
Abstract
Recent Australian data from the Programme for International Student Assessment (PISA) indicate that around 14% of children are performing poorly on reading. Comparisons with earlier data show that the relative numbers of Australian children with low reading status have not declined in this century. This is despite a surge of robust research documenting evidence-based principles that should guide reading intervention for children who make a poor start in learning to read. In this article, we outline an integrated model of best practice based on empirical research, and contrast this with current practices in schools in the Australian state of Victoria to support poor readers. Practices appear to comply with a model of early identification of reading difficulty and an intensive intervention program in early school years. However, significant shortcomings are apparent in the theoretical orientation of some interventions, the resourcing of reading intervention programs and intensity and continuity of intervention for children with persisting difficulty. We suggest that major changes are required to support vulnerable readers at school.
Keywords
Introduction
Large numbers of Australian children are not reaching expected standards of reading competency (e.g., Buckingham, Wheldall, & Beaman-Wheldall, 2013; ‘Teaching Reading: Report and Recommendations’, 2005; Thompson et al., 2011; Wheldall, 2013). In the 2013 National Assessment Program for Literacy and Numeracy (NAPLAN), 13.4% of year 3 Australian children were at or below the expected national minimum standard expected (National Assessment Program—Literacy and Numeracy Summary Report, 2013). Further, the most recent assessment of reading literacy among 15-year-old students conducted by the Programme for International Student Assessment (PISA) in 2013 found 14% of Australian students were low performers, and this figure was not significantly different to that reported in 2000 (Thompson, De Bortoli, & Buckle, 2013, p. 195). Nevertheless, it is reported that only between 1% and 6% of children present with inherent phonological processing difficulties that predispose them having difficulties in learning to read (de Lemos, 2013; Friend, DeFries, & Olson, 2008; Torgesen, 2000). Many other children experience difficulties in learning to read arising from various environmental factors such as having limited experiences with spoken or written text prior to school entry, coming from a low socioeconomic background, or – more alarmingly for educators – not receiving the most effective and evidence-based reading instruction once at school (Buckingham et al., 2013; Buckingham, Wheldall, & Beaman, 2012; Friend et al., 2008). Evidence suggests that regardless of the pathway(s) leading to children’s difficulties in learning to read, the principles of the intervention are the same (de Lemos, 2013). In this article, we discuss in an Australian context the current problems in regards to providing reading intervention to those children who make a poor start in learning to read at school. We use theoretical and recent empirical evidence to challenge current practices and propose alternative models of intervention and service delivery to address the needs of young low-progress readers.
The low-progress reader
Reading involves the ability to decode and recognise printed words and make sense of written text (Buckingham et al., 2013; de Lemos, 2013). Many would argue that a central although not exclusive component of teaching children to read is the explicit and systematic teaching of phoneme-grapheme correspondences in order to gain mastery of the alphabetic code (Adams, 1990; de Lemos, 2013; Juel, 1988; Vellutino, Fletcher, Scanlon, & Snowling, 2004). Supplementary reading intervention for low-progress readers must also adopt an explicit, systematic approach but with even greater structure and intensity of instruction.
There is considerable agreement that children who present with reading difficulty at an early age will not meet year-level expectations when receiving only regular classroom education (Spira, Bracken, & Fischel, 2005; Stanovich, 1986). In fact, it is widely reported that – over time – the gap between typical and low-progress readers is either maintained (Catts, Sittner Bridges, Little, & Tomblin, 2008; Lonigan, Purpura, Wilson, Walker, & Clancy-Menchetti, 2013) or widens (Stanovich, 1986). Apart from the academic consequences associated with a widening gap in reading performance, low-progress readers are vulnerable to a range of longer term psychosocial difficulties including lowered self-esteem and an increased susceptibility to antisocial behaviour and delinquency (Beitchman et al., 2001; Jenkins & O’Connor, 2002; Morgan, Farkas, Tufis, & Sperling, 2008; Morgan, Fuchs, Compton, Cordray, & Fuchs, 2008). Accordingly, supplementary reading intervention is a critical area of educational practice from an educational, ethical and economic perspective.
