
Abstract
Objective:
Culturally safe service provision is essential to improving social and emotional wellbeing among Aboriginal and Torres Strait Islander communities, and to eliminating health inequities. Cultural safety is about ensuring that all people have a safe and healing journey through services, regardless of their cultural background. In this project, we aim to (1) understand how Aboriginal and Torres Strait Islander peoples conceptualise cultural safety, and (2) co-design a qualitative interview for the next phase of this project, where we plan to learn about experiences of cultural safety within mental health services.
Methods:
We conducted six focus groups (in one metro and two regional areas, Western Australia). Following an Aboriginal Participatory Action Research methodology, we yarned with Aboriginal and Torres Strait Islander mental health service users, carers, community members, mental health professionals and Cultural Healers about cultural safety.
Results:
Participants described a culturally safe service as one where Aboriginal cultural knowledges, life experiences, issues and protocols are understood and acknowledged, and reported that mainstream mental health services are not currently culturally safe. Participants emphasised the importance of building trust, rapport, reciprocity and following appropriate relational processes when designing a qualitative interview for the next phase.
Conclusions:
A lack of cultural safety in mental health services is likely to contribute to the disparity in outcomes between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians. Embedding cultural safety into research design allows for authentic community engagement and facilitates knowledge sharing around ways to improve cultural safety in mental health services.
Keywords
Aboriginal and Torres Strait Islander peoples lived and thrived in Australia for 60,000 years prior to colonisation (Dudgeon et al., 2014b; Milroy et al., 2014). The legacy of colonisation, including past and ongoing discrimination, dispossession and the undervaluing of Indigenous knowledges around health and wellbeing, has contributed to a disparity in mental health outcomes between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians (Australian Institute of Health and Welfare, 2016; Australian Psychological Society, 2016; Dudgeon et al., 2014a). There is an urgent need to develop an evidence base to help enable advocacy, and ultimately improve mental health service provision for Aboriginal and Torres Strait Islander peoples and communities. One potential way to improve service provision is by improving the level of cultural safety in mainstream mental health services (National Strategic Framework, 2017).
Culturally safe practice considers culturally relevant concepts of health and wellbeing (e.g. social and emotional wellbeing; Gee et al., 2014). It requires an understanding of the power dynamics in and between cultural groups and applies empowering approaches to working with people seeking support for mental health issues (Curtis et al., 2019; Elvidge et al., 2020; National Strategic Framework, 2017; Ramsden, 1993; Walker et al., 2014). Our overall aim is therefore to develop a ‘Cultural Safety Framework and Practice Guide’ based on the results of this research project.
A first step in developing an evidence base to improve cultural safety is to embed cultural safety into the research process itself (Milroy et al., 2022). Colonisation and related discourse remain evident in mental health research (Dudgeon et al., 2014a; Kennedy et al., 2022), and for the knowledge generated in any research project to be meaningful to Aboriginal and Torres Strait Islander communities, the process of the research needs to be culturally safe (Lindeman et al., 2011; Lindeman and Togni, 2022). In this paper, we aim to summarise findings from a co-design process related to cultural safety that sits within a larger programme of research. First, we summarise how focus group participants conceptualised cultural safety and described their experiences of engaging with mental health services. Second, we summarise qualitative feedback from participants with regard to how mental health services can improve cultural safety. Finally, we summarise some of our learnings as a research team with respect to designing and administering a qualitative interview protocol and online survey. The purpose of the interview and survey is to gain a deeper understanding of the experiences of Aboriginal and Torres Strait Islander mental health service users, carers, community members, mental health workers, Elders and Cultural Healers with regard to cultural safety.
