
Abstract
Mental disorders are among the most common and disabling conditions affecting children and adolescents. Patterns of school attendance among students with and without mental disorders were examined using data from the 2013–2014 Australian Child and Adolescent Survey of Mental Health and Wellbeing. One in seven school students had a mental disorder in the previous 12 months, with attention-deficit/hyperactivity disorder and anxiety being the most common. Students with a mental disorder had lower school attendance – being absent for 11.8 days per year in Years 1–6, 23.1 days per year in Years 7–10 and 25.8 days per year in Years 11–12, on average. In comparison, students without mental disorders were absent an average of 8.3 days (Years 1–6), 10.6 days (Years 7–10) and 12.0 days (Years 11–12) per year. Among students with a mental disorder, absences due to the disorder accounted for 13.4% of all days absent from school. This increased across years in school from 8.9% in Years 1–6 to 16.6% in Years 11–12. Improving prevention, early intervention, treatment and management of mental disorders may lead to significant improvements in school attendance.
Introduction
Regular attendance at school is recognised worldwide as a key component of engagement in schooling and an important pre-requisite for academic success (Gottfried, 2009; Hancock, Lawrence, Shepherd, Mitrou, & Zubrick, 2016). Much of the literature on school non-attendance, or absenteeism, has focussed on three areas, namely truancy, school refusal and chronic absenteeism. While there is a lack of consistency in defining these terms, truancy is generally considered to be regular absence from school without permission or justification, usually without the knowledge of the child’s parents or carers (Maynard, McCrea, Pigott, & Kelly, 2012). On the other hand, chronic absenteeism is generally defined as students being absent more than a set proportion of days (e.g. 10% or 20%) due to chronic ill health or other reasons, with the knowledge of the child’s parents (Balfanz & Byrnes, 2012). Finally, school refusal has traditionally been defined as children refusing to attend school due to severe emotional distress or fear (Berg, Nichols, & Pritchard, 1969; Kearney, 2008).
Historically, the focus of attendance research has been on truancy as a behavioural issue (Brown, 1983). More recently, it has been recognised as being related to oppositional behaviours, more so since education systems developed broader attendance policies.
What has been demonstrated for each of truancy, chronic absenteeism and school refusal, however, is their links to mental health and life outcomes. For example, chronic absenteeism and persistent truancy are related to a range of negative life outcomes including school dropout, unemployment, poverty, substance use and contact with the criminal justice system (Henry & Huizinga, 2007; Reid, 1999; Wilson, Malcolm, Edward, & Davidson, 2008). Chronic absenteeism has also been shown to be associated with concurrent poor mental health (Kearney, 2008; Merry & Moor, 2015; Wood et al., 2012).
Mental health problems are among the most common disabling health conditions in children and adolescents. In 2001, the World Health Organization predicted that childhood and adolescent mental health problems would become one of the leading causes of morbidity, mortality and disability worldwide by 2020 (World Health Organization, 2001). This was supported by the 2004 Global Burden of Disease study which reported that neuropsychiatric disorders were responsible for 21.8% of total burden of disease among 0- to 14-year-olds in high-income countries, as measured by disability-adjusted life years (Gore et al., 2011). By 2012, approximately 20% of adolescents reported experiencing a mental health problem in any given year (World Health Organization, 2014). More recently, a comprehensive meta-analysis reported that 13.4% of children and adolescents worldwide suffer from mental health disorders in a 12-month period (Polanczyk, Salum, Sugaya, Cave, & Rohde, 2015).
In Australia, results from the recent Young Minds Matter: the second Australian Child and Adolescent Survey of Mental Health and Wellbeing (YMM) revealed that one in seven (or 560,000) Australian children aged 4–17 years met diagnostic criteria for a mental disorder in the past 12 months (Lawrence et al., 2015). Attention-deficit/hyperactivity disorder (ADHD) and anxiety disorder were the most common (7.4% and 6.9%, respectively), with major depressive disorder having the greatest impact on daily living – 43% of respondents who experienced it reported severe impairment of functioning. For young people, a significant proportion of the daily adaptive functioning revolves around attending school and mental health problems have the potential to impact school attendance and dropout (Dray et al., 2017; Neufield, Dunn, Jones, Croudace, & Goodyer, 2017).
There is very little research addressing the impact of mental health problems on attendance more generally, as most previous studies have focussed on truancy, chronic absenteeism and school refusal. Often these studies have drawn their samples from students referred to specialist programs for truancy or school refusal. Not surprisingly, studies based on samples of children referred to specialist mental health services as a result of truancy or school refusal behaviour have found that most such children meet diagnostic criteria for a mental disorder, although this includes a wide range of disorders including anxiety disorders, mood disorders and disruptive behaviour disorders (see Kearney & Albano, 2004; McShane, Walter, & Rey, 2001). One of the few previous population-based studies is the Great Smoky Mountains Study (N = 4500 aged 9, 11 or 13 years at baseline and followed longitudinally for over 20 years). The findings showed that anxious school refusal was associated with depression and separation anxiety disorder, while truancy was associated with oppositional defiant disorder, conduct disorder and depression (Egger, Costello, & Angold, 2003).
