
Abstract

Introduction
The prevalence of co-occurring mental health and substance use disorders in Australian clinical treatment settings is between 47% and 100% (Kingston et al., 2017). This highlights the need for an addiction psychiatry workforce to support integrated care delivery, and to diagnose and manage complexity.
There is limited existing data on the Australian and New Zealand addiction psychiatry workforce to guide planning and training efforts. Previous workforce reports have outlined the acute need for root and branch reformation of the addiction psychiatry workforce, acknowledging the lack of training opportunities, the funding model not supporting the clinical service (The Royal Australian & New Zealand College of Psychiatrists (RANZCP), 2017) as well as concerns about succession planning (Department of Health, Australian Government, 2016). In addition, the discrepancy between gender and the disproportionate concentration of those working in metropolitan areas have previously been highlighted (Department of Health, Australian Government, 2016; RANZCP, 2017).
This study was undertaken to address a gap in existing workforce data by scoping the current demographic and practice profile of addiction psychiatrists in Australia and New Zealand, highlighting the strengths and limitations of the current workforce.
Methodology
An anonymous online survey was designed with REDcap (Harris et al., 2009, 2019), adapting elements from previous medical workforce studies in Australia and New Zealand (Lau et al., 2004; RANZCP, 2014). This comprised 26 questions, relating to demographic data, professional training, current clinical practice, factors influencing clinical/geographical location, retirement plans and non-clinical roles. To preserve anonymity, we did not collect specific information about the location of practice (other than the state) or practice. Participants included consultant psychiatrists differentiated into two groups based on years of experience: early mid-career psychiatrists (EMCPs, ⩽20 years) and late career psychiatrists (LCPs, ⩾21 years) and trainees.
The survey was distributed via email to the RANZCP Faculty of Addiction Psychiatry mailing list in February 2023 (553 members including 146 accredited members with a Certificate of Advanced Training in Addiction Psychiatry, or equivalent experience/qualifications in the field; 407 general members with an interest in addiction psychiatry); and promoted via word of mouth at the February 2023 International Medicine in Addiction Conference in Melbourne, and at the Addiction Advanced Training weekly training programme. Ethics approval by Monash University was provided for this study (Project ID 36635).
Results
A total of 102 responses were received, comprising 69 consultant psychiatrists, 8 general psychiatrist fellows undergoing addiction training and 25 psychiatry trainees. Fifty-seven of 146 (39%) accredited members of the Faculty of Addiction Psychiatry answered the survey. Detailed characteristics and comparisons between EMCP and LCP groups are presented in Table 1.
Demographics and survey responses by consultant psychiatrists, with comparison of responses between EMCP (⩽20 years) and LCP (⩾21 years).

EMCP: early mid-career psychiatrist; LCP: late career psychiatrist; SD: standard deviation; RANZCP: The Royal Australian & New Zealand College of Psychiatrists; OST: opioid substitution therapy; FAChAM: Fellowship of the Australasian Chapter of Addiction Medicine; N/A: not applicable.
Demographics
The consultant group included 22 women (29%), two participants did not disclose their gender; mean age was 50 years (standard deviation [SD] = 12.4). Eighty-five per cent of respondents worked in Australia, with the majority practicing in Victoria (36%), followed by Queensland (30%) and New South Wales (20%). The majority gained their medical degree (72%) and completed Addiction Psychiatry training (63%) in Australia or New Zealand.
Training
Forty-nine per cent of respondents had a Certificate of Advanced Training in Addiction Psychiatry, with 68% completing the RANZCP Psychiatry Advanced training programme. Twenty-three per cent had attained Fellowship of the Australasian Chapter of Addiction Medicine.
Clinical work
Seventy-five per cent of respondents were currently working in the field of addictions and 65% in general psychiatry. Ninety-six per cent were predominantly treating adult patients. The most common places of work were public community mental health services (65%), public community drug and alcohol services (33%) and private outpatient clinic (35%). Forty-four per cent of the consultants worked entirely in public, 18% entirely in private and 34% in both. Fifty-five per cent reported prescribing opioid substitution therapy (OST). The majority of respondents worked full-time (71%). Thirty-nine per cent reported involvement in research, 74% in formal teaching and 46% were a supervisor for addiction psychiatry advanced certificate trainees.
EMCP vs LCP
Of the respondents, 43 (70%) identified as EMCPs and 18 (30%) as LCPs, with more female EMCPs compared to female LCPs (42% vs 15%; Table 1). A higher proportion of EMCPs worked in addictions as their primary field of work compared to LCPs (88% vs 50%; Table 1). Many EMCPs (51%) and LCPs (45%) worked in the public sector, although more LCPs worked solely in private practice (30% vs 9%; Table 1). Seventy per cent of LCPs planned to retire or semi-retire within the next 5 years.
Factors influencing the geographic and clinical area of practice differed between the groups and are presented in Figure 1. EMCPs reported the following as important factors when compared to LCPs: financial remuneration (54% vs 20%), non-salary benefits (42% vs 10%), lifestyle and recreational activities (63% vs 25%) and raising children (51% vs 5%).