Methods
Participants
Participants were 19 adult (+18 years) Aboriginal and/or Torres Strait Islander mental health service users, carers, mental health workers, Elders and Cultural Healers. Focus groups were conducted in metropolitan (Perth) and regional (the Great Southern and Kimberley regions) Western Australia. We conducted six focus groups, and there were between three and eight participants in each focus group session. Participants of two focus groups were Aboriginal mental health workers based at local Aboriginal Community Controlled Health Organisations (ACCHOs), in the Perth metro area and in the Kimberley region. Participants of two focus groups were Elders, community members, service users and carers located in the Perth metro area, and in the Great Southern region. Participants of the remaining two focus groups were Cultural Healers. Maban Healers (including support staff) from the Kimberley region participated in one group, and Ngangkari (including an interpreter) from the Ngaanyatjarra, Pitjantjatjara and Yankunytjatjara Women’s Council participated in the other group. The focus groups with Cultural Healers were conducted in Perth.
More detailed demographic data were not collected for any participants, as this was part of the pre-data collection, formative co-design phase of the project. Furthermore, given the small number of focus groups and small number of participants, and due to the sensitivity of topics being discussed, we did not collect more detailed demographic data to protect participants’ anonymity and confidentiality. Participants were recruited by senior team members and community co-researchers within partner ACCHOs, and informed written consent for participation was received from all participants.
Procedure
The significance of culturally safe research processes, and a detailed description of the research process that we followed for this project, is outlined in a separate paper (Milroy et al., 2022). In that paper, we outlined the processes related to conceptualisation and design of the project, the development of focus group questions, decisions around how the sessions should be run and who should facilitate them, and why (Milroy et al., 2022). Here, we will provide a summary of the procedure we followed.
Consistent with Aboriginal Participatory Action Research (APAR) methodologies (Dudgeon et al., 2020), this project was led and governed by senior Aboriginal clinicians and researchers to ensure Indigenous governance. Furthermore, ethical guidelines outlined by the National Health and Medical Research Council of Australia (2018) were followed to ensure that the voices of Aboriginal and Torres Strait Islander peoples were empowered, to embed cultural safety in the research process and to enable high-quality research, where results would be meaningful to Aboriginal and Torres Strait Islander communities (Harfield et al., 2020). Non-Indigenous team members were provided with cultural awareness training (as a first step towards working in a culturally safe way), in addition to having an opportunity to participate in a cultural exchange programme that fostered self-reflexivity. Finally, ethics approval from the appropriate governing committee was received (WAAHEC HREC1037).
Focus group sessions
Focus group sessions were run with the aim of understanding clear, sensitive and culturally appropriate ways of yarning with Aboriginal and Torres Strait Islander peoples about experiences in mental health care, to co-design a qualitative interview about cultural safety in mainstream mental health services. We will administer this co-designed interview in the second phase of the project (Milroy et al., 2022).
Senior Aboriginal team members facilitated six focus group sessions in one metro and two regional areas (two sessions with Cultural Healers, two with community members and two with mental health and social and emotional wellbeing workers) using a yarning methodology (Bessarab and Ng’andu, 2010). Yarning is a culturally safe data collection method that privileges Indigenous knowledge systems (Kennedy et al., 2022). Yarning does not only focus on data collection, but it is also a method that includes relationship building, and establishing connections with Aboriginal or Torres Strait Islander participants prior to collecting information through the sharing of stories, or narratives (Bessarab and Ng’andu, 2010).
Questions for the focus group sessions were designed in consultation with senior Aboriginal research team members involved in the larger Transforming Indigenous Mental Health and Wellbeing project (https://timhwb.org.au/). It was agreed that these questions would be adapted appropriately for participants in each session, and during each session as required. Focus group questions were divided into questions about cultural safety in mental health services, and questions about co-designing a qualitative interview protocol for Phase 2 of the research project.
Focus group sessions ran for between 120 and 180 minutes, and were catered for appropriately (e.g. lunch, snacks, tea/coffee). Participants were each compensated for their time and knowledge sharing with a $100 gift voucher. Research team members typed out responses from participants during the group, and whenever it was possible, the computer screen was projected onto a big screen so that participants could see what was being typed. Participants were therefore able to amend or correct the record as needed. Participant responses were then summarised by the research team.