In recent years, reading difficulty has emerged as a public health issue in academic literature (Roberts, Price, & Oberklaid, 2012; Snow & Powell, 2004), public media (Harrison, 2009; Milburn, 2004; Tarica, 2009) and in government-commissioned reports. Dr Ken Rowe, who headed the Australian government-commissioned report titled ‘National Inquiry into the Teaching of Literacy’ was cited in Milburn’s (2004) newspaper article saying: ‘… psychology clinics at hospitals were straining to cope with the deluge of children seeking medical attention for problems caused by their failure to learn to read’.
The ideal model of reading intervention for low-progress readers
A considerable amount of priming can and should occur for children prior to school entry to optimise the formal process of learning to read. These aspects will not be addressed in this article. Rather we will first describe models of best practice for supporting low-progress readers at school, followed by an exploration of barriers and facilitators to the implementation of such an approach in an Australian context.
Ideally, the school network would support low-progress readers to close their reading gap and aim to meet year-level expectations. Importantly, this support would be provided early in the child’s schooling since once the reading difficulty is entrenched, the required support is likely to be beyond the scope of classroom reading instruction alone (Reynolds, Wheldall, & Madelaine, 2010).
The core components for effective classroom reading instruction are phonemic awareness synthetic phonics, reading fluency, language building and repeated opportunities for practice (‘Report of the National Reading Panel: Teaching Children to Read’, 2000). Extensive research has shown that an effective reading program would reflect these elements in a more targeted, intensive or focused way. Ideally, the reading intervention program would include (a) phonemic awareness and synthetic phonics to build decoding and word identification skills (e.g., Ehri, Nunes, Stahl, & Willows, 2001), (b) text reading; to build reading fluency and rapid recognition of written words (Coltheart, 2005; ‘Report of the National Reading Panel: Teaching Children to Read’, 2000) and (c) grammatical and semantic language building to assist with written text comprehension (Clarke, Snowling, Truelove, & Hulme, 2010; Lonigan et al., 2013; Reynolds et al., 2010; Vernon-Feagans et al., 2012). Repeated opportunities for practice in a variety of environmental contexts would serve to consolidate the skills being mastered in the reading intervention program. Reading intervention service providers (e.g., classroom teachers, specialist teachers, speech pathologists, etc.) would be highly trained in the phonological and linguistic structure of language, the continuum between spoken and written language, the progressive stages of how children learn to read and the factors associated with poor progression in reading. Importantly, service providers would be knowledgeable about how to teach low-progress readers to become competent and independent readers and they would adopt only well supported, evidence-based intervention approaches (Fielding-Barnsley & Purdie, 2005; Hempenstall, 2006; Washburn, Joshi, & Cantrell, 2011). Service providers would assume high expectations regarding reading outcomes for all low-progress readers, since exemplary reading intervention instruction characterised by the aforementioned elements has been shown to outweigh social gradient factors (e.g., Fried, Konza, & Mulcahy, 2012; Lonigan et al., 2013). A whole-school collaborative model would operate to ensure that strategies taught in the reading intervention were constantly and effortlessly reinforced by all staff (Crevola & Hill, 1998). Parents would feel able and welcome to share any concerns about their children’s reading progress with school personnel, knowing that any responses would be based on evidence but also sensitive and empathic (Serry, 2010).
If a reading difficulty was identified for a given child, intervention would start promptly and parents would be kept well informed with objective and transparent information about their child’s progress (or otherwise) during the intervention and how to support the child at home. Since there are a myriad of fee-paying private services (e.g., tutors, educational psychologists, speech pathologists, behavioural optometrists, chiropractors, perceptual-motor program facilitators), parents would also be adequately advised on the role and scope of external service providers. Importantly, parents would receive clear information on which interventions have more evidence and have less evidence to support their efficacy (e.g., ‘Learning Disabilities, Dyslexia, and Vision’, 2009; Pauli, 2007).
Further to theoretical and practical approaches to supporting low-progress readers, implementation models for intervention must also be considered with regards to efficiency and efficacy. A Response-to-Intervention (RtI) model is a multi-tiered, dynamic assessment and intervention system that is designed to provide increasingly specialised intervention according to a child’s response to the current treatment being provided (Buckingham et al., 2013; Fuchs & Fuchs, 2001). The structure of the RtI model is displayed in Figure 1. As can be seen, all children would receive tier-1 intervention. Steps for children identified as low-progress readers commence at tier-2 with small group-based intervention. While reading intervention has traditionally been provided individually (Buckingham et al., 2012; Pinnell, 1989), recent evidence has supported the efficacy of interventions delivered in small groups (e.g., Elbaum, Vaughn, Tejero Hughes, & Moody, 2000; Gersten et al., 2009; Lonigan et al., 2013), usually when children are first identified as at-risk readers. Group delivery has the advantage of greater economic and human resource efficiency. Importantly, group-based intervention reduces the chances of children missing out on intervention at crucial times, while progressively fewer children are expected to need the more specialist and more costly tier-3 intervention.
