
Abstract

Introduction
Dementia is the leading cause of death in Australia, with 425,000 Australians estimated living with dementia in 2024 (Australian Institute of Health and Welfare, 2025). The Australian Clinical Practice Guidelines and Principles of Care for People with Dementia (hereafter referred to as the Australian Clinical Guidelines) (2016) recommend a systematic approach to diagnosing dementia that includes a review of medical and family history, an assessment of cognitive and daily function and mental state, blood tests and structural neuroimaging. In practice, dementia is diagnosed in different settings, such as memory clinics, individual specialists, general practice, hospitals and aged care institutions, and the quality of dementia diagnostic care may vary across these settings (Ng and Ward, 2019). In this study, we reviewed clinical documents collected through the ASPirin in Reducing Events in the Elderly (ASPREE) trial to provide insights into the real-world diagnostic practices for dementia in Australia.
Methods
ASPREE was a primary prevention trial of low-dose aspirin among healthy community-dwelling people conducted in Australia and the United States (McNeil et al., 2018). In Australia, participants were aged 70 years and over, free of dementia at study entry and recruited through their general practitioners between 2010 and 2014. Participants were followed for a median of 4.7 years (interquartile range, 3.6–5.7 years) for the composite endpoint of the first occurrence of death, incident dementia or persistent physical disability (McNeil et al., 2018). Participants ‘triggered’ comprehensive dementia assessment if there was evidence suggesting incident dementia.
We conducted a review of the clinical documents of Australian participants with a dementia trigger for evidence of a clinician-confirmed diagnosis of dementia, and extracted data about (1) the diagnosing service/clinician (e.g. service setting, clinician specialty), (2) key aspects of the diagnostic process (e.g. completion of different investigations) and (3) initial management (e.g. prescription of AChEIs, referral to services). Descriptive statistics were used to report the characteristics of the sample and the diagnostic process. The ASPREE (Project number: CF07/3730-2006000745) and the current study (Project ID: 21397) received approval from the Monash University Human Research Ethics Committee.
Results
Of the 823 Australian ASPREE participants with a dementia trigger during the trial, we found evidence of a clinician-confirmed diagnosis of dementia in 282 participants (34%) (Supplementary Figure 1). Most of the participants were diagnosed in public memory clinics (n = 100, 36%), followed by private specialist clinics (n = 97, 34%) and other hospital outpatient clinics (n = 63, 22%). Across the three settings, those diagnosed in public memory clinics were most likely to be females and living alone, whereas those diagnosed in private specialist clinics were least likely to have less than 12 years of education, live in more disadvantaged areas and have hypertension or depression symptoms (Table 1).