Cultural validation
The research team presented summaries of participant responses to participants for validation, either via online meetings (due to COVID-19-related restrictions) or in written form for feedback. In line with an APAR approach, this process ensured that participants had oversight over how their feedback had been interpreted, and were provided a further opportunity to contribute to the project. Feedback from these summary sessions confirmed that participants’ views had been accurately reported and summarised by the research team. Participants also provided additional comments and feedback, which were then incorporated into the results. Following participant validation of the results, the research team conducted a reflexive thematic analysis on the summaries. Emerging themes aligned well with the Indigenous Allied Health Australia (IAHA; 2019) framework of Aboriginal ways of knowing, being, and doing, and so we used this as an organising framework for the data.
Finally, in consultation with and under the guidance of an Aboriginal Reference Group, we used the results of the focus group to inform the design of the qualitative interview protocol, and the design of a brief online survey to administer to a wider group of participants during Phase 2. Please refer to Supplemental Material Appendix A for the qualitative interview protocol, and Supplemental Material Appendix B for the online survey protocol.
Results
Here, we will present a summary of participant responses to (1) questions around the concept of cultural safety, (2) questions around how mental health services can improve cultural safety and (3) questions around how to design a clear, culturally sensitive and appropriate interview protocol for Phase 2. We stress that the views of participants presented here do not represent the views of all Aboriginal and Torres Strait Islander peoples. It is important to highlight the diversity in Aboriginal and Torres Strait Islander cultures, and views on mental health and social and emotional wellbeing. Rather, we aim to describe the results of our co-design process with this targeted group of participants. We hope to engage with a wider, more representative sample of people during the second phase of this project, with a culturally safe qualitative interview schedule, developed based on learnings from this phase.
The concept of cultural safety
When asked about the meaning of Aboriginal cultures, participants defined culture as something that is a part of ‘who we are’, and as something that is innate. Aboriginal cultures were also described as forming a person’s worldview, e.g. that Aboriginal peoples look at the world through Aboriginal eyes, listening to liyan, and that this influences how people communicate with each other and the words individuals use.
Liyan is a Yawuru word that is recognized across the Kimberley and describes Aboriginal peoples’ connection to self, family, community, country, culture & spirituality. Liyan is all that we are as Aboriginal people and includes everyone and everything around us. When Liyan is strong people are healthy & happy, when Liyan is weak or ‘no good’ people might be unwell, stressed, or sense that something is not right either with themselves, someone they know, or in the environment they are in. What is often spoken about with our mob are the circumstances around the passing of someone, Aboriginal people will often talk about how their Liyan was not good or was a bit off when they learn of the passing of someone, and that explains why their Liyan was impacted, because that connection to the person resulted in their liyan being affected because of that person passing. (Zaccariah Cox, personal communication, 13 January 2023)
Cultural identity
Participants described cultural identity as a sense of belonging, relating to factors such as a person’s role in their family and community, values, beliefs, what is allowed, communication style and how this may impact on communication and connection with clinicians in mental health services. Participants said that cultural identity is ‘everything’ in terms of how a person’s care needs should be assessed.
What does cultural safety mean to you?
Participants described their understanding of a culturally safe service as one where Aboriginal cultural knowledges, life experiences, issues and protocols are understood and acknowledged. For example, programmes built around language and culture can encourage a strong sense of pride, knowledge and ownership of connection to culture and Country.
Participants said that issues around cultural safety in mental health services are different compared to other types of general health services. For example, participants noted that there is more stigma with mental health issues, where people might worry about privacy and confidentiality. Another difference identified by participants is that mental health services often need to work more with families and communities (rather than just the individual service user) in comparison with other types of health services.
Participants also noted that a culturally safe service is one where Aboriginal staff are safe from lateral violence.
Do you feel mainstream mental health services understand Aboriginal peoples and their culture?