The Response-to-Intervention model.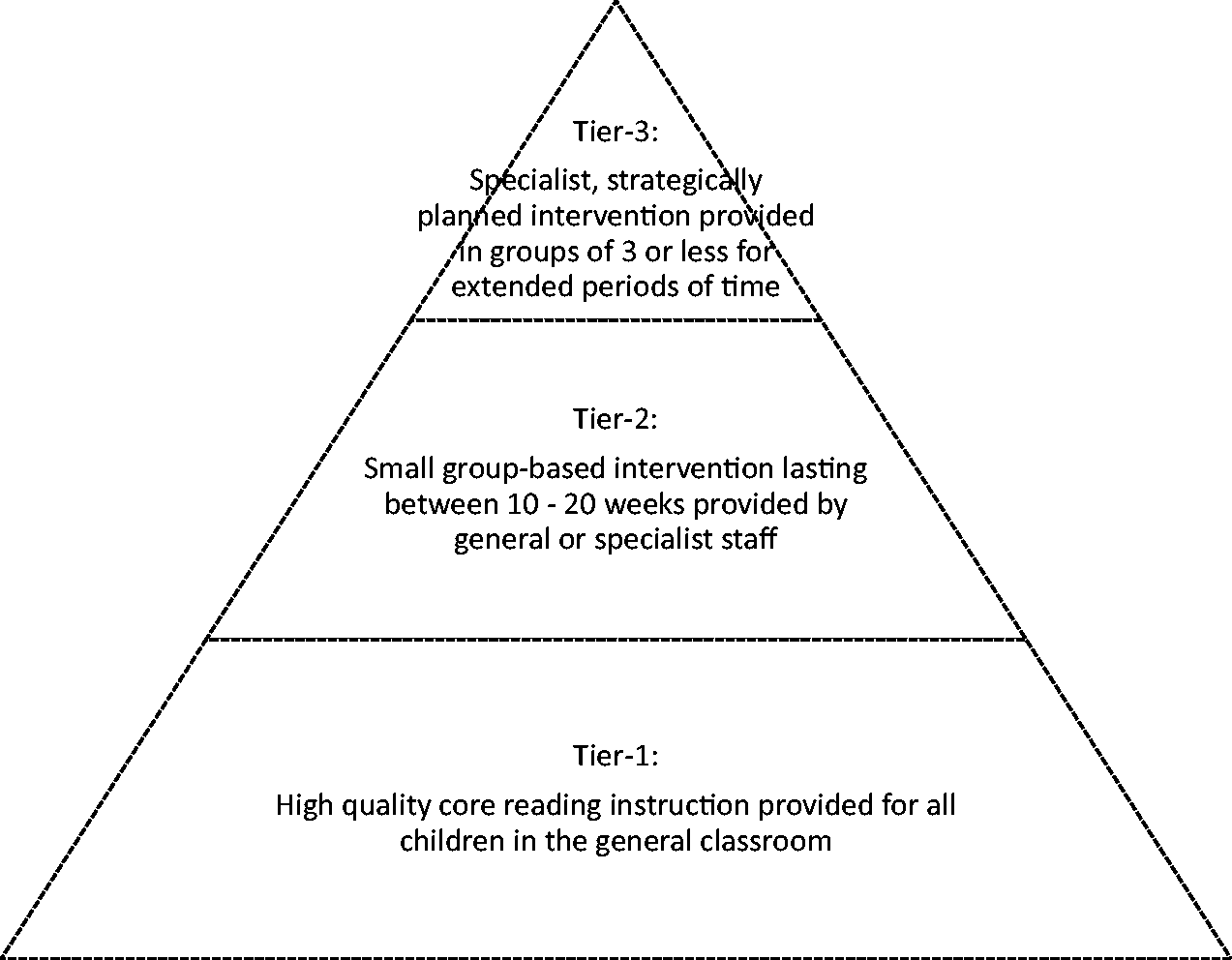
A number of recent studies have investigated differences between one-on-one and small group delivery of reading intervention (Elbaum et al., 2000; Iversen, Tunmer, & Chapman, 2005; Vaughn & Linan-Thompson, 2003). For example, Vaughn and Linan-Thompson (2003) compared the outcomes of daily supplementary reading intervention provided individually to that provided in groups of three and in groups of 10. No significant differences were apparent in reading outcome measures between children taught individually or in the small group. Importantly, children in both of these service delivery modes outperformed children taught in the larger group. Further, given the high cost of allocating resources for supplementary reading intervention, some studies have explored options for having alternative personnel such as community volunteers, student teachers and educational assistants trained to deliver the intervention (Brown, Morris, & Fields, 2005; Fitzgerald, 2001; Fried et al., 2012; Invernizzi, Juel, & Rosemary, 1997; Leal, Johanson, Toth, & Huang, 2004; Lonigan et al., 2013). Although not a controlled study, Fried et al. (2012) concluded that education assistants can be trained to successfully deliver an intensive, systematic and explicit reading intervention to low-progress readers. All studies stressed the importance of providing regular and ongoing support and guidance to those delivering the intervention.
The current situation in Australia
Many children are entering school without the prerequisite skills to support learning to read. Nevertheless, our discussion commences with the focus on processes occurring at school. Serry (2010) identified a base model of supplementary reading support (Figure 2) that was used in a sample of metropolitan Melbourne-based government primary schools in the State of Victoria. Although she found that certain schools adopted some additional reading intervention processes, typically after the second year of school, the base model was used consistently in all schools. In what follows, the RtI model (Figure 1) and the base model (Figure 2) will be used to compare an ideal and evidence-based approach with what appears to be the current situation in many Australian schools where Reading Recovery is the initial reading intervention offered.