While most of the existing literature has focused on truancy, school refusal or chronic absenteeism, this paper examines absenteeism in general as well as chronic absenteeism (as defined by absences of more than 20% or 30% of school days). It was previously considered that students who are absent infrequently can readily ‘catch up’ on missed schoolwork on return to school, while persistent absence or chronic absenteeism may substantially disrupt students’ education (Coventry, Cornish, Cooke, & Vinall, 1984; McCluskey, Bynum, & Patchin, 2004; Zubrick et al., 1997). More recent evidence suggests that higher rates of attendance are associated with higher levels of academic achievement, and that school performance declines consistently with increasing rates of absence from school with no evidence of a threshold effect (Gottfried, 2010; Hancock, Shepherd, Lawrence, & Zubrick, 2013). It is possible that absences from school that are due to mental health issues could re-inforce poor mental health through a self-perpetuating cycle. If absence from school is associated with reduced levels of connectedness, engagement and academic performance, these could further exacerbate mental health issues leading to further absence from school if the cycle is not disrupted. Therefore, given that childhood and adolescence are precarious times for the development of psychopathological symptoms through to full-blown mental disorders (Lee et al., 2014) and that such disorders have an impact on school attendance, establishing the rates of absenteeism associated with specific mental disorders is important.
Study objectives
This study set out to describe patterns of attendance for students with common mental disorders, using a random sample of children and families in Australia from the population of families with children aged between 4 and 17 years living in Australia. The objectives of this study were to ascertain: (i) the number and proportion of days absent from school in students with and without mental disorders by gender and year level in school, (ii) whether or not different mental disorders are associated with different numbers of days absent from school, (iii) the number and proportion of days absent from school due to symptoms of mental disorders and (iv) the proportion of students with and without mental disorders who meet criteria for chronic absenteeism.
Method
Source data
Data were drawn from YMM. Full details of the survey methodology have been published elsewhere (Hafekost, Johnson, et al., 2016; Hafekost, Lawrence, et al., 2016). Briefly, a random sample of 6310 families with children aged 4–17 years was selected from around Australia. Data were collected by means of face-to-face interviews with the primary carer of each selected survey child. Where the selected child was aged 11 years or over, they also completed a self-report questionnaire on a tablet computer. The response rate to the household survey was 55%, and 89% of eligible adolescents in these households completed the self-report questionnaire. The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee and The University of Western Australia Human Research Ethics Committee.
The present analysis is based on 5041 survey children who were attending an Australian school in Years 1–12. The remaining 1269 survey participants were excluded from the study. The excluded participants included 1129, 4- to 6-year-olds who were attending kindergarten or equivalent pre-primary programs, a Preparatory or foundation year or who had not started formal schooling, along with 81, 16- to 17-year-olds who had left school, 15 children who were home schooled and 9 children who were not attending school for various reasons. The primary carers of 35 students reported that they did not know whether their child had been absent from school during the current school year and these students were also excluded from this analysis.
Measures
Mental disorders
Mental disorders were assessed using the Diagnostic Interview Schedule for Children Version IV (DISC-IV) (Fisher et al., 1993; Shaffer, Fisher, Lucas, Dulcan, & Schwab-Stone, 2000). The DISC-IV is a structured interview that assesses diagnostic criteria for mental disorders as specified in the Diagnostic and Statistical Manual for Mental Disorders Fourth Edition (DSM-IV; American Psychiatric Association, 2000). The DISC identifies whether a child meets criteria for a diagnosis of mental disorder during the past 12 months. These criteria include assessing the number, type, frequency and persistence of symptoms and the degree of functional impairment that is associated with these symptoms. Seven disorders were assessed in the survey. These included four anxiety disorders (social phobia, separation anxiety disorder, generalised anxiety disorder and obsessive-compulsive disorder), major depressive disorder, ADHD and conduct disorder. These disorders were selected based on the prevalence and impact of these conditions on children and adolescents as reported in the literature (Hafekost, Lawrence, et al., 2016; Polanczyk et al., 2015).
Days absent from school
The survey questionnaire included an education module in which primary carers were asked whether or not their child went to school, and if so, which grade they currently attended. Children were considered as attending school if they were currently enrolled in Years 1 through 12. Children who had not begun formal schooling or who were attending a post-secondary education or training provider/institution were considered to not be attending school. For children attending school, carers were also asked how many days their child had been absent from school since the start of the school year, excluding school holidays. Based on the date of the interview, the number of school days in the school year in that jurisdiction to that point was calculated. Attendance rates were calculated based on reported days absent and the number of possible days attended. This attendance rate was then extrapolated to a full school year on a pro-rata basis. For example, if the interview was conducted on the 165th day of the school year and the child had been absent for 9 days to that point, the child would be estimated to have been absent for 12 days over a full school year of 220 days. This procedure allowed for number of days absent to be compared across students on a consistent basis.