Participant characteristics at the time of recruitment by dementia diagnosis setting.
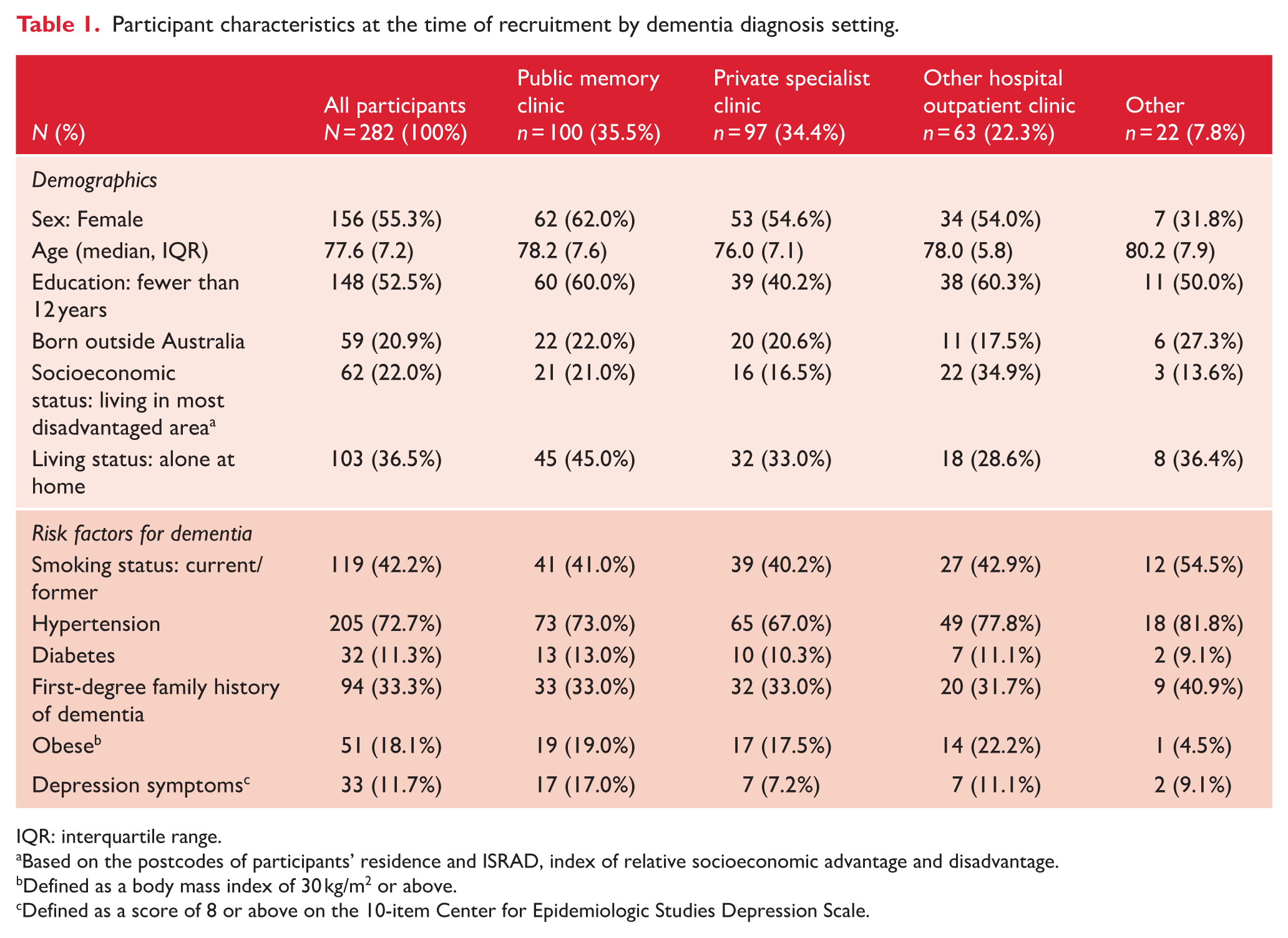
IQR: interquartile range.
Based on the postcodes of participants’ residence and ISRAD, index of relative socioeconomic advantage and disadvantage.
Defined as a body mass index of 30 kg/m2 or above.
Defined as a score of 8 or above on the 10-item Center for Epidemiologic Studies Depression Scale.
The median age at diagnosis was 81.0 years across the three settings (Table 2). Multidisciplinary diagnosing teams were involved in half of the diagnoses in public memory clinics (47%), but very rarely in other settings (under 3%). Geriatricians were the primary diagnosing clinicians (75%), with substantial involvement of neuropsychologists, psychiatrist/neuropsychiatrist and other clinicians (e.g. specialist nurses, allied health specialists) in public memory clinics, and significant involvement of neurologists/neuropsychologists in private specialist clinics. Multi-domain cognitive assessments were widely used (92%), with Mini-Mental State Examination being the most used tool (77%), followed by Montreal Cognitive Assessment (20%). Basic blood tests were completed in 58% of the participants, and brain imaging was undertaken in 75%, with computerised tomography being the most common modality (51%), followed by magnetic resonance imaging (32%). The dementia sub-type was recorded for most participants (95%), with Alzheimer’s disease (AD) being the most common sub-type (71%), followed by mixed Alzheimer’s and vascular dementia (hereafter referred to as mixed dementia) (15%). Dementia severity was documented in 39% of the participants, with the majority classified as mild (84%). Finally, 71% of the participants were recommended AChEIs and 29% were recommended relevant services.
Characteristics of diagnostic care by dementia diagnosis setting.

IQR: interquartile range; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; ACE: Addenbrooke’s cognitive examination; CT: computerised tomography; MRI: magnetic resonance imaging; PET: positron emission tomography; AChEI: acetylcholinesterase inhibitors.
Discussion
We reviewed the clinical documents of 282 ASPREE participants with a clinician-confirmed diagnosis of dementia to provide insights into the real-world diagnostic practices for dementia in Australia. We found that a dementia diagnosis was commonly made in public memory clinics, private specialist clinics and other hospital outpatient clinics. In addition, individuals diagnosed in private specialist clinics were generally younger, better educated and had fewer comorbidities, suggesting different socioeconomic and health status in the patient cohorts across dementia diagnosis settings. Geriatricians were the primary diagnosing clinicians, and a multidisciplinary team approach was used in half of the diagnoses in public memory clinics but very rarely in other settings.
