
Abstract
Background:
The Growth and Empowerment Measure was developed by and for Aboriginal and Torres Strait Islander adults to measure social and emotional well-being and empowerment. This study aimed to co-design and validate a version of the Growth and Empowerment Measure with Aboriginal and Torres Strait Islander young people experiencing youth detention.
Method:
103 Aboriginal and Torres Strait Islander young people experiencing youth detention participated. Participants directed seven adaptations from the Growth and Empowerment Measure for adults to create a Growth and Empowerment Measure-Youth (GEM-Youth). 78 participants completed the GEM-Youth version 7 and 57 participants completed both the full GEM-Youth version 7 and the Kessler psychological distress scale (K10). Cronbach’s alpha and inter-item correlations were calculated for two components of the GEM-Youth: how I feel about myself and thinking about my everyday life. Associations between K10 and GEM-Youth scores were quantified using Pearson’s correlation.
Results:
How I feel about myself questions had a mean inter-item correlation of (0.21) and good internal consistency (α = 0.80). Thinking about my everyday life questions had a mean inter-item correlation of 0.18 and internal consistency of α = 0.69. How I feel about myself showed a strong negative correlation (r(55) = –0.61, [95% confidence interval: –0.42, –0.75] p < 0.001) with K10. Thinking about my everyday life showed a moderate negative correlation with K10 (–0.31, [95% confidence interval: −0.05, −0.52] p = 0.02).
Implications:
The GEM-Youth provides a culturally grounded and validated measure to assess social and emotional well-being and empowerment for Aboriginal and Torres Strait Islander young people in detention settings. This measure has therapeutic and research value that should be further refined and explored. Future research should adapt and validate this tool for use with other groups and settings.
Keywords
Background
Aboriginal and Torres Strait Islander people’s social and emotional and well-being
Aboriginal and Torres Strait Islander people are the oldest living cultures, having connections to the lands now known as Australia for over 60,000 years. Social and emotional well-being and resilience of Aboriginal and Torres Strait Islander people is related to cultural strengths including connection to country, family, community, mind, body and spirit, acknowledging historical political and social determinants (Dudgeon et al., 2017). Historic and ongoing experiences of colonisation and legislated assimilation practices have enforced removal of Aboriginal and Torres Strait Islander people from their homelands, kin and culture, impacting on social and emotional well-being. These impacts are compounded by health systems and services that prioritise the perspectives, experiences and needs of the Eurocentric majority (Gatwiri et al., 2021). Health research and practice has historically colonised the experiences of Aboriginal and Torres Strait Islander people, using methods, measures and interventions that fail to appropriately identify and acknowledge communities’ priorities and needs, perpetuating deficit discourses and racist and discriminatory practices (Sherwood, 2013). Aboriginal and Torres Strait Islander people consequently experience disproportionately poorer health and well-being outcomes; unmet social and emotional well-being needs; poorer socioeconomic, education and housing status; and overrepresentation in the criminal justice system (Hamilton et al., 2020).
Overrepresentation of Aboriginal and Torres Strait Islander young people in detention
Reducing the numbers of Aboriginal and Torres Strait Islander young people in contact with the criminal justice system is a key priority. Aboriginal and Torres Strait Islander young people experience detention at higher rates and at younger ages than non-Indigenous young people (Australian Institute of Health and Welfare (AIHW), 2023, 2024). While only 1% of Aboriginal and Torres Strait Islander young people will be subject to a supervision order on any given day, and despite comprising 5.7% of the general population, they currently represent over half of young people in youth detention (AIHW, 2023, 2024). These young people have considerable mental health and social and emotional well-being needs requiring tailored, culturally capable supports (Meurk et al., 2019).
IMHIP-Youth project
To address these needs, the Indigenous Mental Health Intervention Project for Young People (IMHIP-Youth) was developed to support the social and emotional well-being of Aboriginal and Torres Strait Islander young people experiencing youth detention in south-east Queensland. The goal of the project is to assist young people to return to community with improved social and emotional well-being and reduce the risks of re-incarceration. The IMHIP-Youth project has followed a co-design process through leadership of the Cultural Governance Group and continuous community involvement of Aboriginal and Torres Strait Islander young people experiencing detention, their families, carers, Elders and communities and other stakeholders (Dale et al., 2023). Part of this project has included the development and validation of a culturally informed measure of growth and empowerment.
Growth and Empowerment Measure
Valid and reliable research and therapeutic outcomes measures are essential tools for health services and individual providers to measure the effectiveness of services delivered. Due to a lack of culturally appropriate, strengths based measures, the IMHIP-Youth team aimed to co-design and validate a version of a measure accessible for young people experiencing detention for use therapeutically and to evaluate the IMHIP-Youth project intervention (Westerman and Dear, 2023). The approach taken was to adapt the Growth and Empowerment Measure (GEM), originally developed by and for Aboriginal and Torres Strait Islander adults (Haswell et al., 2010), for a youth population. The GEM measures individuals’ perspectives of their psychosocial well-being and empowerment at individual, family, organisational and structural levels. The GEM is based on western empowerment theory, holism in health care, issues of particular significance in the everyday life for Aboriginal and Torres Strait Islander communities such as grief, loss and stress and culturally relevant action to heal from the past and gain control over present (Haswell et al., 2010; Le Grande et al., 2017).
The GEM consists of two main psychometric scales designed to measure different aspects of social and emotional well-being: (1) ‘how I feel about myself’ (HIFAM), a 14-item Emotional Empowerment Scale with answers on a five-point scale and (2) ‘thinking about my everyday life’ (TAMEL) featuring 12 scenarios measuring functional aspects of empowerment on a seven-point scale. The original factor analysis of these scales found that the HIFAM related to two underlying constructs, described as ‘inner peace’ and ‘self-capacity’ while the TAMEL scenarios also related to two components described as ‘healing and enabling growth’ and ‘connection and purpose’ (Haswell et al., 2010). These two scales are accompanied by ‘getting to know you’ (GTKY) questions which includes questions to elicit demographic information, including culturally relevant information (Haswell et al., 2010).