As part of the DISC-IV, carers who reported that their child had mental disorder symptoms were asked how many days their child had been absent from school specifically due to the symptoms they had reported. Where a child met all the criteria to establish a diagnosis of a mental disorder based on the DSM-IV criteria, the number of days absent due to mental disorder symptoms was regarded as number of days absent due to a mental disorder for this analysis. Where the child did not meet all the diagnostic criteria for a mental disorder, the number of days absent from school due to symptoms of mental disorder was not used, and the number of days absent due to a mental disorder was treated as zero. Thus, the impact of sub-clinical symptoms on absenteeism has not been considered in this analysis.
Statistical analysis
Survey data were weighted to represent the full Australian population of school students aged 4 to 17 years and to adjust for patterns in non-response. A detailed analysis of non-response patterns in the survey has been reported separately (Hafekost, Lawrence, et al., 2016). Briefly, it was identified that families with children aged 7 years or younger or with more than one child aged 4 to 17 years were found to be more likely to participate in the survey. Additionally, 16- to 17-year-olds were specifically oversampled in the survey due to particular interest in measuring the onset of mental health problems at these ages. The weighting adjusts for each of these factors in addition to adjusting for the original survey sample design.
The survey sample was drawn in two stages, resulting in a clustered sample. At the first stage, a series of Statistical Area 1 (SA1) areas was selected. These are small geographic areas, averaging around 250 households, which were designed for use in the Australian Census of Population and Housing and to facilitate large-scale sample surveys. Families with children aged 4 to 17 years were then picked within the selected SA1 areas to identify the final sample. Both the clustering and weighting were accounted for during analysis of the data. Survey estimates and associated confidence intervals have been calculated using these weights and accounting for the clustered survey design using the method of Taylor Series Linearisation (Wolter, 2007).
The average number of days absent from school was calculated for all students, by year level in school (grouped as Years 1–6, Years 7–10 and Years 11–12) and by sex. We also calculated the prevalence of mental disorders by year level in school and by sex. The average number of days absent from school was calculated separately for students with and without mental disorders. For students with a mental disorder, the average number of days absent from school specifically due to symptoms of mental disorders