
Abstract
Objective:
Rates of suicide, suicidal ideation and self-harm are higher in regional and remote areas of Australia. This study aimed to examine the regional co-occurrence of adolescent suicidal ideation/self-harm and adverse childhood experiences, with consideration of area-based indices of socio-economic disadvantage and remoteness and the availability of mental healthcare professionals in New South Wales (NSW).
Methods:
Participants were 73,883 young people, born between 2002 and 2005, represented in the NSW Child Development Study (NSW-CDS) – a record-linkage study utilising Commonwealth and State government records. Aggregated longitudinal data according to statistical areas of residence were used to geographically map adolescent suicidal ideation/self-harm against prior adverse childhood experiences, socio-economic disadvantage, geographical remoteness and the number of mental healthcare professionals per region.
Results:
The average number of adverse childhood experiences and the proportion of children residing in areas of socio-economic disadvantage and geographical remoteness were strongly associated with the regional incidence of suicidal ideation/self-harm. Associations between the incidence of suicidal ideation/self-harm and the number of mental healthcare professionals in each region were not significant in adjusted models. Young people growing up in regions outside of Greater Sydney, particularly those in north-west NSW, had the greatest exposure to early adverse childhood experiences, the highest proportion residing in socio-economic disadvantaged and geographically remote areas and the highest incidence of adolescent suicidal ideation/self-harm.
Discussion:
These findings have policy implications for the geographic allocation of resources to prevent self-harm and suicide in young people. Early-life interventions should be aimed at reducing adverse childhood experiences.
Suicide rates vary across geographical locations, with the highest suicide rates in Australia observed in the most remote regions (Australian Institute of Health and Welfare, 2024e; Cheung et al., 2012). This corresponds with the regional distribution of suicidal ideation and self-harm, which have also been linked to the geographic distribution of socio-economic status and rates of mental illness (Australian Institute of Health and Welfare, 2024b, 2024d; Hielscher et al., 2022). The Young Minds Matter survey of Australians aged 12–17 years (Lawrence et al., 2015) demonstrated that rates of suicidal ideation/self-harm were generally higher in regions with elevated aggregate levels of socio-economic disadvantage and higher incidence of depressive and anxiety disorders (Hielscher et al., 2022).
According to socio-ecological frameworks of adversity, traditional adverse childhood experiences (ACEs) (e.g. abuse, neglect and household dysfunction) are recognised to occur within a broader socio-political context that makes ACEs more likely to persist in marginalised populations (Meléndez Guevara et al., 2024). These frameworks posit that ACEs increase risk for poor health and mental health outcomes (including suicidal ideation/self-harm) via their synergistic and deleterious impact on the stress-response systems of ACE-exposed individuals (Mehta et al., 2023; Niño et al., 2025; Nurius et al., 2016). Specific ACEs which have been linked to suicidal ideation/self-harm include child maltreatment and contact with the criminal justice system, in addition to familial factors such as parental death, mental illness, criminal offending and welfare recipience (Angelakis et al., 2019; Kisely et al., 2024; Thompson et al., 2019; Watkeys et al., 2024). To our knowledge, there has been no attempt to examine the relationship between the geographic distribution of these ACEs and rates of suicidal ideation/self-harm among Australia’s adolescent population. Such knowledge could inform the allocation of health and social service resources to both prevent and respond to community needs.
Youth with histories of ACEs and suicidal ideation/self-harm are at increased risk of attempting and dying by suicide, making it critical to deliver timely intervention to young people affected by ACEs (Duarte et al., 2020; Fernando et al., 2022; Leckning et al., 2023). However, individuals living in outer regional and remote areas, where suicidal ideation/self-harm is most prevalent, tend to access mental health services at a reduced rate relative to those in metropolitan and inner regional areas (Productivity Commission, 2020). Multiple barriers have been suggested to account for this trend, including the reduced availability of mental healthcare providers (Productivity Commission, 2020). Despite this, the association between regional availability of mental health professionals and rates of adolescent suicidal ideation/self-harm in Australia has yet to be investigated.
Geographic mapping of adolescent suicidal ideation/self-harm and ACEs in Australia has been limited to date. The only study to examine this topic (to our knowledge) was based on synthetic estimates derived from self-report data of 2967 young people included in the Young Minds Matter survey. That study examined only a limited range of risk factors for suicidal ideation/self-harm and may have failed to accurately capture the regional distribution of suicidal ideation/self-harm in regions of Australia lacking representation among survey respondents (Hielscher et al., 2022). Policy and planning for suicide prevention in Australia could be greatly enhanced by improving our understanding of the geographic relationship between childhood adversity, suicidal ideation/self-harm and the availability of mental health service providers. The current study aimed to address this gap by investigating the relationships between the regional incidence of adolescent suicidal ideation/self-harm in association with the geographic distribution of ACEs, number of mental health professionals, socio-economic disadvantage and geographical remoteness among ~73,000 children drawn from the New South Wales Child Development Study (NSW-CDS) (Green et al., 2024). This study further aimed to determine whether there were regional differences in the types of services responding to suicidal ideation/self-harm in the context of ACE exposure by examining suicidal ideation/self-harm as reported by health and non-health services separately, and in tandem.