Responses were a resounding ‘no’, and that services do not consider Aboriginal ways of being, e.g. not understanding men’s and women’s business, lore and kinship systems. Participants noted that some non-Aboriginal mental health workers do try to understand Aboriginal ways of being, but due to the often-high turnover of staff, there is an overwhelming burden on Aboriginal mental health workers to keep training new staff.
How can mental health services build cultural safety?
Perspectives of Cultural Healers
Researchers met with representatives from two groups of Cultural Healer organisations (including Healers, support staff and interpreters) to discuss issues around cultural safety in mental health services. Because some of the Healers used different mediums to respond to questions (e.g. drawings, principles in language, cultural knowledge), we first present their answers, followed by a summary of all other participant responses. Below is a summary of the Healers’ responses.
The current state of mental health services
Cultural Healers reported that people in rural communities have limited access to mental health workers, and these workers only treat people with severe issues. In addition, mainstream mental health was described as ‘rigid’ and focussed on diagnosis and treatment that ‘shuts the door’ for many Aboriginal consumers. Furthermore, the mainstream system treats only the individual rather than engaging and working with the family/community system and doesn’t account for all the other factors at play, such as ongoing stress associated with financial issues, cultural obligations and racism. This was described as ‘like trying to fit a circle into a box’. Cultural Healers viewed mental health agencies as currently working in silos and described how they do not address issues of ‘survival stress’ well.