Since its initial development and validation, the GEM has been identified as a high quality measure internationally and been widely used in several settings, including in services delivered to Aboriginal and Torres Strait Islander adults in custody (Campbell et al., 2021).
Methods
Stage 1: co-design of GEM-Youth
Participants
Co-design occurred with 103 Aboriginal and Torres Strait Islander young people experiencing detention at Brisbane Youth Detention Centre or West Moreton Youth Detention Centre between 2021 and 2023. Participants were aged between 12.5 years and 18 years, with a mean age of 15 years and 9 months. The majority of participants (n = 82, 80%) were male.
Recruitment and consent
A detailed description of the recruitment and consent process is provided in the study protocol (Dale et al., 2023). The minimum legal requirement for consent among these young people was signed written consent by the in-custody guardian. This was determined to be insufficient from a cultural perspective and inconsistent with the principle of respect (National Health and Medical Research Council (NHMRC), 2018). Therefore, the researcher (RHF) additionally sought signed written consent from young people and, where possible, attempted to contact the young person’s parent or primary caregiver in the community to explain the project and invite them to raise any questions or concerns they might have. A set of information cards was developed in collaboration among the research team, IMHIP-Youth Cultural Governance Group, and with assistance from a qualified speech therapist to explain the study to young people in a clear and accessible way. The researcher (RHF) went through these cards verbally with young people prior to obtaining consent. Consistent with the principle of reciprocity (NHMRC, 2018), young people were remunerated with a $20 gift card. In addition, through her engagements with young people, RHF discovered that ‘crown tags’ (personalised crown symbols associated with graffiti) were popular. In recognition of this, RHF invited all young people with whom she engaged the opportunity to submit their crown tag to create a collage that she compiled and distributed back to them as a poster and appeared in the centrefold of a booklet entitled ‘Dreams and Visions’ that summarised the information young people had provided and was also distributed back to them. Where crown tags included, or appeared to include, identifying information (e.g. initials or postcodes), these were blurred so as not to be recognisable.
Procedure
An initial prototype of the GEM-Youth (version 1), closely resembling the GEM, was created by members of the IMHIP-Youth project, including Aboriginal and non-Aboriginal project chief investigators whose disciplines and experience included youth work, mental health, health and social science, psychology, psychiatry and social work. The GEM-Youth maintained the three part structure of the GEM (GTKY, HIFAM and TAMEL). All interviews and adaptations were undertaken by a Garigal and Walkaloa woman researcher (RHF).
In response to feedback, new versions were developed and tested iteratively through discussions with participants, critical reflections by the researcher and discussions among the IMHIP-Youth Cultural Governance Group. Through this process the researcher continued to develop rapport with the young people and gained greater insights into the measure’s relevance to them, order of questions, visual appeal and language. Most participants completed the GEM-Youth face-to-face with the researcher. Four interviews were completed via videocall due to COVID-19 pandemic restrictions, with a case worker present to support the participant. In a small number of instances participants were able to compare versions of the GEM-Youth they had completed with updated versions to provide ongoing feedback. Overall, the co-design process prior to validation resulted in seven adaptations of the GEM-Youth (Supplementary Material 1).
Stage 2: validation of GEM-Youth
Measures and procedure
GEM-Youth (version 7), HIFAM and TAMEL components, and K10 data collected from individuals completing interviews in Stage 1 were used to validate the GEM-Youth. Inter-item correlations and Cronbach’s alpha were calculated for 78 young people who completed some or all of the GEM-Youth v7. Comparison with the K10 was performed on data from 57 individuals for whom complete Gem-Youth v7 and K10 data were collected. These were a subset of the 103 young people who engaged in the co-design process.
Scoring GEM-Youth
Answers on the GEM-Youth were transferred into numerical scores by item. Numerical scores for HIFAM items ranged from 1 to 5 (1 = Never, 2 = Hardly ever, 3 = Sometimes, 4 = Mostly, 5 = Always) and numerical scores for TAMEL items ranged from 1 to 7 (varying answer possibilities, with 7 being the most positive and 1 being the most negative option). HIFAM questions 12 and 14 were inverted to align with the other HIFAM questions (i.e. ‘Always’ being the most positive and ‘Never’ being the most negative option). Total scores were calculated separately for HIFAM and TAMEL questions. For HIFAM and TAMEL, higher scores were interpreted as stronger empowerment, for the K10, higher scores indicate higher levels of psychological distress.
Analysis
Reliability and internal consistency of the GEM-Youth version 7 was measured by calculating Cronbach’s alpha and corresponding inter-item correlations for HIFAM, TAMEL and K10 questions. Scores obtained from the HIFAM and TAMEL and K10 were compared by computing Pearson’s correlations. It was hypothesised that there should be negative association between GEM-Youth and K10 scores (i.e. higher levels of reported growth and empowerment should be associated with lower levels of psychological distress).
To evaluate inter-item correlations, we followed Clark and Watson (2019) in seeking a mean inter-item correlation in the range of 0.15–0.5, with individual scores sitting close to the mean. Assessing the adequacy of inter-item correlations is contingent on the scope of the construct being examined. Broader constructs, such as contained in the GEM-Youth, might reasonably have inter-item correlations at the lower end of this range, while narrower constructs should be more highly correlated. Inter-item correlations that are too high can suggest shortcomings with a measure, such as repetitiveness, narrowness or lack of generalisability. Cronbach’s alpha was used to assess the internal consistency of constructs. Conventionally, an alpha score at or above 0.8 is considered an indication of good or excellent reliability. Pearson’s correlations were evaluated as <|0.3| = weak,|0.3–0.5| = moderate and >|0.5| strong (Cohen, 1988).