Method
Participants
The 73,883 participants in this study were drawn from the NSW-CDS (Green et al., 2024). The NSW-CDS is a population cohort study of 91,957 children born between 2002 and 2005, for whom records of birth, child protection, criminal justice, education, welfare and health system contacts for the children and their parents were linked by the NSW Centre for Health Record Linkage (CheReL) and the Australian Institute of Health and Welfare (AIHW) Data Integration Service Centre. Record linkages were performed in December 2021, when participants were 18 years of age (mean = 18.24, SD = 0.37), with records available from birth (and prior for parent data). Children were excluded from the current analysis if they lacked linked data for either parent (n = 16,266), if they had a sibling in the cohort (n = 1313 – one sibling was retained at random) or if they were missing key demographic data (n = 135). Ethical approval was received from the NSW Population and Health Services and ACT Health Human Research Ethics Committees (HREC/18/CIPHS/49) and the AIHW Human Research Ethics Committee (EO2020/4/1026) under the ‘waiver of consent’ provision of the National Health Medical Research Council (NHMRC) National Statement of Ethical Conduct in Human Research (National Health and Medical Research Council, 2023).
Measures
Geographic location – Statistical Area 4
All measures were derived in relation to the young person’s Statistical Area 4 (SA4) area of residence, as described by the Australian Bureau of Statistics’ (ABS) Australian Geography Standard (Australian Bureau of Statistics, 2021b). Each participant’s SA4 of residence was drawn from the 2009 Australian Early Development Census (AEDC; a teacher-completed assessment of each child at school entry) (Brinkman et al., 2014) or from the 2015 Middle Childhood Survey (MCS; a self-report assessment conducted in Grade 6) (Laurens et al., 2017) for the 3.1% of children (n = 2265) who lacked an AEDC record.
Self-harm and suicidal ideation
Instances of self-harm and suicidal ideation among adolescents (⩾12 years of age) were identified in multiple record sets from health and other social services agencies. In brief, health contacts for suicidal ideation/intentional self-harm were identified via International Classification of Diseases 10th Edition – Australian Modification (ICD-10-AM) diagnostic codes for intentional self-harm (X60-X84, T14.91 and Y87.0) and suicidal ideation (R45.81) present in the NSW Ministry of Health and ACT Health Directorate’s Admitted Patient Data Collections (APDC, 2001–2021) or Emergency Department Data Collections (EDDC, 2005–2021) or the NSW Ministry of Health Mental Health Ambulatory Data Collection (MH-AMB, 2001–2020). Instances of non-health contact for suicidal ideation/self-harm, included child protection contacts recorded by the NSW Department of Communities and Justice ChildStory database (2000–2020) and records of police contact recorded by the NSW Police Force in their Computerised Operational Policing System (COPS, 2004–2020). Three indicators of suicidal ideation/self-harm contact were used in focal analyses, representing (1) any suicidal ideation/self-harm contact, (2) any health contact for suicidal ideation/self-harm and (3) any non-health contact for suicidal ideation/self-harm. These indicators were cross-referenced with the individual’s SA4 of residence to determine the number and percentage of young people in each SA4 region with each index of suicidal ideation/self-harm.
Number of ACEs
From a total of 17 ACE indicators, the average number of ACEs prior to 12 years of age (i.e. prior to the outcome observation period) was determined among young people residing in each SA4 region. The 17 ACE indicators were: (1) maternal mental disorder; (2) paternal mental disorder; (3) maternal means-tested welfare recipience; (4) paternal means-tested welfare recipience; (5) child criminal charges; (6) maternal criminal charges; (7) paternal criminal charges; (8) child criminal incarceration; (9) maternal criminal incarceration; (10) paternal criminal incarceration; (11) maternal death; (12) paternal death; (13) child protection contact; (14) child out-of-home care placement; (15) child police contact as a victim; (16) child police contact as a witness and (17) child police contact as a person of interest.
Indicators of maternal and paternal mental disorders were derived from health records (APDC, EDDC and MH-AMB) based on the presence of ICD-10-AM F-codes, or codes for suicidal ideation and self-harm (X60-X84, T14.91, Y87.0, R45.81). Parental means-tested welfare recipience – including welfare payments targeting financial hardship, for which individuals are subject to asset and income tests to assess eligibility (see Green et al., 2024) – was identified in the ‘Data Over Multiple Individual Occurrences’ (DOMINO, 2001–2018) dataset, from the Australian Commonwealth Department of Health and Welfare and Department of Social Services. Records of criminal offending or incarceration for the child, or their parents, were derived from the NSW Bureau of Crime Statistics and Reporting (BOCSAR, 1994–2022) Custody and Reoffending database. Parental death was determined from records in the NSW Registry of Births, Deaths, and Marriages (RBDM, 2000–2021). Records of child protection contact and out-of-home care placements were identified in the ChildStory database. Finally, the COPS database was utilised to derive indices of children’s contact with police as a victim, witness and person of interest, respectively.
Availability of mental health professionals
The numbers of full-time equivalent (FTE) psychiatrists, psychologists and mental health nurses per 100,000 residents in each SA4 region in 2021 were obtained from the AIHW (Australian Institute of Health and Welfare, 2021a).
Sociodemographic factors
Area-based measures of socio-economic status and geographical remoteness were derived from the AEDC in the first instance, or from the MCS where AEDC data were not available. Children were grouped into quintiles of socio-economic status measured by the Socio-Economic Index for Areas (SEIFA) Index of Relative Disadvantage (Australian Bureau of Statistics, 2011), ranging from 1 (most disadvantaged) to 5 (least disadvantaged). The proportion of children residing in the most disadvantaged SEIFA quintile was then derived for each SA4 region. Measurement of geographical remoteness was based on the Accessibility/Remoteness Index of Australia (ARIA) (Australian Bureau of Statistics, 2006), grouped into ‘Metropolitan’, ‘Inner regional’ and ‘Outer regional, remote, and very remote’ areas, with the percentage of children residing in the latter category derived for each SA4 region. Variations between outer regional, remote and very remote areas could not be investigated given limited numbers of children residing in such areas (particularly remote and very remote areas) within each SA4 region.