Improving cultural safety
Cultural Healers reported that to improve cultural safety, mental health service providers needed a cultural advisor, and someone based on Country to prevent a disconnect between management and what is happening on the ground. Furthermore, service priorities should include helping with basic survival (e.g. support around getting a drivers licence).
When asked how mainstream services can collaborate with Cultural Healers to improve cultural safety, one group of Healers outlined some principles of cultural safety. These principles emphasised a collaborative way forward, with Healers and mainstream services ‘walking together in friendship’. Healers also discussed non-Indigenous and Aboriginal peoples’ ways of being as working together to ensure the best outcomes for a person, through respectful relationships based in trust, or ‘two ways, one path’.
The Healers then outlined principles that govern their approach to healing, and that are important in determining how mainstream mental health services can work in partnership with Cultural Healers. The Healers used words and artwork (e.g. Figures 1–3) to explain some of the concepts outlined below.
Utulu Kutjungku Atunymara Kanyintaku: When everybody works together and is united to hold a person, so they are safe, under the umbrella of families.
Malpara-Malpara: Working together as friends, ongoing, moving forward on a journey (see Figure 1).
Nyakukatima, Palyakatima, Wangkatima: Looking (while going along), doing/acting (while going along), talking (while going along).
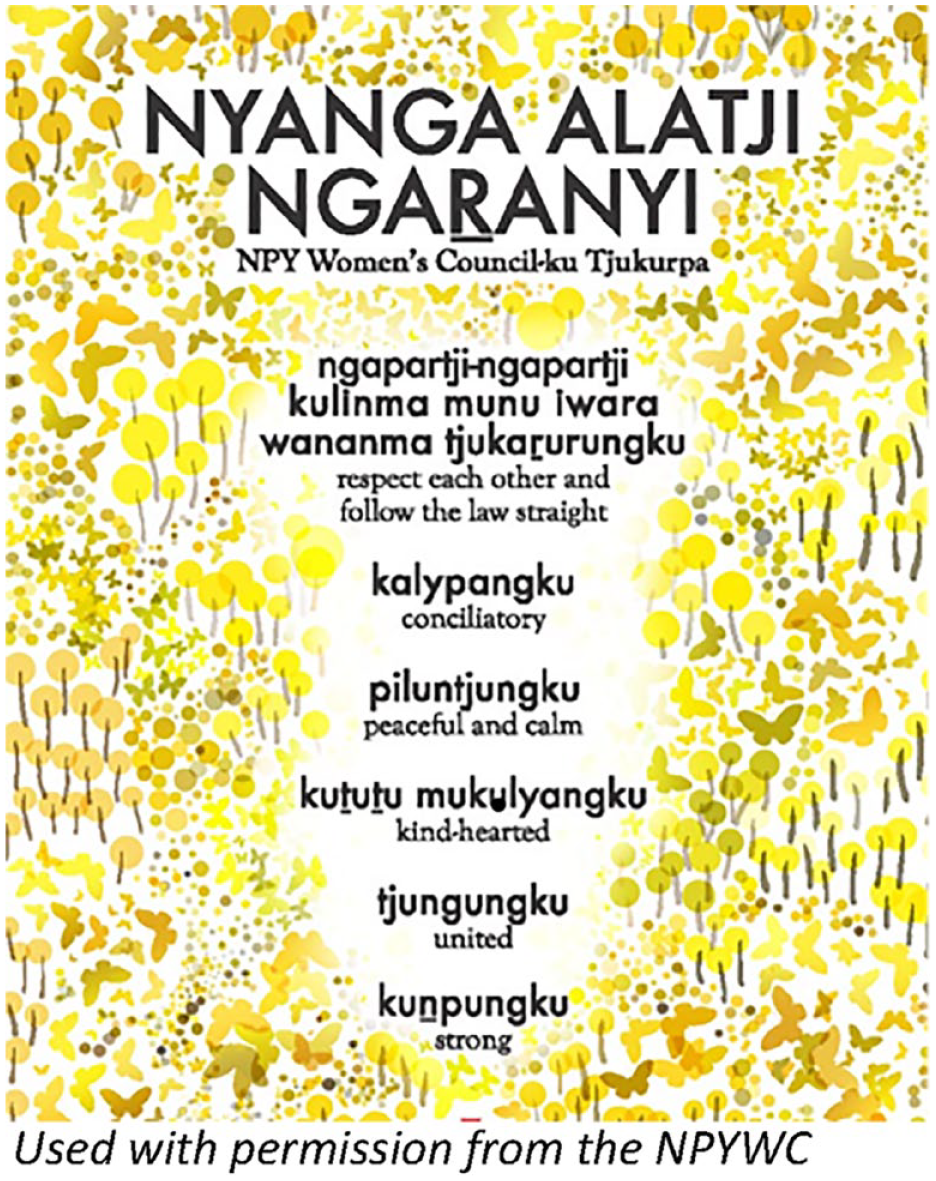
Principles followed by the NPYWC.
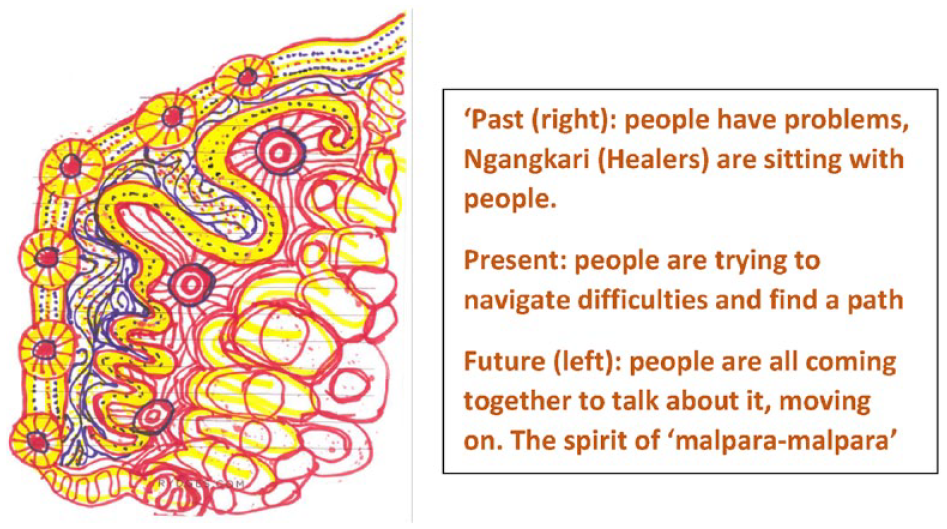
Drawing depicting the spirit of ‘malpara-malpara’.