The base model for reading intervention.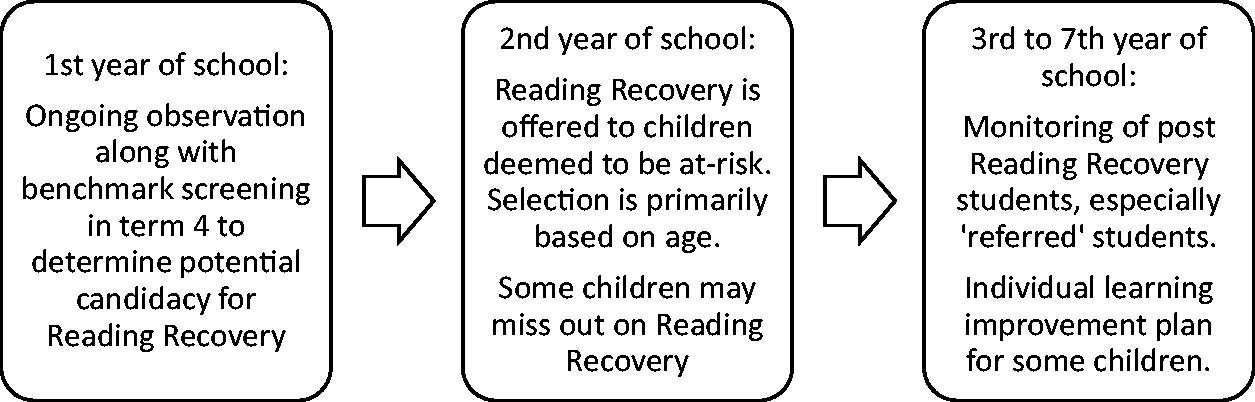
On entry to school, it appears that we cannot assume that all children, regardless of being at-risk readers or not, will receive high-quality, evidence-based, effective classroom reading instruction. Buckingham et al. (2013) summarised evidence indicating a high level of inconsistency in general reading instruction practices in Australian classrooms. Importantly, they note considerable variability in the teaching of phonics, despite the strong evidence base for systematic and explicit phonics instruction (or synthetic phonics). Further, Australian and international research finds that primary school teachers may not necessarily possess the requisite phonological, linguistic and metalinguistic knowledge in order to teach reading (e.g., Fielding-Barnsley & Purdie, 2005; Moats, 2009). Extensive phonological knowledge is necessary for anyone teaching children to read.11
This knowledge is especially critical for practitioners working with low-progress readers since phonological processing is likely to be vulnerable in these children (Moats, 2000). However, the federally funded Australian report titled ‘Prepared to Teach’ (Louden et al., 2005, p. 48, Table 4.3) revealed that among a surveyed group of 1300 novice teachers, 57% reported feeling inadequately prepared to teach phonics and only 54% reported feeling prepared to teach students with literacy learning difficulties (Louden et al., 2005, p. 52, Table 4.11). For at-risk readers, whether due to biological and/or environmental influences, exposure to less than ideal classroom reading instruction increases the likelihood of these children failing to read even before commencing supplementary reading intervention.
