potential outcomes in further research.
These findings shed light on how a universal prevention approach could be challenging to implement depending on the school context, and therefore might do a disservice to children in need of intervention and prevention. Future research should consider an approach that better suits the needs of primary-school students, teachers, and schools.
Conclusions
This trial uniquely contributes to the literature an evaluation of a mental health prevention using a positive psychology approach, specifically aimed at primary-school-aged children. GWG was not effective in this trial; however, poor implementation fidelity significantly impacted the conclusions that can be drawn. There were signs that GWG might be useful for children who present with symptoms of anxiety and depression which might suggest a future application. Nonetheless, further research is urgently needed, particularly studies with improved implementation fidelity. Primary schools provide a valuable context to address the concerning rates of mental illness in children, but consideration must be given to implementing preventative programs that are feasible in the school context.
Footnotes
Acknowledgements
Ash Manuel provided access to the Growing with Gratitude program. Aline Kunnel performed statistical analysis. We would also like to acknowledge the schools and students who took part in this project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author was previously employed at one of the schools involved in this trial (not employed during the trial).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by an Australian Government Research Training Program (RTP) Scholarship. No further funding was received.