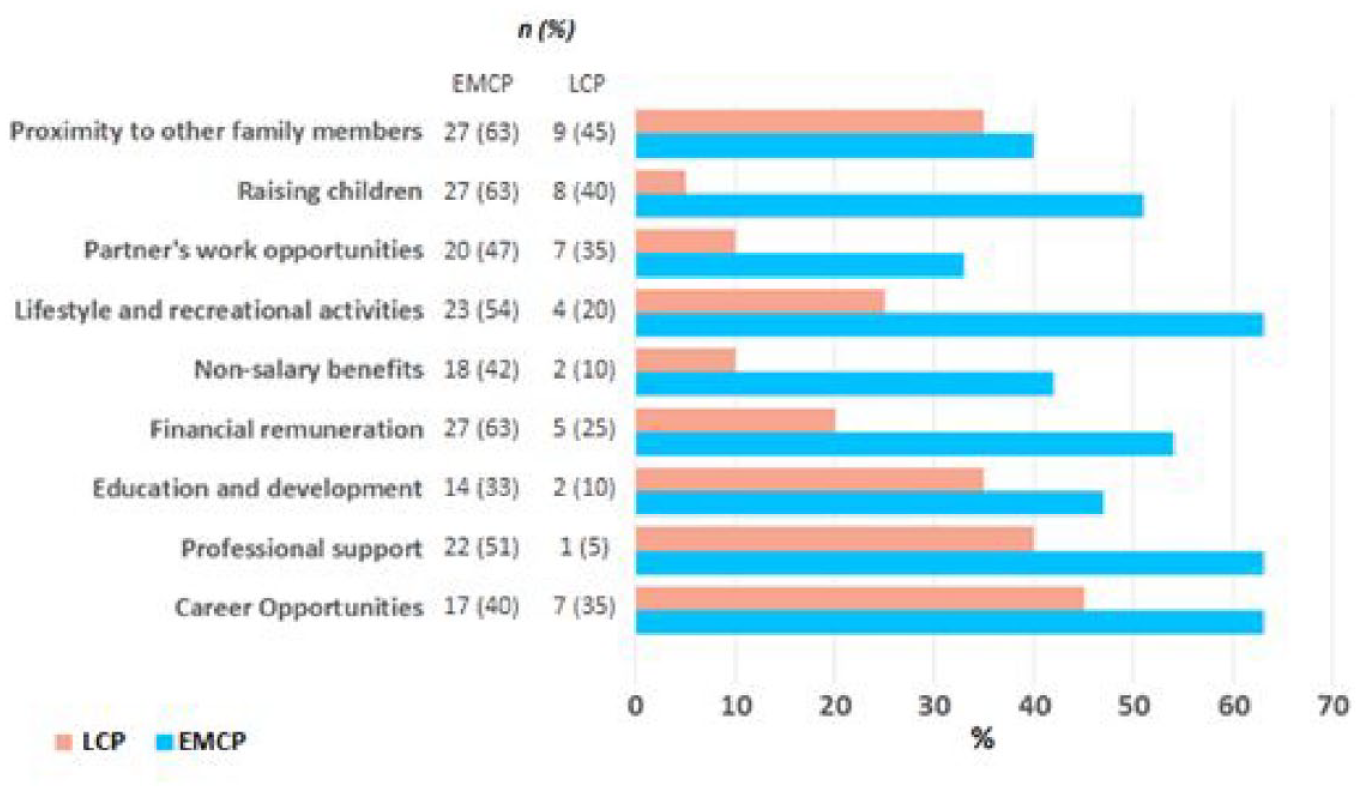
Factors deciding geographic or clinical area of practice.
Discussion
The addiction medicine and psychiatry workforce in Australia and New Zealand face challenges in relation to growth, ageing and succession planning (Department of Health, Australian Government, 2016). To our knowledge, this is the first study to gather detailed contemporary characteristics of the Australian and New Zealand addiction psychiatry workforce. This survey provides useful insights to inform workforce planning, highlighting the characteristics and work intentions of trainee, EMCPs and LCPs. Relevant to this survey is the context that the addiction psychiatry faculty currently has record numbers of trainees binationally (n = 105), reflected in our high survey response from trainee and EMCP groups. Although the overall response rate was low, this was comparatively high when considering response rates in previous Australian psychiatrist surveys (RANZCP, 2014). Given the highest response was from Victoria, survey data may not be representative of the overall binational workforce.
The survey found that the mean age of the respondents was 50 years (SD = 12.4) with higher responses from EMCPs (68%) compared to LCPs (32%). While the current workforce is predominantly male, when looking into the future, the gender disparity appears to be improving with increase in female addiction psychiatrists among the EMCP (42%) compared to LCP (15%). This is in keeping with the overall trend of increased number of female doctors within the Australian general medical workforce (Department of Health, Australian Government, 2021).
The majority of surveyed participants recording addictions as the primary field of work (75%) serves to be a strength of the current workforce, with future trends likely to maintain this given the high proportion of EMCP currently working within the field of addictions (88%). The addiction psychiatry workforce predominantly saw adult patient groups, raising concern of the potential lack of support for the high-priority populations including the youth and older adults (Department of Health, Australian Government, 2017). The majority of respondents worked in the public sector, with only 12% of respondents working entirely in private practice, compared to 31% of the Australian psychiatric workforce (Lau et al., 2004). Contributing to these workforce patterns may be the lack of training or clinical opportunities available for addiction psychiatry in practice areas such as the private sector or with populations other than adults.
Psychiatrists reported high rates of participation in research, formal teaching and supervision, as well as a majority reporting active OST prescribing (55%). While encouraging, this may reflect bias based on the majority of respondents working in the public sector.
The proportion of surveyed consultants working full-time (71%) is in keeping with the broader psychiatric workforce. However, more than half (56%) of registrars planned to work part-time upon fellowship with 27% of consultant respondents considering retirement within the next 5 years. There may be ongoing workforce shortages unless efforts are made to attract and promote addiction psychiatry. The availability of clinical opportunities that align with professional, location and personal priorities including lifestyle and family is also needed. A better understanding into the barriers to working in addiction psychiatry, particularly in regional and remote areas, is needed and should be explored in future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.