Comparison of Reading Recovery with an ideal reading intervention.
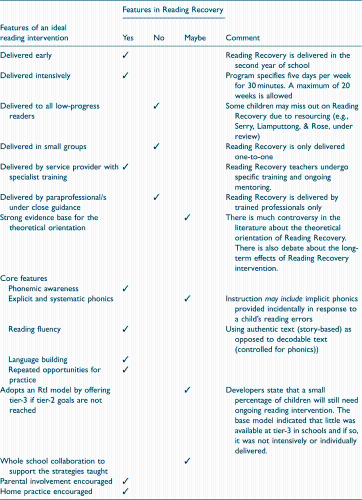
Reading Recovery fulfils ideals such as early and intensive implementation, and adopts three of the five core elements of an ideal reading program (reading fluency, language building and repeated opportunities for practice). However, in the Reading Recovery program, a number of the core elements are missing, and this places the vulnerable reader at even greater risk of ongoing reading difficulty. The theoretical orientation of Reading Recovery is inconsistent with the explicit and systematic teaching of phonics, which in turn also limits the amount of formal phonemic awareness instruction that can occur. A significant proportion of low-progress readers, particularly as beginning readers, need a more intensive and highly structured intervention compared to their typically reading peers in order to master the alphabetic code; explicit and systematic teaching of phonics has been shown to be the most effective way to do so (Buckingham et al., 2013; Lonigan et al., 2013). Moreover, Lonigan et al. demonstrated that low-progress readers need instruction in all areas of weakness and emphasised that instruction across ‘multiple domains’ was essential (2013, p. 126).
It is of particular concern that some children may miss out completely on accessing Reading Recovery simply due to resourcing constraints (Serry, Rose, & Liamputtong, 2014). Although we argue that Reading Recovery does not meet all the requirements of an ideal tier-2 reading intervention, the opportunity to engage in focused reading support is still likely to be of some benefit. Without any formal intervention, or intervention that starts late in the second year of school, children face even greater challenges as the gap between their own reading performance and that of their peers continues to widen, potentially alongside a host of other negative psychosocial consequences. To address resource issues, consideration could be given to small-group based intervention (Vaughn & Linan-Thompson, 2003) or the coexistence of a consultative model of practice whereby trained reading intervention specialists could guide and mentor many paraprofessionals to deliver high-quality reading intervention effectively. A consultative model could also extend to training for classroom teachers at tier-2, which would result in less disruption to the child or children concerned.
As the RtI model illustrates, tier-2 intervention allows for scope in regards to whom and how the intervention is delivered. The base model, however, adopts a specialist-driven withdrawal model that generally appears to be conducted in relative isolation from the broader school community. School-based speech pathologists, who, by definition, are highly trained in the phonological properties of language, are well placed to contribute to tier-2 intervention. However, resourcing constraints, combined with a lack of transparency about speech pathologists’ potential role on the reading support team compared with working in the domain of verbal communication, present significant obstacles to an effective intervention. In a qualitative investigation, Serry (2013) identified many more barriers than facilitators to Victorian school-based speech pathologists having a role with low-progress readers. These barriers included speech pathologists feeling too busy with their current caseload, having little time per week at a given school which impedes the feasibility of engaging in reading intervention and experiencing resistance from educational colleagues about their potential role with low-progress readers. Despite Australian and international position statements (e.g., American Speech-Language-Hearing Association, 2007; Scope of Practice for Speech-Language Pathology, 2008; Scope of Practice in Speech Pathology – Speech Pathology Australia, 2003) endorsing the role for speech pathologists to assess and treat written language impairments, this process does not appear to be reliably enacted across many schools.