Results
Stage 1: co-design of GEM-Youth
Initial feedback and observations from young people completing version 1 of the GEM-Youth affirmed that its concepts were for an adult participant group, as originally intended, and did not always resonate with young people. Young people identified challenges with several concepts, such as empowerment and spirituality, as well as phrasing and terminology. Completing the GEM-Youth Version 1 was time consuming and fatiguing for many, with most requiring two interviews to complete the measure. None of the young people were able to independently read the GEM-Youth version 1. Additional limitations of the custodial setting such as noise, lockdowns, time pressures and perceived peer pressure were thought to impact on comprehension, cognitive load and feelings about completing the measure. The format of the answer boxes in HIFAM appeared to be confusing and some of the concepts relevant to adults and to general community populations did not appear to resonate with young people in a detention setting. Feedback from young people included ‘I haven’t been to school much. I can’t understand this’ and ‘This is hard’.
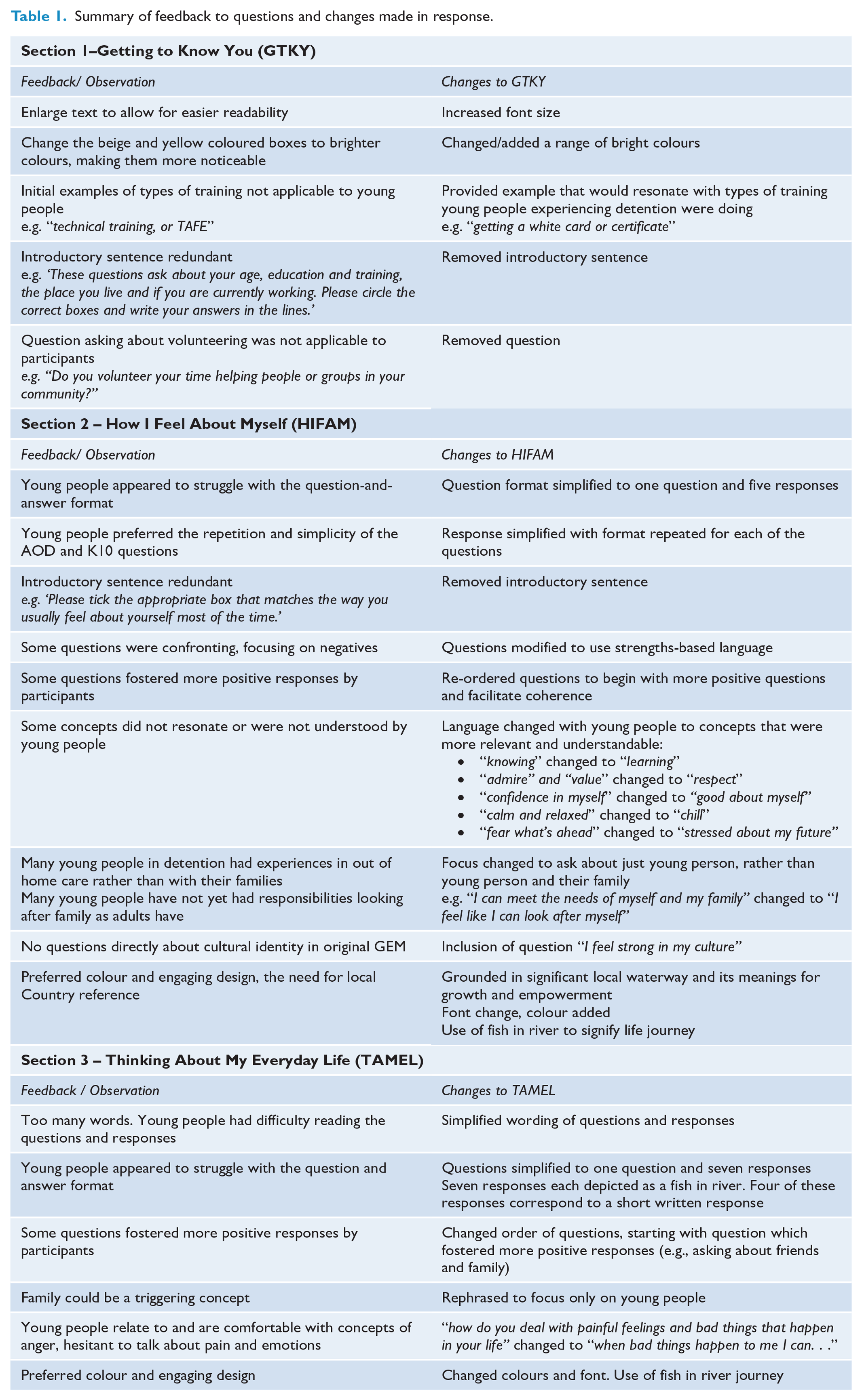
Feedback and observations from young people informed changes to language, content and design of the subsequent iterations. Specific suggestions from young people included: simplifying language, using age-appropriate language, using brighter colours, enlarging text and using easily recognisable concepts to improve readability, comprehension and engagement (Table 1). Young people helped provide alternative words to convey concepts that they did not understand, or which were not relevant to them. Following feedback from young people, questions were asked in first person to assist young people reflecting on their personal feelings and experiences; and questions were re-ordered to support coherence.
Summary of feedback to questions and changes made in response.
In making these changes, the researcher had discussions with the young people about the overall visual design of the GEM for young people. They made suggestions that prompted changes from the original visual design, grounded in the north-Queensland landscape and its feature of the Kauri pine tree. Instead, the local landscape of the significant nearby river and concept of fish swimming in the river, was created and drawn by the researcher. The design was then brought to the young people for consultation and reflection and, upon their approval, was brought to the Cultural Governance Group for endorsement. The fish movement in the river represents stages in a journey, with fish being used when answering questions (Figure 1).