Statistical analysis
All analyses were performed in R v4.0. Geographic maps of SA4 regions in NSW were generated using the ozmaps (Summer et al., 2022), ozmaps.data (Summer, 2022), sf (Pebesma and Bivand, 2023), ggplot2 (Wickham, 2016) and plotly (Sievert, 2020) packages. Associations between regional incidence of self-harm/suicidal ideation, ACEs, mental health professionals, socio-economic disadvantage and geographical remoteness were assessed using bivariate correlation analyses. Univariate and multivariate linear regression analyses explored associations between the cumulative incidence of adolescent suicidal ideation/self-harm in each region and all other variables. Regions were excluded from analyses if they contained less than 15 children with a record for any particular variable under analysis. This was done to preserve the anonymity of research subjects and the reliability of statistical analyses.
Results
Regional distribution of variables
The average number of ACEs experienced by young people in NSW was highest in the North and North-Western regions of NSW, with elevated adversity also evident throughout all of NSW outside the Northern, Eastern and inner regions of metropolitan Sydney (Figure 1(a), Table 1 and online interactive figure). Similarly, the incidence of suicidal ideation/self-harm was highest in the North-Western regions of NSW and was lowest in the Greater Sydney area (including South-Western regions of Sydney) and the Riverina region in the state’s South-West (Figure 1(b)). There was a strong regional association between the average number of ACEs and incidence of suicidal ideation/self-harm (Figure 1(c)). Regions in the North, East, inner West and South of Sydney consistently had the lowest average ACEs (0.61 ⩽ 0.96) and incidence of