Taken together, the system in place to support low-progress readers in many schools lacks both a robust scientific base and efficiency in its delivery of reading intervention, a situation further compounded by being insufficiently resourced. The base model does not have a formal tier-3 component as defined in the RtI model. Serry (2010) found that some schools provided options such as an individual educational plan or literacy groups for children who continued to struggle with reading, but this was not consistent practice. She found no evidence of the recommended tier-3 protocol which advocates for highly specialised and individually focused, evidence-based intervention. Reading Recovery developers acknowledge that some children will remain in need of further assistance once they have reached their 20-week allowance of sessions and should be referred for ongoing intervention (Clay, 1987; Lyons, 1989; Pinnell, 1989). Similarly, researchers who support a systematic approach to reading instruction and intervention also claim that between 2% and 6% of low-progress readers will be ‘treatment resisters’ and need further intervention. These views align with the tier-3 concept. In practice, however, a standard tier-3 component is not built into the structure of reading intervention across schools. Although it is likely that certain schools offer excellent or even just adequate support beyond the tier-2 phase, it is unacceptable that luck determines whether the child is at one of those schools.
Children who struggle with learning to read and who receive minimal, poorly focused or no ongoing reading support tend to become highly vulnerable for school disengagement and a range of comorbidities, especially across health, behavioural and psychosocial domains (e.g., Morgan, Fuchs, et al., 2008). It is hardly surprising that paediatricians in Australia often receive referrals for diagnosis and management of children with learning disorders and school problems (Hiscock et al., 2011; Roberts et al., 2012)
How we can achieve a best practice model for reading intervention
We argue that a best practice model to support low-progress readers adopts two key strategies. First, we advocate for an RtI model as a framework for reading intervention to ensure the use of evidence-based methods and optimal efficiency of the service delivery. This is likely to require an increase in primary school funding for more dedicated and well-trained specialists (speech pathologists, specialist literacy consultants, etc.) to work directly or indirectly towards the provision of evidence-based, early reading intervention. Second, many teachers lack the training and expertise to be able to identify and manage common developmental and behavioural conditions in the classroom that impact on learning (O’Keeffe & McDowell, 2004; Oberklaid, 2004). We maintain that tertiary preservice institutions need to review the content of their teacher training courses to ensure that they equip their graduates with knowledge about current best practice for supporting low-progress readers. Evidence suggests this is not the case at present (Fielding-Barnsley & Purdie, 2005; ‘Teaching Reading: Literature Review’, 2005). Further, to ensure that educators can generate their own professional life-long learning, we maintain that preservice teachers should be trained to critically appraise the evidence base for any instructional program or approaches they may use (see also ‘Focusing on the Learner’, 2013). Just as health and allied health professionals are held accountable for their use of scientifically validated evidence-based methods, we propose that teachers are trained to adopt the same approach.
Widespread access to high-quality and early reading intervention would have a host of positive short- and long-term outcomes for struggling readers, and very likely, for the broader school community. Using an RtI model, it would be expected that many low-progress readers would respond to the tier-2 phase of intervention. Given the clear evidence that there is just a small window of opportunity to provide intervention for optimal impact, there is no justification for children who are forced to wait for services or to miss out completely on receiving appropriate intervention. In turn, resources for the more intensive tier-3 intervention must be allocated for those children who have not responded sufficiently to the previous level of intervention.
We would also urge consideration of a consultative service delivery model, whereby skilled specialists can train and mentor teachers and classroom assistants to deliver high-quality reading intervention. The research would suggest that increased investment early in the developmental trajectory, before problems become entrenched and harder to remediate, makes sense from an economic point of view. A high-quality early intervention model reduces the range of comorbidities that are likely if children continue to fail in reading, and the long-term consequences of poor literacy are profound in terms of reduced life chances and poor outcomes in a range of domains (Deshler, 2005; DeWalt, Berkman, Sheridan, Lohr, & Pignone, 2004; Svetaz, Ireland, & Blum, 2000). The need to provide timely, appropriately focused and strategically delivered reading intervention is an issue that seems self-evident. The need is urgent, and the time is now – our children deserve nothing less.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.