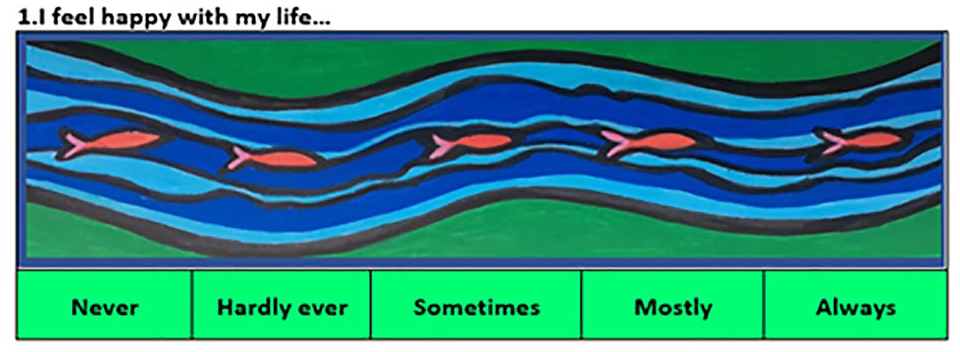
Example of fish motif used to support response format.
The GEM-Youth v7 was completed by 78 young people at their initial contact with RHF. The K10 appeared to be the preferred measured by the young people in comparison to the GEM-Youth until the GEM-Youth version 6 and version 7 were developed, at which point it was observed that young people preferred completing the GEM-Youth over the K10. Positive feedback from a speech pathologist included that the ‘visuals really help’ to provide guidance and ease of understanding of the questions, especially for young people who required literacy support.
Stage 2: validation of GEM-Youth
Internal consistency and reliability
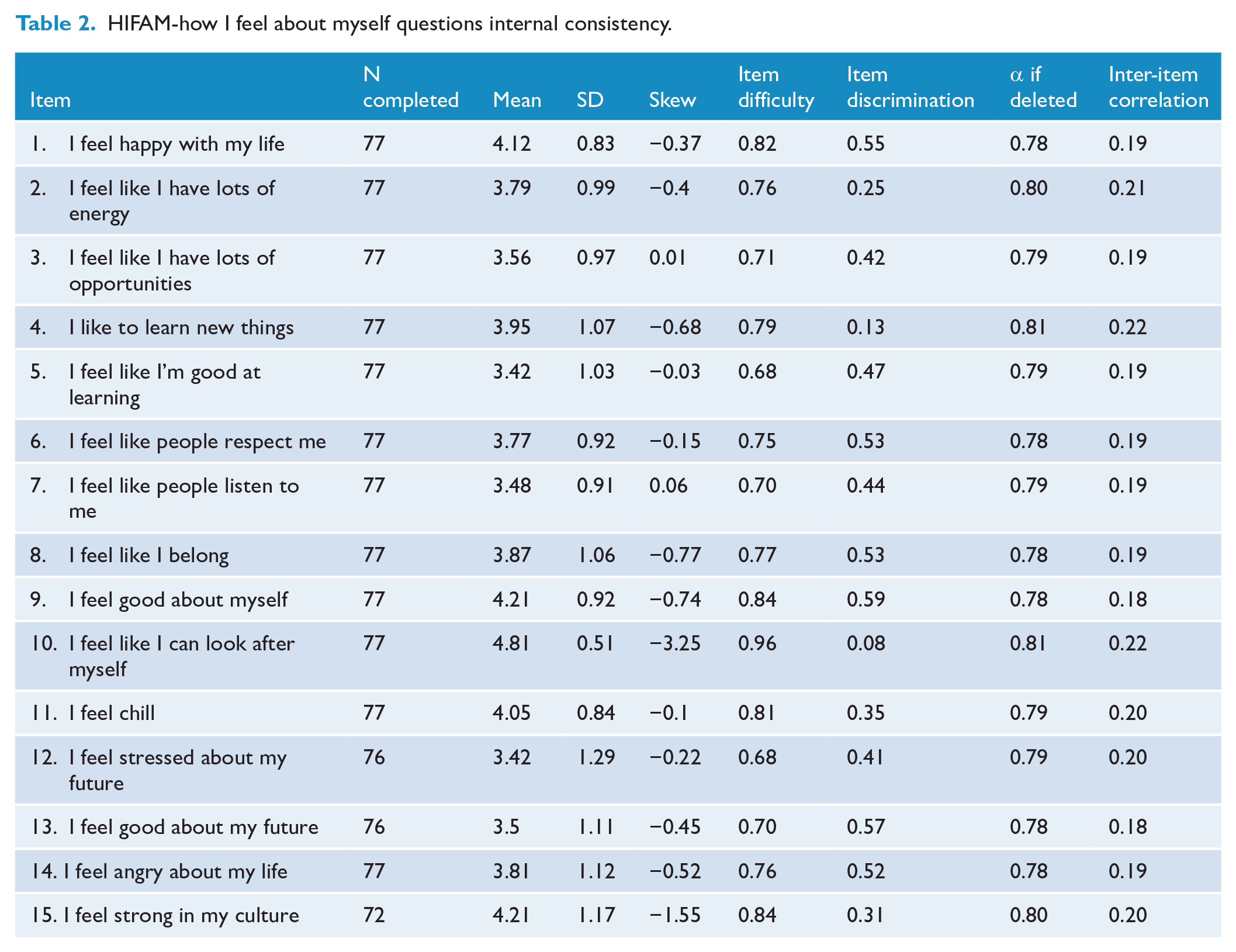
Analysis indicated that the internal consistency of the HIFAM questions is reasonable, with a mean inter-item correlation of 0.21 and Cronbach’s alpha of 0.80. The mean inter-item correlation of 0.21 suggests that, on average, the items of the HIFAM scale are moderately correlated with each other and a Cronbach’s alpha at or above 0.8 is often seen as a good level of internal consistency reliability (Table 2).