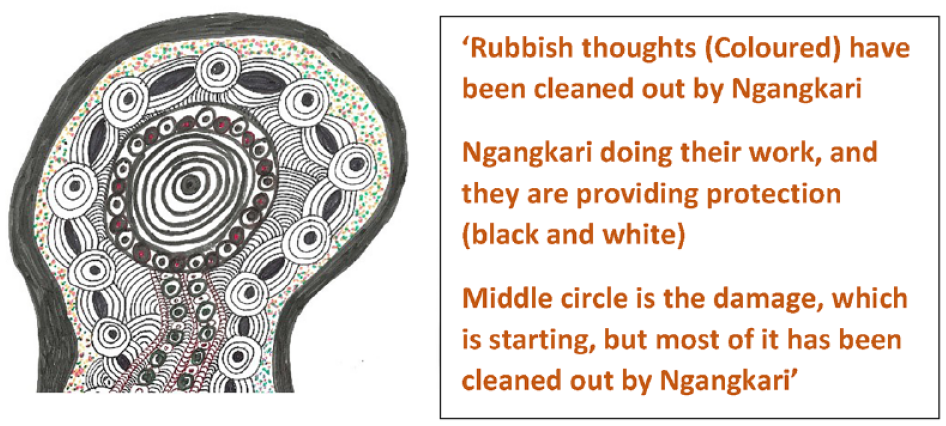
Drawing describing healing work for mental health issues.
Combined participant responses to ‘how can services build cultural safety?’
Participant responses were summarised, and following a thematic analysis, themes were organised according to the IAHA (2019) framework of Aboriginal ways of ‘knowing, being, and doing’. Responses were coded under each theme by two researchers independently, and then a third researcher (a senior Aboriginal researcher) resolved any discrepancies and refined wording. The initial list of items under each theme was then presented to the Aboriginal Reference Group, during the consultation process around how we can use information gathered during focus groups to design the protocol for a qualitative interview, and items were further refined based on feedback from this group. Please refer to Supplemental Material Appendix B for a full list of items, and Figure 4 for a diagram that illustrates our preliminary understanding of how mental health services can build cultural safety based on the information gathered during focus group sessions. We also used these themes and items to design a brief online survey (see Supplemental Material Appendix B).

Summary of participant responses around how mental health services can build cultural safety through Aboriginal ways of knowing, being, and doing; a preliminary understanding, based on Phase 1 (co-design phase) of this project.
What are culturally sensitive and clear ways to administer an interview protocol about cultural safety in mental health services?
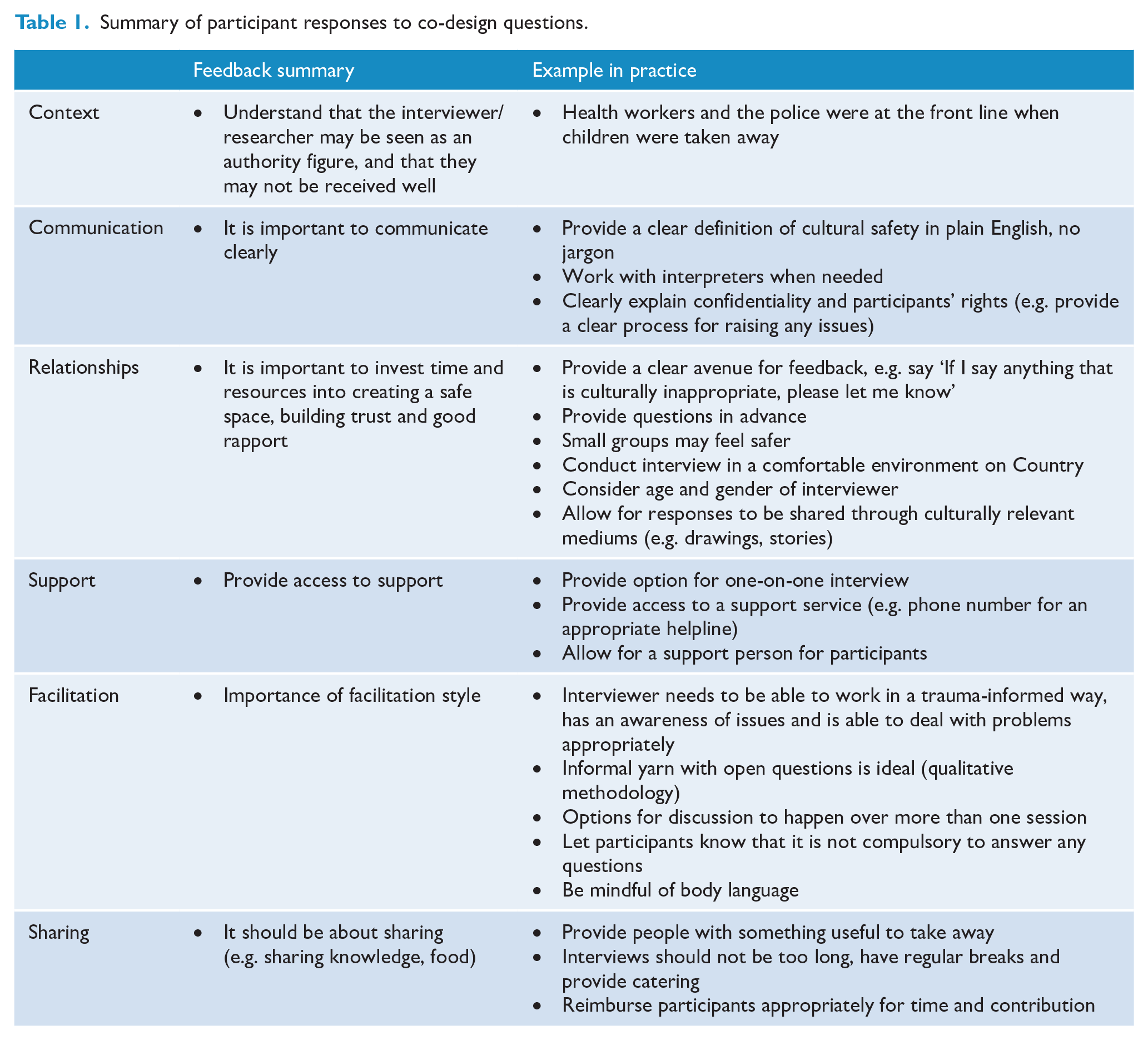