suicidal ideation/self-harm (2.7 ⩽ 4.4%). The inner city, outer West and South-Western regions of Sydney had higher mean ACEs (1.41 ⩽ 1.96), with three of these regions also showing elevated rates of suicidal ideation/self-harm (Blacktown [5.6%], City and Inner South [5.5%] and Outer South West [6.25%]). Outside Greater Sydney, the regions showed consistently elevated average numbers of ACEs (1.58 ⩽ 2.41) and incidence of suicidal ideation/self-harm (4.9 ⩽ 10.8%). The regional distributions of suicidal ideation/self-harm as determined by health (Supplementary Figure 1A) or non-health (Supplementary Figure 1B) records were similar throughout NSW. Five regions across the North, East and centre of Sydney, in addition to Newcastle and Lake Macquarie, had a higher incidence of suicidal ideation/self-harm reported in health records (relative to non-health records), while the remaining regions of NSW had a higher incidence in non-health records.
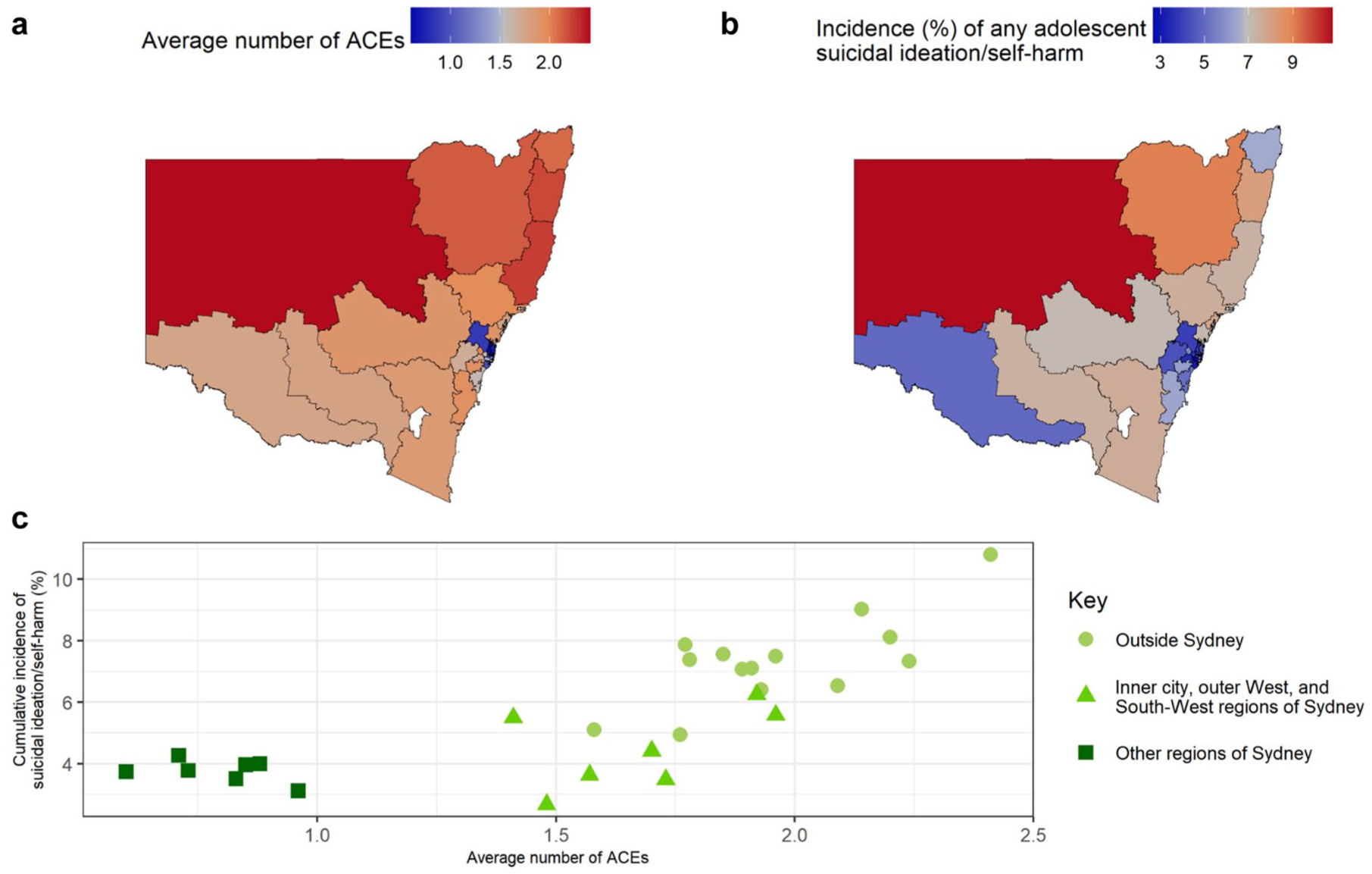
Maps of New South Wales (Statistical Area 4 regions) depicting (a) average number of adverse childhood experiences (ACEs) and (b) incidence of adolescent self-harm/suicidal ideation, in addition to (c) a scatterplot of the average ACEs and incidence of self-harm/suicidal ideation.
Descriptive statistics for Adverse Childhood Experiences and self-harm and suicidal ideation in each Statistical Area 4 (SA4) region of New South Wales.
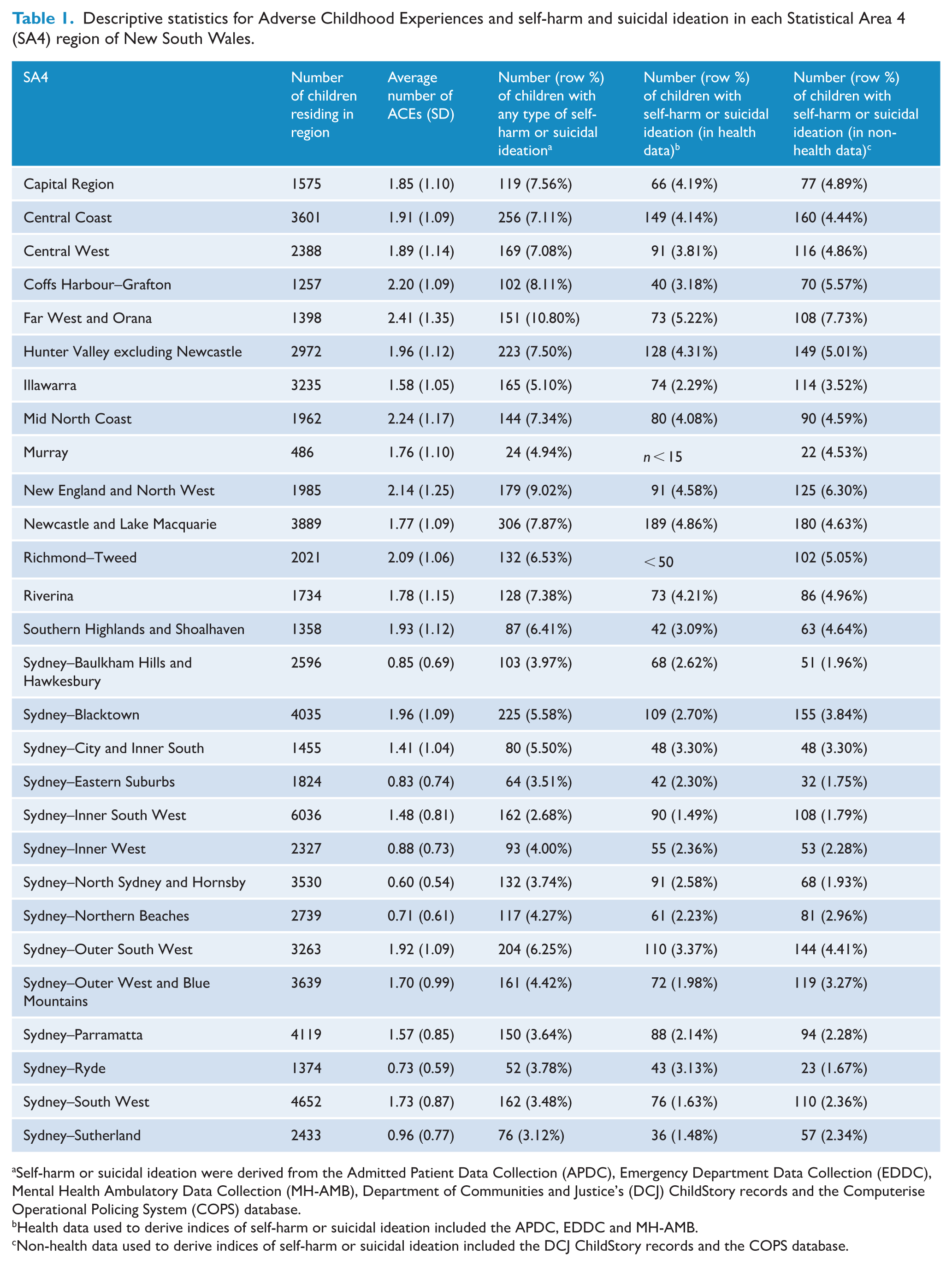
Self-harm or suicidal ideation were derived from the Admitted Patient Data Collection (APDC), Emergency Department Data Collection (EDDC), Mental Health Ambulatory Data Collection (MH-AMB), Department of Communities and Justice’s (DCJ) ChildStory records and the Computerise Operational Policing System (COPS) database.