HIFAM-how I feel about myself questions internal consistency.
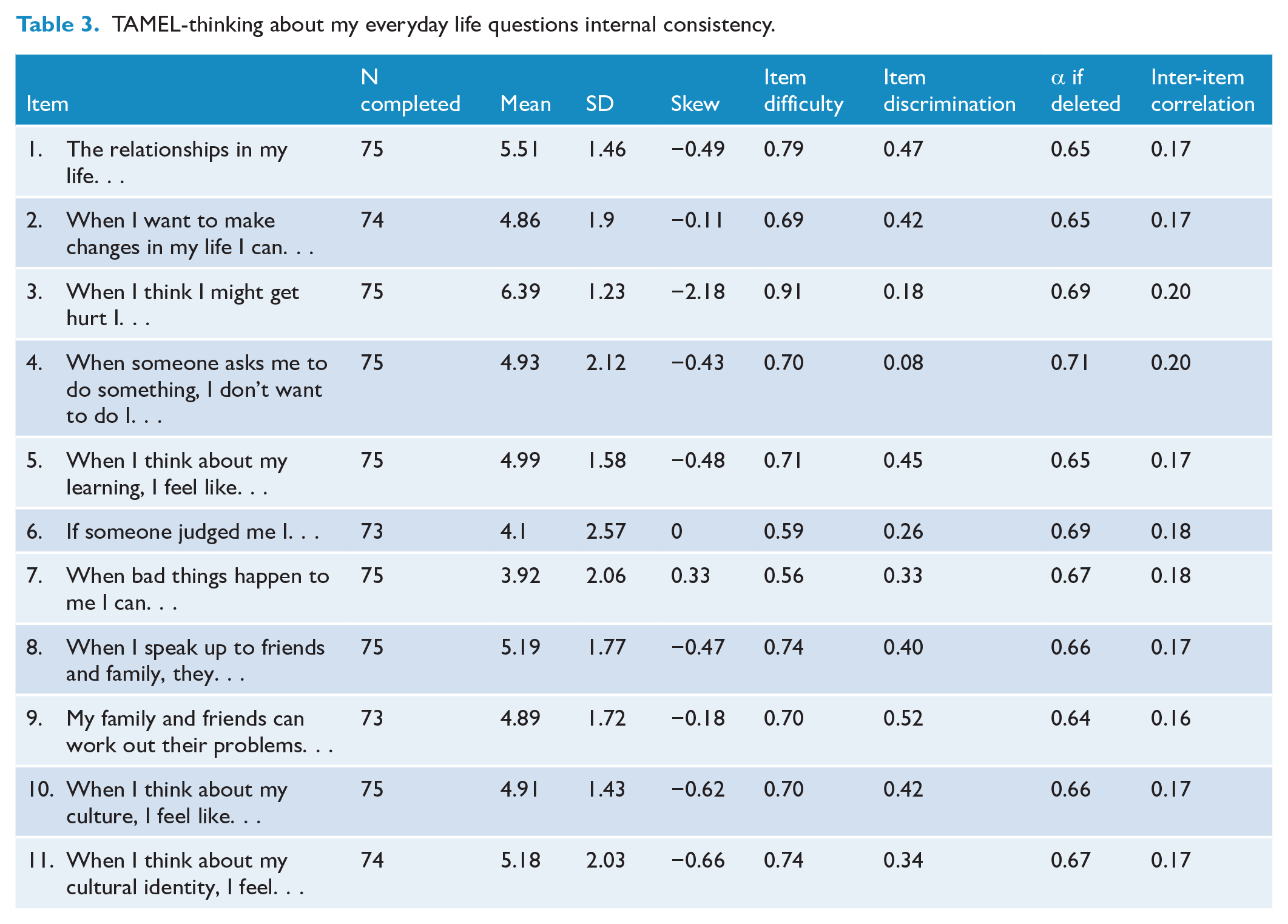
Analysis indicated that the internal consistency of the TAMEL questions is lower than the HIFAM. The mean inter-item correlation was 0.18. Cronbach’s alpha 0.69 was below the threshold range of 0.7–0.8 in this sample (Table 3).
TAMEL-thinking about my everyday life questions internal consistency.