was also calculated. Using these averages, we estimated the total number of days absent from school across each year level group, and the total number of days absent due to a mental disorder. These estimates were used to calculate the proportion of days absent from school that could be attributed to mental disorders. These proportions were first calculated only for those students who had a mental disorder, and secondly, for all students. The latter proportions were used to estimate the relative contribution of mental disorders to absence from school.
Finally, the proportion of students who had been absent for more than 20 days, or absent for more than 30 days, during the school year according to school, sex and year level was calculated as an indicator of chronic absenteeism.
Results
The unweighted distribution of the sample by key characteristics is shown in Table 1. The sample in the analysis included a disproportionately higher number of students in Years 10–12, due to the oversampling of 16- to 17-year-olds in the survey sample. The survey weights adjust for this feature of the survey design. As shown in Table 1, approximately one in seven (14.5% unweighted, 14.7% weighted) of students met diagnostic criteria for one or more mental disorders in the 12 months prior to the survey. Anxiety disorders and ADHD were the two most common mental disorders in Australian school students. About 8% of the survey sample had missed no days of school in the past year, 61% had been absent 1–10 days, 19% had been absent for 11–20 days and 12% had been absent for more than 20 days of a maximum of 220 days in the school year.
Characteristics of students in the sample.
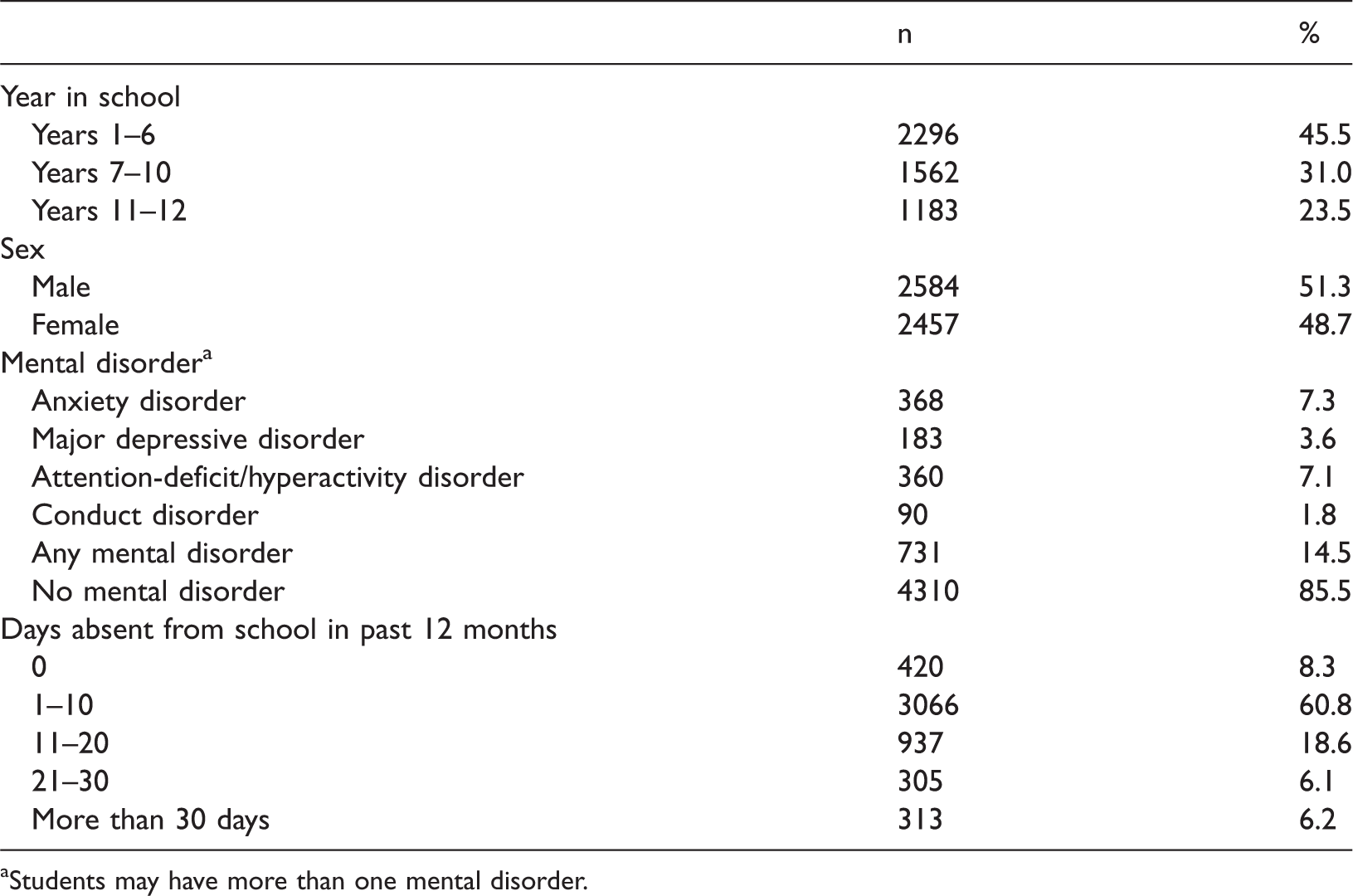
Students may have more than one mental disorder.
The prevalence of mental disorders did not vary greatly between Years 1–6 (15.4%), Years 7–10 (14.6%) and Years 11–12 (13.0%) (see Table 2). In most Australian jurisdictions and schools, Years 1–6 correspond to primary school and Years 7–12 correspond to secondary school. While the overall prevalence of disorder was similar across school year levels, the nature of disorder varied. ADHD was more common in younger students than older students and more common in males than in females (see Table 3) while major depressive disorder was more common in older students than younger students and more common in females than in males.
Days absent from school, prevalence of mental disorder, days absent attributed to mental disorder and proportion of total days absent that were due to mental disorder by year level (proportion (95% Confidence Interval)). a
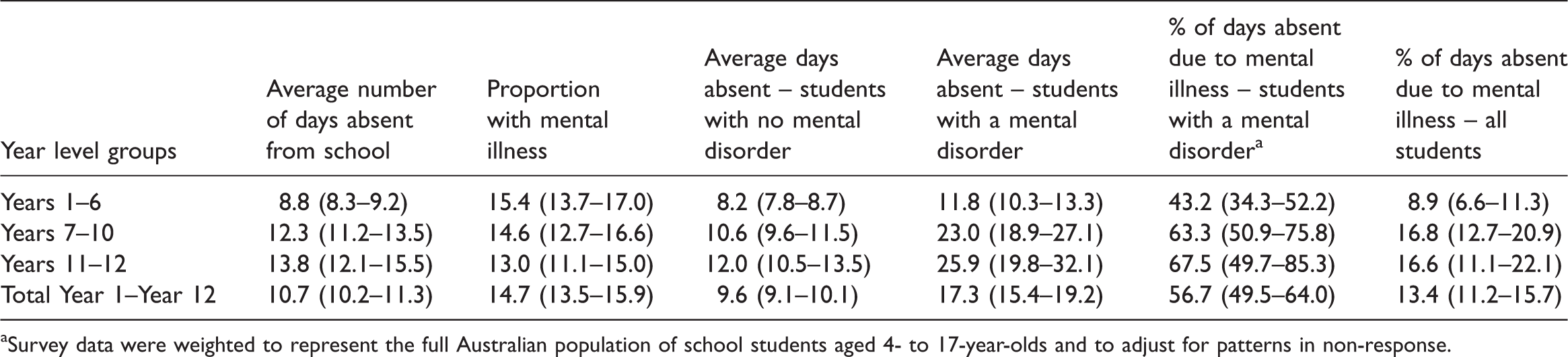
Survey data were weighted to represent the full Australian population of school students aged 4- to 17-year-olds and to adjust for patterns in non-response.