Health data used to derive indices of self-harm or suicidal ideation included the APDC, EDDC and MH-AMB.
Non-health data used to derive indices of self-harm or suicidal ideation included the DCJ ChildStory records and the COPS database.
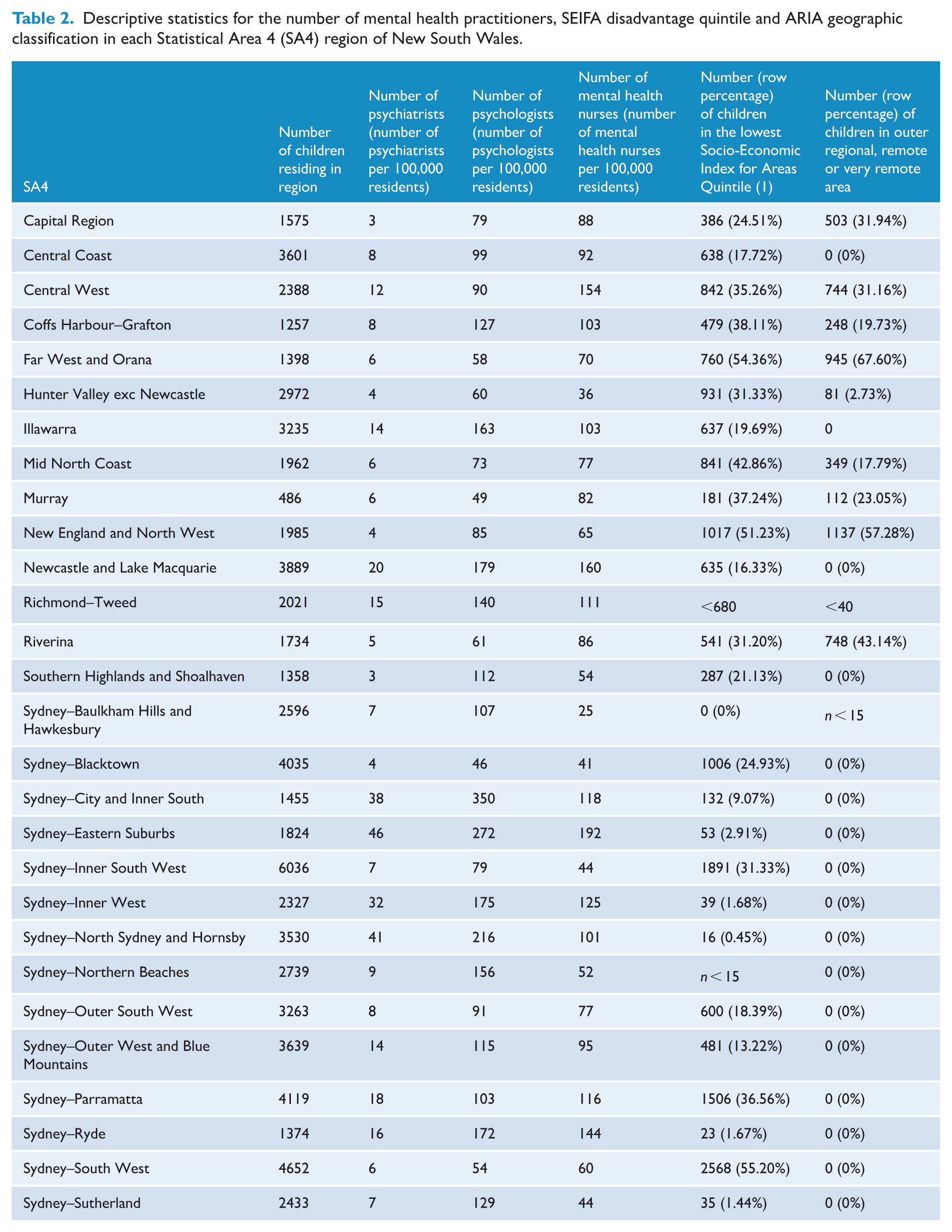
The numbers of FTE psychiatrists and psychologists (per 100,000 people) were heavily concentrated in four regions of Sydney (City and Inner South, Eastern Suburbs, Inner West [for psychiatrists only] and North Sydney and Hornsby) (Table 2). The number of mental health nurses was similarly high in particular regions of Sydney, including City and Inner South, Eastern Suburbs, Inner West, Paramatta and Ryde, with above-average numbers also in the Central West and Newcastle and Lake Macquarie regions of NSW. Bivariate associations between each of the variables described earlier are presented in Supplementary Figure 2.
Descriptive statistics for the number of mental health practitioners, SEIFA disadvantage quintile and ARIA geographic classification in each Statistical Area 4 (SA4) region of New South Wales.