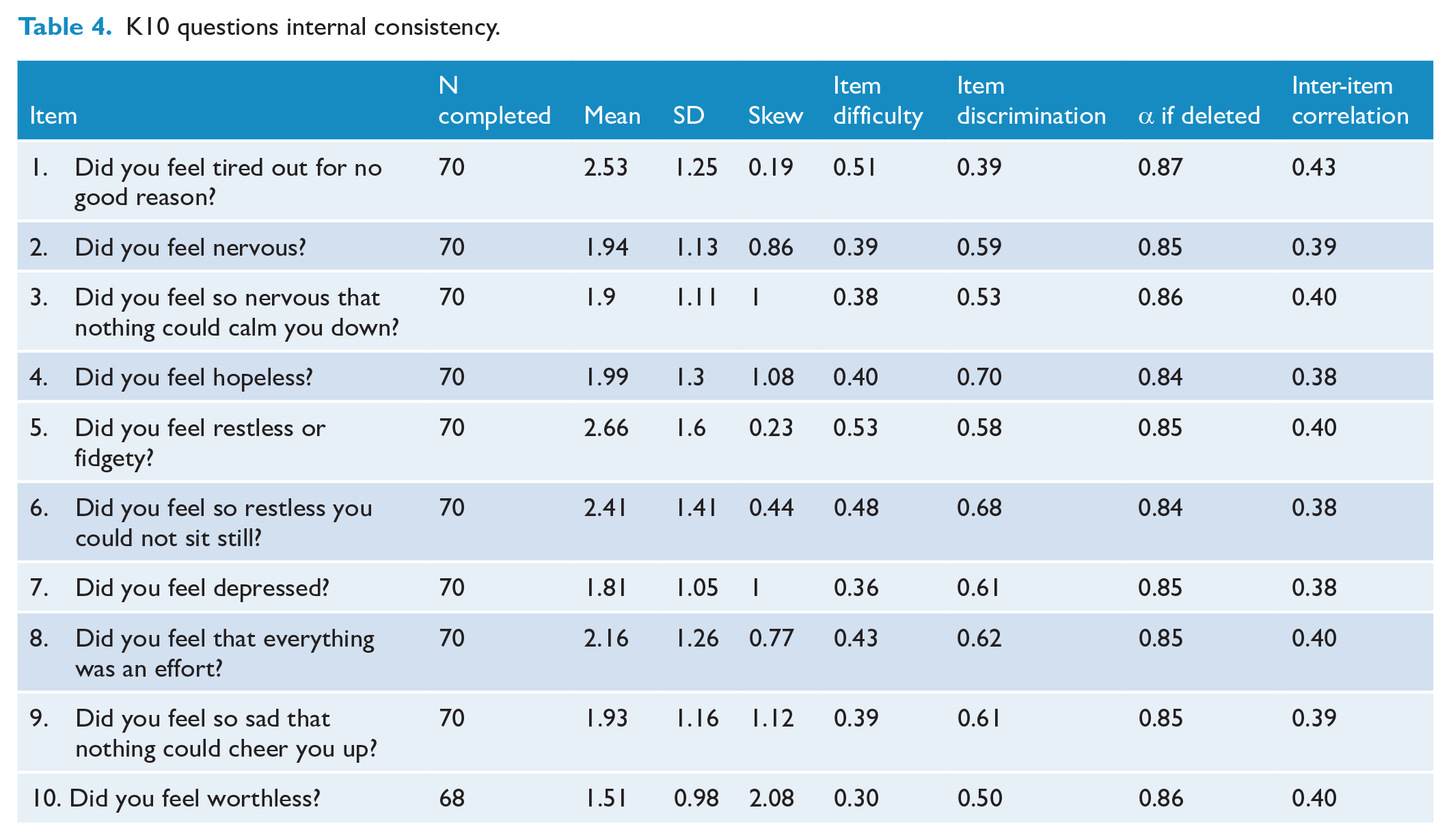
By comparison, the mean inter-item correlation for the K10 was 0.40 with a Cronbach’s alpha of 0.86; both values exceeding their thresholds for acceptability (Table 4).
K10 questions internal consistency.
Correlation analysis
Correlation analyses assessing the association between the HIFAM Score and the K10 Total score revealed a strong, statistically significant negative correlation, (r(55) = –0.61 [95% CI: –0.42, –.75] p < 0.001). Analyses assessing the association between the TAMEL Score and the K10 Total score revealed a moderate significant negative correlation, (r(55) = –0.31 [95% CI: –0.05, –0.52], p = 0.02) (Figure 2).
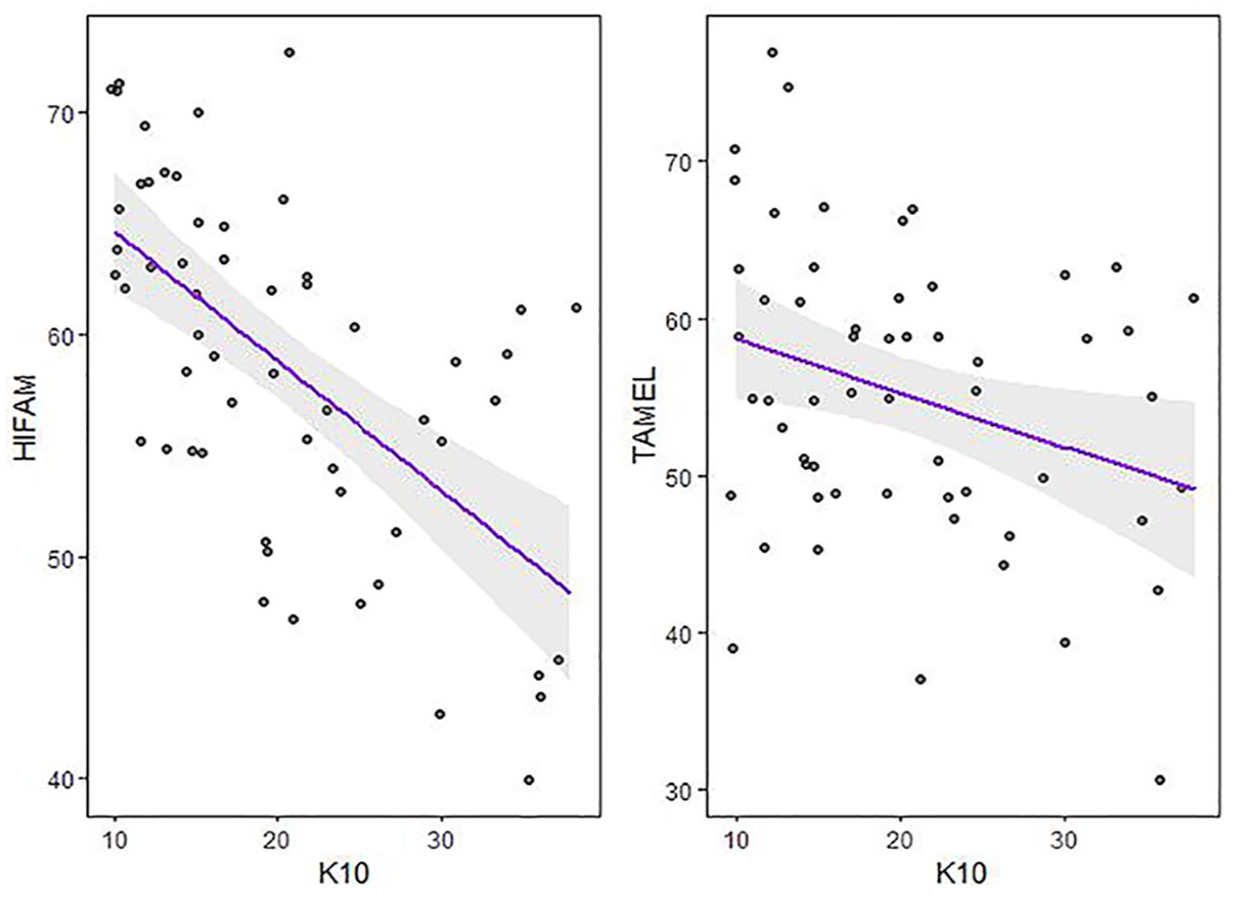
Correlation between K10 and GEM-Youth HIFAM score and TAMEL score.