Prevalence of mental disorder, average days absent from school and average days absent due to mental disorder, by mental disorder, year levels and sex. a
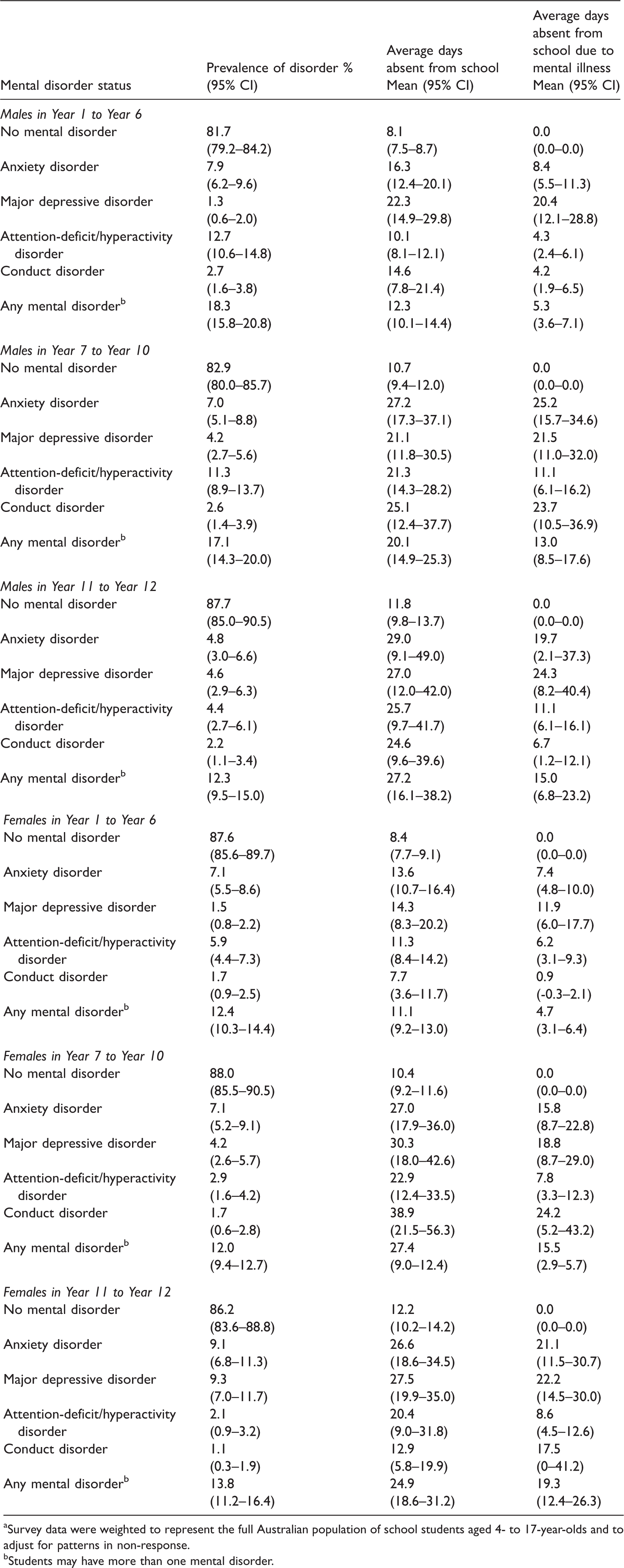
Survey data were weighted to represent the full Australian population of school students aged 4- to 17-year-olds and to adjust for patterns in non-response.
Students may have more than one mental disorder.
Some students may have more than one mental disorder. Of the students with at least one mental disorder in the past 12 months, 30% met diagnostic criteria for more than one disorder. Students with one or more mental disorders had higher rates of absence from school. In Years 1–6, students with no mental disorder were absent an average of 8.2 days per year (95% CI: 7.8–8.7), students with one mental disorder were absent on average 10.7 days per year (95% CI: 9.0–12.3) and students with two or more disorders were absent on average 15.0 days per year (95% CI: 11.6–18.5). In Years 7–12, students with no mental disorder were absent an average 11.0 days per year (95% CI: 10.2–11.8), students with one mental disorder were absent on average 21.6 days per year (95% CI: 17.8–25.5) and students with two or more disorders were absent on average 28.3 days per year (95% CI: 21.5–35.1).
In 2013, the national attendance rate, defined as the number of actual full-time equivalent student-days attended by full-time students in Years 1 to 10 as a percentage of the total number of possible student-days attended in semester 1 in each school year, was 93.6% in Years 1–6 and 91.3% in Years 7–10. National attendance rate data are not reported for Years 11–12 (Australian Curriculum, Assessment and Reporting Authority, 2016).The number of days absent estimated in the current study expressed as attendance rates were 95.5% in Years 1–6 (95% CI: 95.3–95.7) and 93.7% in Years 7–10 (95% CI: 93.1–94.3).
As shown in Figure 1, on average, student absence rates increased over the school years, from 8.8 days per year in Years 1–6 to 13.8 days per year in Years 11–12. These figures were broadly comparable to those based on administrative school data (see Hancock et al., 2013). On average, students with a mental disorder were absent for more days than students without a mental disorder and the size of the difference increased over the school years. In Years 1–6, students without a mental disorder missed an average of 8.2 days per year while those with a mental disorder missed 11.8 days, a difference of 2.6 days. In Years 11–12, students without a mental disorder missed an average of 12.0 days per year while those with a mental disorder missed an average of 25.9 days, a difference of 13.9 days (Figure 1). Among students with a mental disorder, days absent due to the mental disorder as a proportion of all days absent represented 13.4% of all days absent from school. This increased across years in school from 8.9% in Years 1–6 to 16.6% in Years 11–12 (see Table 2).