Associations between suicidal ideation/self-harm and all other factors
Univariate and multivariate linear regression coefficients reflecting associations between the regional cumulative incidence of each type of suicidal ideation/self-harm and the average number of ACEs, numbers of mental health professionals, socio-economic disadvantage and geographic remoteness, are displayed in Table 3. A significant amount of the variance was explained by each multivariable model for the health (F[6,16] = 5.57, p = 0.003, Adjusted R2 = 0.555), non-health (F[6,17] = 39.03, p = 5.043×10−9, Adjusted R2 = 0.908) and the combined (F[6,17] = 20.20, p = 7.264×10−7, Adjusted R2 = 0.834) indices of suicidal ideation/self-harm. The average number of ACEs and the proportion of children residing in outer regional, remote and very remote areas were both significantly associated with the cumulative incidence of all indices of suicidal ideation/self-harm in both univariate and multivariate models. The average number of ACEs were most strongly associated with the incidence of ‘any’ suicidal ideation/self-harm: Each unit increase in the average number of ACEs was associated with a 3.0% (4.3% adjusted) increase in the regional incidence of suicidal ideation/self-harm. Increased ACEs were associated with the greatest increase in the non-health (2.5% unadjusted, 3.2% adjusted), relative to the health (1.2% unadjusted, 1.8% adjusted), index of suicidal ideation/self-harm incidence.
Univariate and multivariate regression coefficients examining the associations between self-harm/suicidal ideation and adverse childhood experiences (ACEs), sociodemographic risk factors and number of mental health practitioners in each Statistical Area 4 (SA4) region of New South Wales.
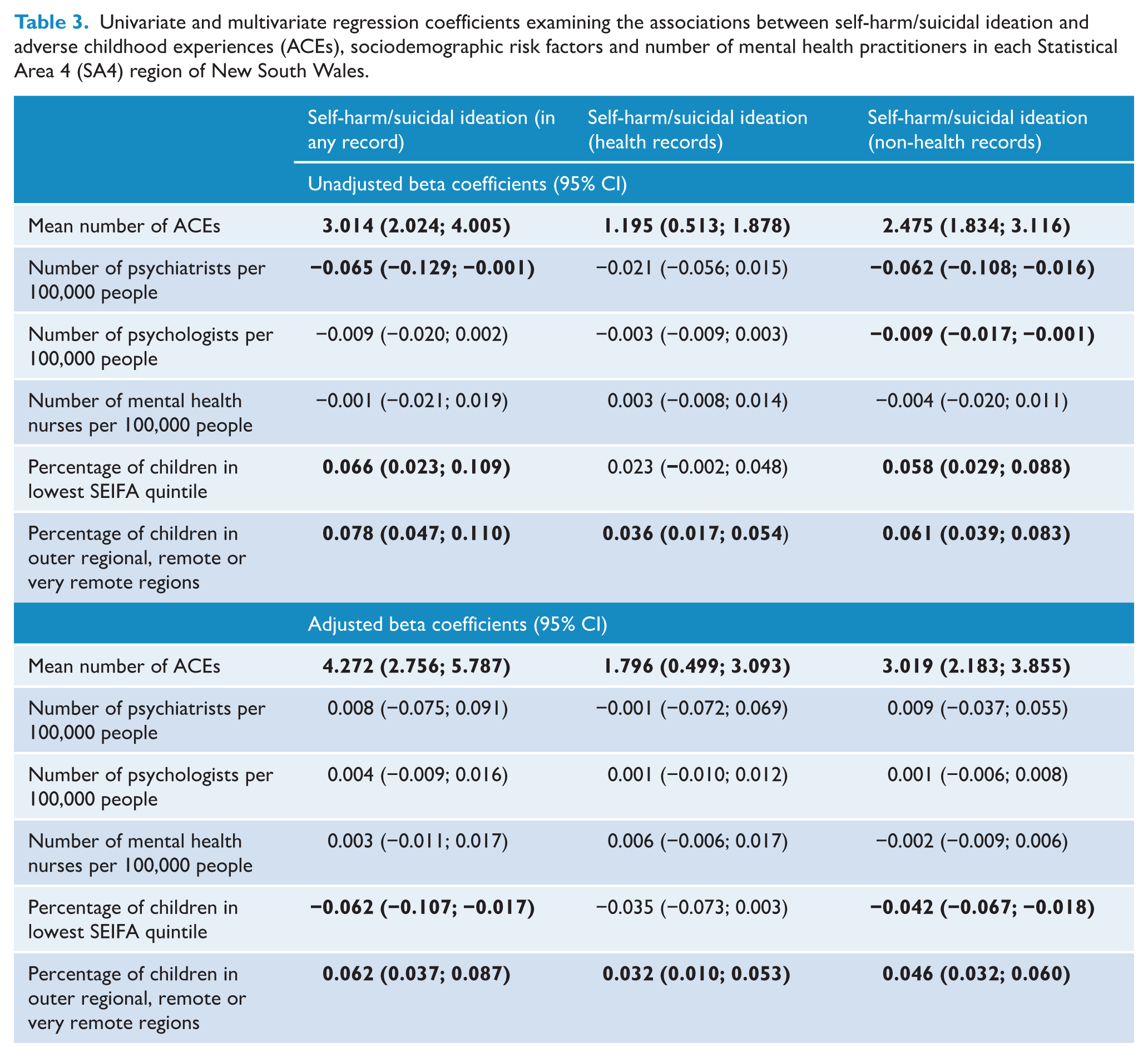
Each percentage increase in the proportion of children residing in outer regional, remote and very remote regions was associated with a 0.08% (0.06% adjusted) increase in the incidence of suicidal ideation/self-harm. Similarly, each percentage increase in the proportion of children in the most disadvantaged SEIFA quintile in each region was associated with a 0.07% increase (0.06% decrease in adjusted models) in the incidence of suicidal ideation/self-harm in univariate models. Similar effects were observed between health and non-health indicators of suicidal ideation/self-harm in association with geographical remoteness. However, socio-economic disadvantage was associated only with the non-health indicator of suicidal ideation/self-harm incidence.