Discussion
Based on a co-design process and initial psychometric validation, the GEM-Youth shows promise as a culturally valid version of the GEM for Aboriginal and Torres Strait Islander young people experiencing youth detention. The co-design process is ongoing and further refinements have been made to create GEM-Youth version 8 (Supplementary Material 2 and Supplementary Material 3).
Co-design with Aboriginal and Torres Strait Islander young people
Co-design approaches ensure that perspectives, cultural values and lived experiences are meaningfully incorporated, leading to tools that are more relevant, respectful and effective in capturing the unique aspects of their social and emotional well-being (Butler et al., 2022; Gee et al., 2024). The co-design process was based on an approach that was strengths-based and trauma-informed, in recognition of the fact that the administration of deficits based instruments may have unintended harms for young people and communities, both in their administration and reporting. Oversight by the IMHIP-Youth Cultural Governance Group additionally ensured that the research method and design of the tool was culturally grounded and empowering. Collaboration with the IMHIP-Youth Cultural Governance Group resulted in inclusion of questions relating to cultural identity, such as ‘I feel strong in my culture’, not found in the adult GEM. The original GEM does not include questions relating to cultural identity, as the overall tool relates to culture. However, since the original GEM development, inclusion of questions in surveys that directly focus on identity have become more pertinent.
Psychometric validation
The approach to psychometric validation was based on the method applied to validate the GEM adult, specifically measuring the internal consistency and reliability of the GEM-Youth with respect to its two key components: HIFAM and TAMEL as well as comparing it to the K10 via correlational analysis. The GEM adult was validated against the K6, a short version of the K10 commonly used in surveys and screening tools with Aboriginal and Torres Strait Islander populations (Haswell et al., 2010). For this study the K10 was used rather than the K6, due to the K10’s broader acceptance as a reliable measure of psychological distress internationally for the purposes of validation (Furukawa et al., 2003) as well as due to the use of the K10 in Young Minds Matter: The mental health of Australian children and adolescents thus enabling comparison of this cohort to Australian benchmarks (Hafekost et al., 2016).
Results for the GEM-Youth were negatively correlated with those of the K10, as expected. The correlation between the HIFAM and GEM-Youth, in particular, was strong, while not being too high so as to suggest the GEM-Youth simply provides a mirror image to the K10. The correlation between the TAMEL and GEM-Youth was lower but still showed a moderate negative association with K10 as expected. While these negative associations with the K10 are encouraging, it is important not to overstate their significance given that the GEM-Youth aims to measure a holistic construct of social and emotional well-being.
The HIFAM performed well with respect to examination of its internal consistency and reliability, as measured by mean inter-item correlation and Cronbach’s alpha. The TAMEL component, however, did not reach the desired threshold with respect to Cronbach’s alpha. Mean inter-item correlations of HIFAM and TAMEL (0.21 and 0.18 respectively) sat at the lower end of the theorised optimal range of 0.15–0.50 (Clark and Watson, 2019) which is consistent with what is expected of a holistic measure (i.e. measurement of a broad construct). By comparison, the K10, a measure of a narrower construct, sat at the higher end of this range (0.40).
The TAMEL arguably underwent the largest transformation from the format of the original GEM, which focussed on scenarios. Simplifications were necessary for the tool to be legible to young people and in order that the GEM-Youth could be completed in a reasonable timeframe. Nevertheless, future research should focus on examining and potentially refining this component of the tool, including potentially undertaking further factor analysis.
Generalisability
The GEM-Youth has been developed and validated with a cohort of Aboriginal and Torres Strait Islander young people within a youth detention setting. However, feedback suggests that this tool has strong potential to be used with Aboriginal and Torres Strait Islander young people across community settings and in areas outside of south-east Queensland. Further research and investigation is needed to validate the GEM-Youth across Australia, with a larger and broader participant base.
Finally, there are learnings from this process that we hope may be applicable to the development of tools and measures that can help clinicians better understand and service the needs of young people from a range of cultural backgrounds, including in western cultures. Reductionist instruments developed from a theoretical standpoint and not informed through co-design processes that facilitate lived experience involvement, may be failing to capture important complexities of young people’s experiences and needs. The process documented here of co-design and validation of the GEM-Youth provides an example of a process that could be used in other domains of practice to develop strengths-based instruments for young people to more holistically understand their perspectives and needs and track changes over time.
Limitations
Given the overall sample size as well as sex distribution of the sample, where males strongly outnumber females, findings were not disaggregated by sex. Further research with community samples could usefully examine sex differences relating to these scales. We did not undertake an examination of the factor structure of the GEM-Youth, as was done in the original validation of the GEM adult due to our using these established constructs in the context of co-design. Further work, particularly with respect to the TAMEL could investigate this. The validation was restricted to comparing the HIFAM and TAMEL with the K10 due to feasibility constraints on collecting additional measures. It is important to recognise that undertaking research within custodial settings is highly challenging due to multiple logistic constraints. In addition, the research team was conscious of the potentially taxing nature of this research with young people, including those experiencing mental health or substance use problems or cognitive impairments, as evidenced by the challenges in getting complete data on the GEM-Youth and K10 alone.