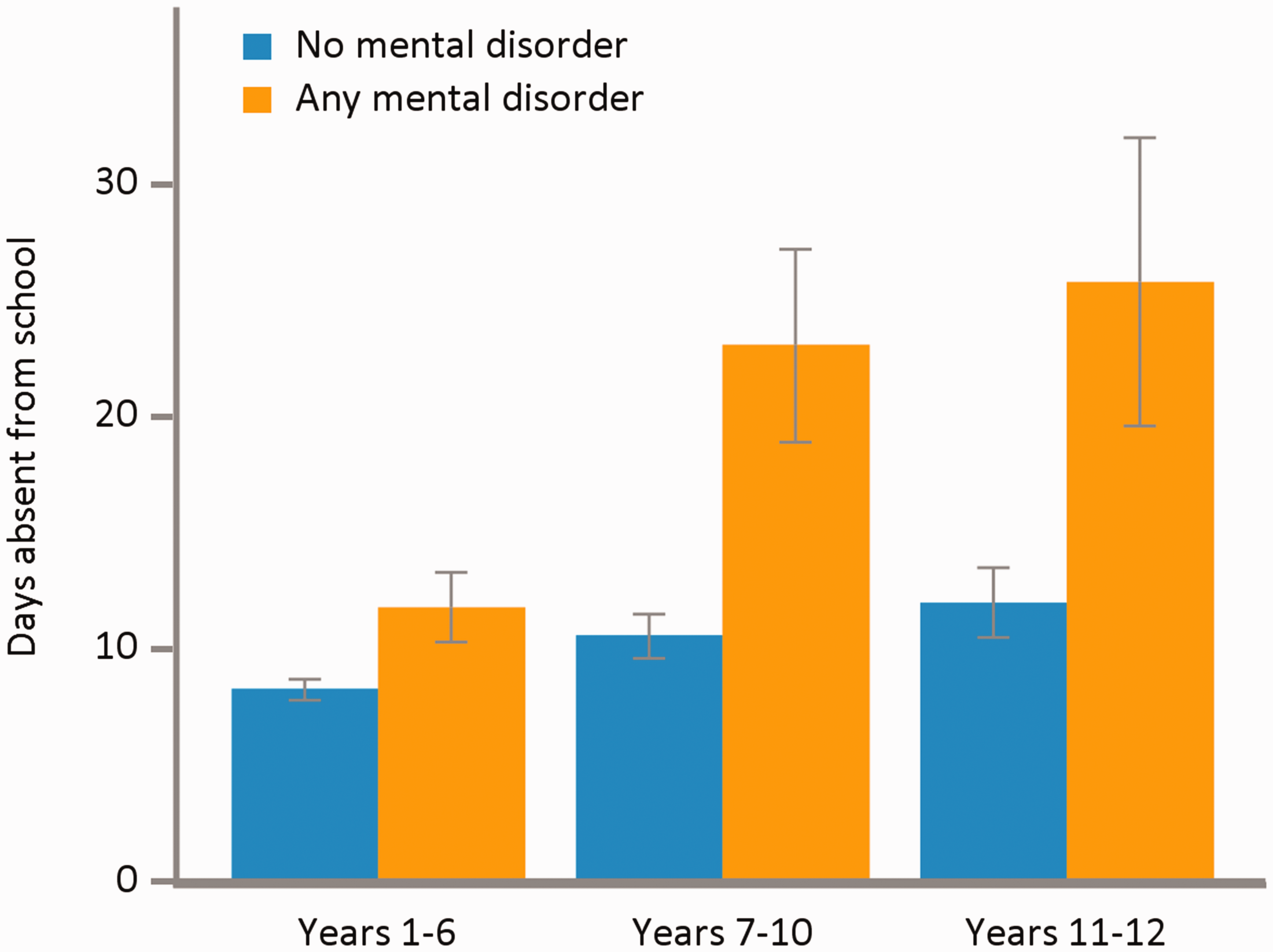
Average number of days absent from school, by year level groups and mental disorder status.
The average number of days absent from school varied by type of mental disorder, although the differences between major depressive disorder, anxiety disorders and conduct disorder were not statistically significant. While the prevalence of major depressive disorder is low in children of primary school age, its functional impact can be substantial. As can be seen in Table 3, in the secondary school years, anxiety disorders, major depressive disorder and conduct disorder are all associated with similarly high levels of absenteeism.
In the secondary school years, over one-fifth of males and one-third of females with a mental disorder were absent for more than 20 days in the course of the school year (i.e. chronic absenteeism). In contrast, around one in every ten secondary school students without a mental disorder missed this many days of school (see Table 4).