The regional availability of psychiatrists was associated with a 0.07% reduction in the regional incidence of any suicidal ideation/self-harm in the unadjusted but not the adjusted model. Both the regional availability of psychiatrists (
Discussion
The incidence of suicidal ideation and self-harm in adolescence was significantly higher in regions of NSW where children had been exposed to a greater number of ACEs, and where there was greater socio-economic disadvantage and geographic remoteness. Regions in the North, East, Inner West and South of Sydney had consistently low numbers of ACEs, suicidal ideation/self-harm incidence, socio-economic disadvantage and geographical remoteness; regions in the inner city, outer West and South-West of Sydney had consistently elevated ACEs with some regions also demonstrating elevated suicidal ideation/self-harm incidence and/or socio-economic disadvantage. Finally, regions outside Sydney typically had the highest ACEs, suicidal ideation/self-harm incidence and proportions of children residing in areas of socio-economic disadvantage and geographic remoteness. In contrast, the availability of mental health professionals was not significantly associated with the regional incidence of suicidal ideation/self-harm.
These findings extend prior research that has demonstrated strong associations between ACEs and suicidal ideation/self-harm at an individual level (Cheung et al., 2012). The current findings further suggest that the variance in the regional incidence of suicidal ideation/self-harm (especially that recorded by child protection and police services) can largely be explained by the average number of ACEs, proportions of children residing in areas of socio-economic disadvantage and geographical remoteness and number of mental healthcare professionals in each region. These findings could be leveraged by policymakers to guide the regional allocation of resources to address adolescent suicidal ideation/self-harm. Furthermore, while not implying causation, the strength of the associations between the regional extent of ACE exposure and incidence of adolescent suicidal ideation/self-harm adds further weight to calls for reducing/eliminating ACEs as a means of preventing suicide and multiple other health conditions linked to ACE exposure (Hughes et al., 2017). There are a variety of evidence-based strategies policymakers could implement to prevent ACEs (Matjasko et al., 2022), including increasing the financial security of families; changing social norms around violence towards children through public awareness campaigns and legislation banning corporal punishment; providing early intervention programmes such as positive parenting and social-emotional skills training; increasing the accessibility of mentoring and after-school programmes and ensuring that ACE-exposed victims receive adequate mental health treatment (Centers for Disease Control and Prevention, 2019).
The regional incidence of suicidal ideation/self-harm found in the current study was broadly consistent with prior studies (Australian Institute of Health and Welfare, 2024a, 2024b; Hielscher et al., 2022). However, the current study reported a higher incidence of adolescent suicidal ideation/self-harm in the Far West and Orana region compared to prior studies, while relatively lower incidence was evident in the Murray region and Southern/Western regions of Sydney (despite still reflecting the highest incidence within Sydney in the current study). Methodological differences between studies, including the different data acquisition methods and the timescale of the outcome assessment period may account for these discrepancies. Prior survey-based estimates of suicidal ideation/self-harm may have been subject to selection/response bias, while the current study likely underestimated the true extent of adolescent suicidal ideation/self-harm as affected children do not always receive treatment or become the subject of child protection or police reports (Fitzpatrick et al., 2021). Nevertheless, the findings of the current study align more closely with the geographic distribution of the age-standardised suicide rate reported by the AIHW (Australian Institute of Health and Welfare, 2024c) than those from the survey-based estimates of adolescent suicidal ideation/self-harm. The synergy of findings from the current and prior studies suggest that the highest incidence of adolescent suicidal ideation and self-harm (in NSW) is in the North-West and Far West of the state, and in the Western and South-Western regions of Sydney. However all regions outside of Sydney (apart from Murray) demonstrated elevated incidence of suicidal ideation/self-harm.
Interestingly some regions in the Inner city, outer West and South-Western regions of Sydney demonstrated a reduced incidence of suicidal ideation/self-harm relative to regions outside of Greater Sydney with similar numbers of average ACEs. It may be that the high proportion of culturally and linguistically diverse families in these regions face greater obstacles in accessing mental healthcare (Australian Bureau of Statistics, 2021a; Wohler and Dantas, 2017), resulting in a lower proportion of service use among children experiencing suicidal ideation/self-harm in these regions. Despite findings which suggest that residence in metropolitan relative to regional/remote areas has been associated with increased resilience and reduced psychological distress (Australian Institute of Health and Welfare, 2021b; Lykins et al., 2024), both regional and urban environments vary considerably in terms of their levels of affluence, amount of green space, infrastructure and services and population characteristics (Cortina and Hardin, 2023; Gong et al., 2016). Further research of these factors is needed in the context of ACEs and suicidal ideation/self-harm.