Table 1 provides a summary of participant responses around culturally safe ways of yarning with Aboriginal and Torres Strait Islander peoples about experiences of engaging with mainstream mental health services.
Summary of participant responses to co-design questions.
Discussion
In this paper, we provide a summary of the knowledges shared during the co-design phase of a research project. Our project aims to understand the key characteristics of a culturally safe mental health service for Aboriginal and Torres Strait Islander peoples, with the ultimate aim of developing a ‘Cultural Safety and Framework Practice Guide’ that can be used by mental health services. A critical component of our project is embedding cultural safety into our research process, including through co-designing the research project. In this paper, we aimed to better understand (1) Aboriginal and Torres Strait Islander peoples’ conceptualisation of cultural safety, (2) how mental health services can improve cultural safety and (3) how to design a clear, culturally sensitive and appropriate interview protocol to have a more in-depth yarn about peoples’ experiences of cultural safety when engaging with mental health services (Phase 2).
During this co-design phase, we were guided on the design and administration of a semi-structured qualitative interview protocol, and an online survey for Phase 2 of our project. The co-design phase involved consulting with Aboriginal and Torres Strait Islander service users, carers, community members, mental health workers, Elders and Cultural Healers from different regions in Western Australia for focus group discussions, as well as consulting with an Aboriginal Reference Group.