Proportion of students absent for more than 20 days or more than 30 days during the school year, by mental disorder, year level group and sex. a
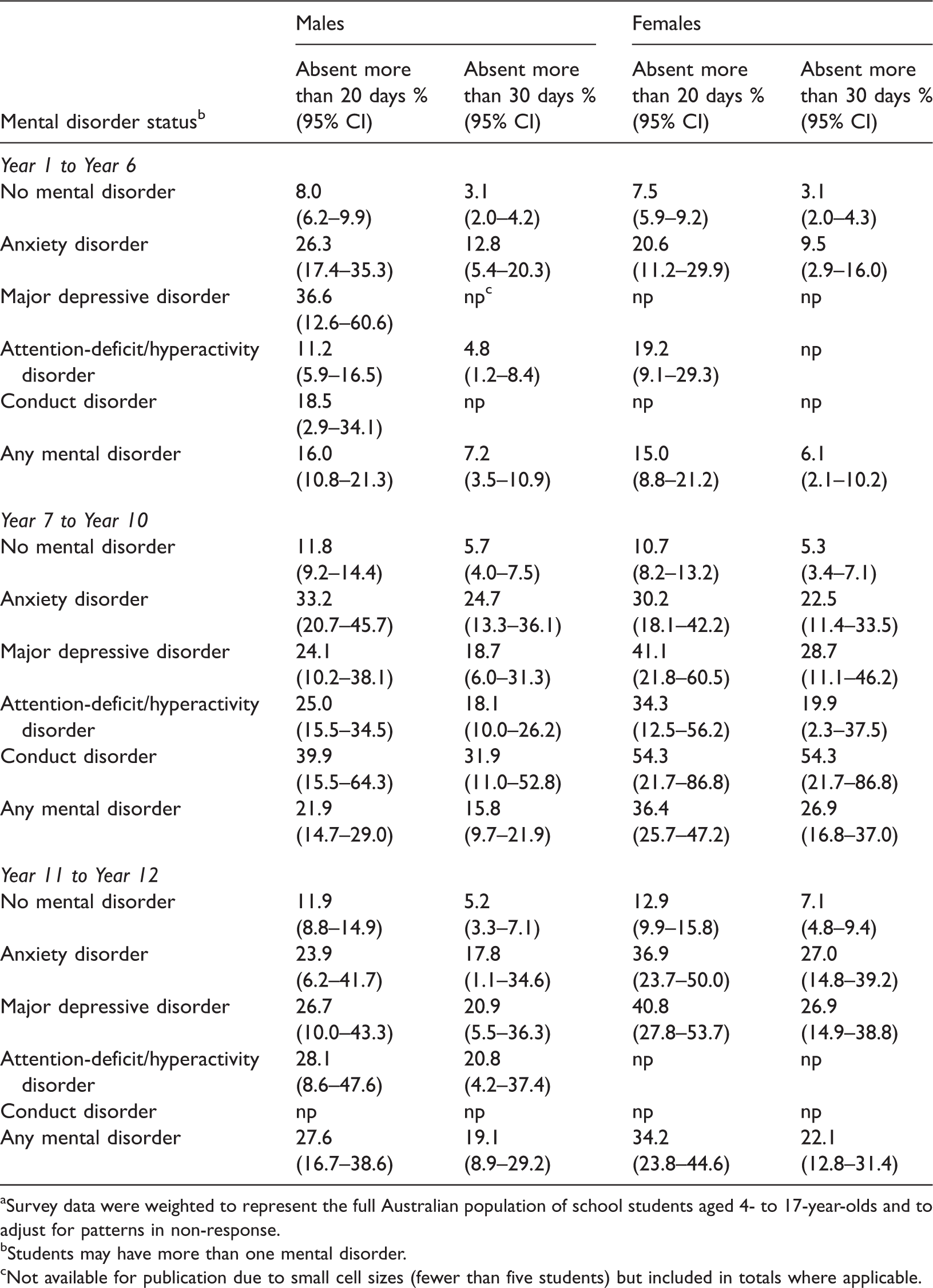
Survey data were weighted to represent the full Australian population of school students aged 4- to 17-year-olds and to adjust for patterns in non-response.
Students may have more than one mental disorder.
Not available for publication due to small cell sizes (fewer than five students) but included in totals where applicable.
Discussion
Data from YMM have shown that students with mental disorders have lower school attendance, and symptoms of these mental disorders are a major reason for absences from school. For each of the mental disorders considered in the survey, average attendance rates for students with a disorder were lower than for students without a mental disorder. These differences were particularly noticeable in the secondary school years, where days absent due to symptoms of mental disorders represented over 16% of all absences from school. While some students with mental disorders did not miss any days of school, others missed substantial numbers of school days. Around one-fifth of males and one-third of females in secondary school with a mental disorder have missed more than 20 days of school. This level of absence can be considered substantial, as it is likely to have a significant impact on students’ learning, which may place their mental health and other outcomes at further risk (Gottfried, 2009; Hancock et al., 2016).