A diagnosis of dementia requires a systematic approach that includes a review of medical and family history, an assessment of cognitive and daily function and mental state, basic blood tests and structural neuroimaging (Guideline Adaptation Committee, 2016). Our study found that most participants had cognitive testing and brain imaging completed (92% and 75%, respectively) as part of the diagnostic workup, but only 58% had basic blood tests completed. Across the three settings, participants diagnosed in public memory clinics were most likely to have these investigations completed. Overall, our results were consistent with those from the Australian Dementia Network (ADNeT) Registry, which is a clinical quality registry for people newly diagnosed with dementia (Lin et al., 2025). Interestingly, the completion rates for these investigations are higher in the ADNeT Registry (98% for cognitive test and 95% for both braining imaging and blood test), possibly because site participation in the ADNeT Registry is voluntary (Lin et al., 2025) and services that choose to participate may have more resources. The ADNeT Registry also commenced data collection from 2020, several years after the publication of the Australian Clinical Guidelines, reflecting overall improvements in clinical practice, education and knowledge. Finally, the ADNeT Registry collects data directly from diagnosing services, whereas the study used clinical documents gathered as part of the ASPREE trial and these documents might not include all information about the dementia diagnostic processes.
Regarding initial post-diagnostic care, the Australian Clinical Guidelines recommend AChEIs for managing symptoms of mild to moderately severe AD, and referral to, or provision of information on, appropriate services (Guideline Adaptation Committee, 2016). Our study found that over 70% of the participants were recommended AChEIs, whereas only 30% were recommended relevant services. The ADNeT Registry reported a 67% AChEI prescription rate for mild and moderate AD and a 61% referral rate to a dementia post-diagnostic programme (Lin et al., 2025). Together, these results suggest that increasing referral to relevant services is an area for continuous quality improvement for dementia diagnostic services in Australia.
We acknowledge limitations of our study. As noted above, clinical documents collected in the ASPREE trial might not include all information about the dementia diagnostic workup. Also, the ASPREE trial recommended the GPs to conduct a full clinical assessment for participants with a dementia trigger, and this might lead to higher uses of dementia diagnostic services than among the general population.
Despite these limitations, our study provides important insights into how dementia is diagnosed in Australia. It highlights substantial variability in the dementia diagnostic workup across different settings and identifies opportunities to enhance the quality of dementia diagnostic care, including the adoption of a multidisciplinary team approach and improving referral to relevant services following a dementia diagnosis.
Supplemental Material
sj-docx-1-anp-10.1177_00048674261431638 – Supplemental material for Differences in dementia diagnosis based on clinical setting: Data from the ASPREE clinical trial
Supplemental material, sj-docx-1-anp-10.1177_00048674261431638 for Differences in dementia diagnosis based on clinical setting: Data from the ASPREE clinical trial by Xiaoping Lin, Swarna Vishwanath, Jane Banaszak-Holl, Delphine Allan, Susannah Ahern, John J McNeil, Henry Brodaty, Robyn L Woods, Suzanne G Orchard and Stephanie A Ward in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We are most grateful to the ASPREE participants who volunteered for this clinical trial, the general practitioners and the medical clinics that supported the participants in the study. We also thank the dedicated and skilled ASPREE staff with specific acknowledgement to ASPREE Senior Project Manager Dr. Sharyn Fitzgerald and Senior Administration Manager Aaron Ham.
Author contributions
Xiaoping Lin: substantial contributions to design, analysis and interpretation of data, drafting the article and final approval of the version to be published.
Swarna Vishwanath: substantial contributions to design, acquisition, analysis and interpretation of data, drafting the article and final approval of the version to be published.
Jane Banaszak-Holl: substantial contributions to design, analysis and interpretation of data, drafting the article and final approval of the version to be published.
Delphine Allan: substantial contributions to design, acquisition and interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Susannah Ahern: substantial contributions to interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
John J. McNeil: substantial contributions to conception, acquisition and interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Henry Brodaty: substantial contributions to design, interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Robyn L. Woods: substantial contributions to acquisition and interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Suzanne G. Orchard: substantial contributions to acquisition and interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Stephanie A. Ward: substantial contributions to conception and design, interpretation of data, revising the article critically for important intellectual content, and final editing and approval of the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The ASPREE trial was supported by the National Institute on Aging and the National Cancer Institute at the NIH (U01AG029824), the National Health and Medical Research Council (NHMRC) of Australia (334047 and 1127060), Monash University and the Victorian Cancer Agency. This paper was prepared as part of the project entitled ‘A pilot dementia clinical Quality registry to improve dementia clinical care’, which was funded by the National Health and Medical Research Council (NHMRC) of Australia’s National Institute for Dementia Research (NNIDR) (Principal investigator: John J. McNeil, NHMRC APP 1140485). J.J.M. was supported through an NHMRC Leadership Fellowship (IG 1173690). The funding bodies had no role in the design, methods, subject recruitment, data collections, analysis and preparation of paper.
Ethical considerations
The ASPREE (Project number: CF07/3730-2006000745) and the current study (Project ID: 21397) received approval from the Monash University Human Research Ethics Committee. The ASPREE is a multicentre study and all sites received Institutions and Ethics Committee approvals under the governing site approval.
Consent to participate
All ASPREE participants provided written informed consent.
Consent for publication
Not applicable.
ORCID iDs
Data availability statement
Supplemental material
Supplemental material for this article is available online.