What we learned from this co-design process overall is that a lack of cultural safety in mental health services is likely to contribute to the disparity in mental health outcomes between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians. Indeed, there was broad consensus among Aboriginal and Torres Strait Islander participants that services are not currently culturally safe, and that there is significant work to do. We learnt that factors including cultural identity and an acknowledgement of Aboriginal and Torres Strait Islander cultures are crucial for cultural safety.
We also learnt that embedding cultural safety into research processes encourages the sharing of knowledges that typical Western quantitative methods of data collection probably would not. E.g. because we were flexible in how we collected data and information (e.g. including stories and artwork), Cultural Healers were perhaps more willing and able to communicate concepts such as ‘malpara-malpara’, and we were able to understand ‘malpara-malpara’ in a more integrated manner (i.e. an explanation in both words and artwork). This is significant information that we would not have otherwise known about, and our research is richer for it. We collected data through stories and artwork because we were aware of the value of these culturally relevant mediums of communication, further emphasising the importance of Indigenous governance.
Furthermore, guidance for how to develop and administer a qualitative interview to understand this issue in more detail highlights the importance of building trust, rapport, reciprocity and following appropriate research and relational processes. These processes include understanding context, communication, support, facilitation, sharing and relationships.
Limitations
The co-design phase would have been strengthened if we were able to meet with the Cultural Healers (Ngangkari and Maban) on Country, rather than in Perth. However, travel was restricted due to COVID-19 travel restrictions, and so we met with both Healer groups when they were in Perth for a conference that we organised. Meeting with the Healers on Country may have resulted in engagement with a larger number of Healers, and may have allowed us to learn more about how mental health services can better work with Cultural Healers while on their respective Countries. Furthermore, we could have spent more time relationship building with participants from one region, e.g. we could have made two trips instead of one. This would have given the research team a better sense of the context at the time, allowed us to adjust plans accordingly and may have improved our ability to engage with participants.
Finally, based on participant responses in this co-design phase, some questions we are left with include the following:
We aim to develop a cultural safety framework and practice guide to be used by mental health services, but can a cultural safety framework be implemented in a system that is not currently culturally safe?
If the current system is based on historical models of exclusion rather than Aboriginal and Torres Strait Islander models of inclusion, can we have an inclusive system, within a system that was designed to exclude?
Are these juxtapositions that cannot be brought together? If not, how do we resolve this tension? What are the broader starting points to think about?
Perhaps changing systems means operationalising self-determination, through sharing equal power and decision-making in mental health services’ model of practice, for Aboriginal and Torres Strait Islander clients. We hope to learn answers to these questions through the next phases of this research project.
In conclusion, learnings from this co-design phase of the project have highlighted the importance of authentic community engagement and participatory action research, and have formed a solid foundation for the next phases of this project.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674241246444 – Supplemental material for Walking together in friendship: Learning about cultural safety in mainstream mental health services through Aboriginal Participatory Action Research
Supplemental material, sj-pdf-1-anp-10.1177_00048674241246444 for Walking together in friendship: Learning about cultural safety in mainstream mental health services through Aboriginal Participatory Action Research by Helen Milroy, Shraddha Kashyap, Jemma Collova, Michael Mitchell, Angela Ryder, Zacharia Cox, Mat Coleman, Michael Taran, Beatriz Cuesta Briand and Graham Gee in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-pdf-2-anp-10.1177_00048674241246444 – Supplemental material for Walking together in friendship: Learning about cultural safety in mainstream mental health services through Aboriginal Participatory Action Research
Supplemental material, sj-pdf-2-anp-10.1177_00048674241246444 for Walking together in friendship: Learning about cultural safety in mainstream mental health services through Aboriginal Participatory Action Research by Helen Milroy, Shraddha Kashyap, Jemma Collova, Michael Mitchell, Angela Ryder, Zacharia Cox, Mat Coleman, Michael Taran, Beatriz Cuesta Briand and Graham Gee in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the time and knowledges shared with the research team by Aboriginal and Torres Strait Islander community members.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Health and Medical Research Council, Million Minds Mission (MRFF; grant no. APP1178803).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.