In Australia, where school attendance is compulsory to at least age 17 years, attendance policy is set at the school system level. Each State or Territory has its own Education department responsible for overseeing public schools whereas policy for Catholic and Independent schools can be set at the state, diocese, or individual school level. These policies generally confirm the compulsory nature of school attendance and set procedures for reporting of allowable absences and follow-up for unexplained absences. In addition, some jurisdictions have developed policies and tools aimed at promoting the importance of attendance at school. For instance, the Queensland Government Department of Education and Training has developed the ‘Every day counts’ strategy, which is focused on promoting the importance of attending school every day, with a range of resources targeting students, parents and school communities (Queensland Government Department of Education, Training and Employment, 2016). These include strategies to communicate expectations around attendance to students and families, through regular communication with students and their parents, strengthening relationships between schools and families and improving student connectedness to school. Resources available include a web site (Queensland Government Department of Education and Training, 2017), videos, posters and a comic book. Other jurisdictions including Victoria, Western Australia and the Northern Territory have also produced strategies under the banner ‘Every day counts’ (e.g. Northern Territory Department of Education, 2016).
Kearney and Graczyk (2014) have recently outlined a multi-tier model for the promotion of school attendance and decreasing absenteeism. Their model has three tiers – a framework for promoting regular attendance for all students (Tier 1), targeted interventions for at-risk students (Tier 2) and intensive interventions for students with chronic absenteeism (Tier 3). They have identified the support of mental health and social and emotional wellbeing as key strategies in both Tier 1 and Tier 2. These strategies are recommended to include both health promotion and prevention strategies as well as school-based mental health services. Health promotion and mental health prevention strategies may help build resilience, help students learn and develop strategies for managing and improving their mental health and wellbeing as well as help students to understand when they should seek additional help and how to do so (Australian Government Department of Health, 2014; Slee et al., 2009). Strategies that improve student mental health and wellbeing may also improve student attendance at school (Hoagwood et al., 2007).
Reasons cited for school absence related to mental disorders may include medical illness (either somatic or comorbid physical conditions), suspension or expulsion, juvenile detention or family issues and peer problems (e.g. bullying). While disruptive behaviours such as conduct disorder and ADHD (categorised as Disruptive, Impulse-Control, and Conduct Disorders in DSM 5) may be expected to have an impact on school attendance due to behaviour management issues, which may result in exclusion from school, anxiety disorders and depression are common in Australian school students and are associated with significant absence from school. In the literature, this has primarily been reported in relation to school refusal behaviour (Egger et al., 2003; Kearney, 2008). However, absence due to anxiety disorders may also manifest as somatic complaints about physical conditions. The underlying reasons for absences related to mental disorders vary and, as a result, the strategies implemented to improve school attendance and ultimately academic achievement will also need to vary.
Absenteeism in the primary school years (Years 1–6) can mean that children are missing out on developing the basic literacy and numeracy skills that they need for future learning (United States Department of Education, 2016). These children may also miss out on opportunities to develop the higher order critical thinking and reasoning skills that would enable them to problem solve in the later years of schooling and beyond (Gottfried, 2014). From a social perspective, young children also miss out on developing important social and collaborative skills (Balfanz & Byrnes, 2012). In the early secondary school years (Year 7–10), students learn foundational content knowledge and skills as well as further develop their cooperative skills, usually through group work. Adolescents who are frequently absent are less likely to develop the foundational knowledge needed to continue with university entry subjects, particularly science and mathematics, and are likely to have fewer opportunities to form productive relationships with their peers and teachers (Commissioner for Children and Young People, 2018). Gaps in learning due to absenteeism may have a deleterious impact in upper secondary school where the curriculum builds on students’ prior knowledge and skills from lower secondary school.
Academic achievement can be improved for students with poor attendance when school leaders, teachers and other education staff have a belief that every child is capable of success and consequently demonstrate a commitment to assisting students regardless of the reason for absenteeism (Rubie-Davies, Hattie, & Hamilton, 2006). Where possible, teachers and school leaders can assist students by working with parents/care givers and school support staff (e.g. school psychologist, counsellors, chaplains) to support students as they return to school. Specifically, teachers can provide catch-up work and access to online study materials (e.g. Khan Academy), use differentiated strategies and adjust assessment schedules and types (Skinner & Belmont, 1993). For example, students may be able to complete a take-home paper assignment as an alternative to an in-class test. In class, teachers can ensure that their classroom environments are safe and welcoming for all students.
Strengths, limitations and future directions
This study was based on a large, nationally representative population sample, as part of the Australian Government’s National Survey of Mental Health and Wellbeing initiative, with detailed interviews conducted face-to-face by trained interviewers. Data are based on parent report and are subject to recall errors. As these data are based on parent report, school truancy without the parent’s knowledge will not be captured. However, the average number of days absent estimated from the survey was comparable to figures estimated from school administrative attendance records.
It should be acknowledged that mental and physical health problems may be comorbid. While the survey asked parents for number of days absent due to symptoms of mental disorder, it did not ask if the child also had comorbid physical health problems which may have also contributed to the absences from school.
Conclusion
Mental disorders are a significant cause of student absence from school, particularly in the secondary school years. While school attendance strategies have focussed on identifying truancy and school refusal behaviour, early identification and appropriate management of mental disorders may also help to improve general school attendance.
Footnotes
Acknowledgements
The authors would like to thank the over 6000 families that gave their time to participate in the survey; Rajni Walia, Gerry Bardsley and the team at Roy Morgan Research who undertook the data collection; and the Survey Reference Group for their input into the design and conduct of the survey.
Data Access Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health, with additional funding from the Australian Government Department of Education.