Future research directions
The GEM-Youth has been designed for use within the IMHIP-Youth research project as a culturally validated tool to evaluate success of a programme for Aboriginal and Torres Strait Islander young people who experience youth detention. However, the aim is also for this tool to be used therapeutically. Evaluation of its use as a therapeutic outcome measure will require further examination, including with respect to identifying therapeutically meaningful scores and cut-offs and further examination of test–retest reliability and sensitivity analysis.
The GEM-Youth was developed within a research, rather than therapeutic, context. The co-design process ensured that the tool resonated with young people, was strengths-based and trauma-informed. It is hoped that the use of this tool will support clinicians in developing trust and rapport with young people during their initial engagements. However, the context in which the GEM-Youth was developed may contrast to the way it may be implemented in therapeutic contexts, including that it is being used in relation to a different type of relationship (i.e. between the young person and clinician rather than a researcher) and where clinicians may be managing multiple conflicting priorities, needs and time pressures. Initial feedback of the GEM-Youth from health professionals has highlighted possible barriers for clinical use relating to the length of the tool and number of questions. Consequently, in phase 2 (implementation and evaluation of a model of social and emotional well-being care), researchers will continue to work collaboratively with programme facilitators and young people to critically assess this tool, with the potential for further refinements and/or to co-design a shortened form of the GEM-Youth that may be more applicable to busy clinical contexts or early engagement with young people while rapport and trust is being established.
Conclusion
Current and future leaders and Elders play a vital role in strengthening the social and emotional well-being of Aboriginal and Torres Strait Islander young people, using their cultural knowledge and guidance as a key to address existing gaps in health and well-being. Gaps currently exist in the availability of valid and reliable measurements for social and emotional well-being, with existing instruments developed for young people in western cultures that may be of limited validity and acceptability to Aboriginal and Torres Strait Islander young people. The co-design and validation of the GEM-Youth provides an example of a collaborative and culturally informed research approach, resulting in development of a tool that shows promise in helping to address some of these critical gaps and the potential to be used in a range of other contexts, as both a therapeutic and research outcome measure.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251324819 – Supplemental material for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people
Supplemental material, sj-docx-1-anp-10.1177_00048674251324819 for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people by Rebecca Hird Fletcher (Garigal and Walkaloa), Lisa Wittenhagen, Alyssa Cormick, Marshall Watson (Noongar), Jessica Elliott, James G Scott, Scott Harden, Stephen Stathis, Stuart A Kinner,IMHIP-Youth Cultural Governance Group, Ed Heffernan, Penny Dale (Turrbal), Carla Meurk and Megan Williams (Wiradjuri) in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674251324819 – Supplemental material for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people
Supplemental material, sj-docx-2-anp-10.1177_00048674251324819 for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people by Rebecca Hird Fletcher (Garigal and Walkaloa), Lisa Wittenhagen, Alyssa Cormick, Marshall Watson (Noongar), Jessica Elliott, James G Scott, Scott Harden, Stephen Stathis, Stuart A Kinner, IMHIP-Youth Cultural Governance Group, Ed Heffernan, Penny Dale (Turrbal), Carla Meurk and Megan Williams (Wiradjuri) in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-3-anp-10.1177_00048674251324819 – Supplemental material for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people
Supplemental material, sj-pdf-3-anp-10.1177_00048674251324819 for Development of a growth and empowerment tool (GEM-Youth) co-designed with Aboriginal and Torres Strait Islander young people by Rebecca Hird Fletcher (Garigal and Walkaloa), Lisa Wittenhagen, Alyssa Cormick, Marshall Watson (Noongar), Jessica Elliott, James G Scott, Scott Harden, Stephen Stathis, Stuart A Kinner, IMHIP-Youth Cultural Governance Group, Ed Heffernan, Penny Dale (Turrbal), Carla Meurk and Megan Williams (Wiradjuri) in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The IMHIP-Youth project team acknowledges the Traditional Owners and their custodianship of the lands on which this research project took place, the Turrbal and Jaggera peoples. We pay respect to the Aboriginal and Torres Strait Islander young people this research serves, to their ancestors and descendants and recognise their ongoing connections to and knowledges for this Country. We benefit from their valuable contributions to Australian and global society.
Author Contributions
RHF implemented and documented culturally appropriate co-design of GEM-Youth with young people within detention setting (v1–v7) and collection of K10, and produced ‘fish’ concept for answer formats. LW led data management, oversight of data cleaning and verification and was lead analyst for validation. AC collated draft manuscript and revisions and supported analysis and variation of GEM-Youth v8. JE undertook data cleaning and verification of GEM-Youth and K10. Cultural Governance Group oversighted the co-design process, reviewed and assessed from a cultural perspective. EH and SH facilitated approvals for accessing the cohort and provided clinical oversight. PD coordinated feedback via Cultural Governance Group. MegW provided feedback throughout co-design process. CM oversighted co-design activities and tasks, data management and ethics and other approvals. EH, JS, SS, SH, SK, MegW, MarW, CM obtained funding as project CIs. All authors reviewed the draft for critical content and approved submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding for this project has been provided through a NHMRC Medical Research Future Fund scheme, Indigenous Health Research Grant (grant no. APP1200300).
Ethical Approval and Informed Consent Statements
This study was approved by Children’s Health Queensland Hospital and Health Service Human Research Ethics Committee (HREC/20/QCHQ/70612), The University of Queensland Human Research Ethics Committee (2021/HE001359) and the Department of Children, Youth Justice and Multicultural Affairs (DCYJMA). We thank DCYJMA for their role in facilitating this research, but responsibility for any errors of omission or commission sits with the authors. In-custody guardian consent was provided and participants provided informed written consent to be involved in this project where possible.
Data Availability Statement
Due to the sensitivity of data gathered, raw data are unavailable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.