The results of this study also replicate previous reports of associations between the regional incidence of self-reported suicidal ideation/self-harm in adolescence and lower socio-economic status (Australian Institute of Health and Welfare, 2024a, 2024b; Hielscher et al., 2022). Interestingly, however, increased socio-economic disadvantage was associated with decreased incidence of suicidal ideation/self-harm in adjusted models (for combined and non-health incidences). This suggests that when holding constant the average number of ACEs, proportion of children in geographically remote areas and number of mental health professionals, children in regions with greater socio-economic disadvantage were less likely to be reported to child protection and police services for issues related to suicidal ideation/self-harm. This may be partially explained by fewer mandatory reporters (e.g. allied health professionals) and child protection caseworkers in socio-economically disadvantaged areas (NSW Health, 2021; NSW Ombudsman, 2014), decreased mental health literacy among socio-economically disadvantaged populations (Wu et al., 2024) leading to reduced reporting of children displaying signs of suicidal ideation/self-harm in such regions and/or wage and cost of living disparities between metropolitan and remote areas (Baker et al., 2016). It should be noted that while inequalities in the regional distribution of child protection caseworkers have substantially diminished in NSW over the past decade (NSW Department of Communities and Justice, 2024), the inequalities reported in 2014 correspond to the period during which the child protection records for the current study were ascertained.
However, the regional (per capita) availability of mental health professionals (including psychiatrists, psychologists and mental health nurses) was not associated with the cumulative incidence of suicidal ideation/self-harm throughout NSW after adjusting for other factors. This suggests that unadjusted associations may have been confounded by other factors such as socio-economic status. Alternatively, the lack of significant associations may be partially attributable to the provision of mental healthcare via telehealth, which eliminates distance-based barriers to accessing mental healthcare (Kavanagh et al., 2022; Thorn and Olley, 2023). Regardless of these issues, the present findings suggest that efforts to address regional disparities in the incidence of suicidal ideation/self-harm will likely need to address systemic factors promulgating ACE exposure to be effective, in addition to improving the accessibility of mental health professionals in regional areas.
Several limitations must be considered when interpreting these findings. First, rates of suicidal ideation/self-harm may have been underestimated given the omission of ICD-10-AM codes corresponding to poisoning via some pain and psychotropic medications. However, inclusion of such codes may have overestimated suicidal ideation/self-harm as such codes are not necessarily indicative of intentional self-harm. Second, this study was unable to account for the movement of children between regions over time, relying instead on cross-sectional assessments to determine their location of residence at school entry (or in middle childhood). Third, the examination of broad (SA4) geographic regions limits the extent to which the current findings can be used to guide resource allocation to specific communities in need. However, this analytic strategy was necessary to preserve the anonymity of subjects and the statistical reliability of estimates, given the limited number of children residing in some regional/remote areas. Fourth, we did not directly account for whether children died during the study period. Suicide deaths were recorded among the suicidal ideation/self-harm outcome variables, but not disaggregated due to the limited number of suicide deaths among children in the cohort at the time of record linkage (n < 15). Furthermore, since only 0.1% of the child cohort died during the study period (Green et al., 2024), the extent to which child deaths would have influenced our findings is limited. Finally, children who moved outside NSW would have been lost to follow-up, potentially further underestimating the extent of suicidal ideation/self-harm in this population cohort. These limitations should be counterbalanced against the strengths of this study, including its sample size, integration of multiple record sets across diverse government sectors, reduced selection bias and longitudinal design.
To reduce regional disparities in the incidence of adolescent suicidal ideation/self-harm, policymakers should focus on addressing the systemic inequalities underpinning the disproportionate number of young people exposed to ACEs in regional and remote areas of NSW. Further research is required to establish the efficacy of ACE-prevention strategies in reducing subsequent self-harm and suicide outcomes in Australia. Nevertheless, international evidence has convincingly demonstrated the benefits of ACE-prevention strategies (Centers for Disease Control and Prevention, 2019). State-wide reduction of ACE exposure, in-line with the most affluent regions of Sydney, thus has the potential to substantially reduce the overall incidence of suicidal ideation and self-harm in NSW. Increased resources directed to regions where children experience more extensive exposure to ACEs may begin to help facilitate this change.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251369628 – Supplemental material for Geographic mapping of adverse childhood experiences and adolescent suicidal ideation/self-harm in New South Wales, Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674251369628 for Geographic mapping of adverse childhood experiences and adolescent suicidal ideation/self-harm in New South Wales, Australia by Oliver J Watkeys, Kristin R Laurens, Stacy Tzoumakis, Kimberlie Dean, Felicity Harris, Melissa Mei Yin Cheung, Vaughan J Carr and Melissa J Green in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; Australian Institute of Health and Welfare; Department of Social Services; NSW Bureau of Crime Statistics and Research; NSW Department of Justice and NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC is funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments and Agencies, or the NSW and Australian Government. Record linkage was performed by the Centre for Health Record Linkage (http://www.cherel.org.au) and the Australian Institute of Health and Welfare (AIHW) Data Integration Service Centre (![]() ). We acknowledge the contribution of members of the NSW Child Development Study Lived Experience Network to this work.
). We acknowledge the contribution of members of the NSW Child Development Study Lived Experience Network to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055), an Australian Research Council (ARC) Discovery Project (DP230101990), a Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (APP2006436) and a Postdoctoral Fellowship from Suicide Prevention Australia (awarded to OW) funded by the Australian Government Department of Health, Disability and Ageing. Funding bodies had no role in the design, collection, analysis, interpretation, writing or decision to submit this manuscript for publication.
Data Availability Statement
Data used in this project has been provided by government or other agencies for the research purposes of the NSW Child Development Study and is unable to be shared with third parties or deposited into data repositories. Data can be accessed by applications to relevant data custodians.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.