
Abstract
Background:
Prevention and Recovery Care services are residential sub-acute services in Victoria, Australia, guided by a commitment to recovery-oriented practice. The evidence regarding the effectiveness of this service model is limited, largely relying on small, localised evaluations. This study involved a state-wide investigation into the personal recovery, perceived needs for care, well-being and quality-of-life outcomes experienced by Prevention and Recovery Care services’ consumers.
Methods:
A longitudinal cohort design examined the trajectory of self-reported personal recovery and other outcomes for consumers in 19 Victorian Prevention and Recovery Care services over 4 time points (T1 – 1 week after admission; T2 – within 1 week of discharge; T3 – 6 months after discharge; T4 – 12 months after discharge). T2–T4 time frames were extended by approximately 3 weeks due to recruitment challenges. The Questionnaire about the Process of Recovery was the primary outcome measure.
Results:
At T1, 298 consumers were recruited. By T4, 114 remained in the study. Participants scored higher on the Questionnaire about the Process of Recovery at all three time points after T1. There were also sustained improvements on all secondary outcome measures. Improvements were then sustained at each subsequent post-intervention time point. Community inclusion and having needs for care met also improved.
Conclusion:
The findings provide a consistent picture of benefits for consumers using Prevention and Recovery Care services, with significant improvement in personal recovery, quality of life, mental health and well-being following an admission to a Prevention and Recovery Care service. Further attention needs to be given to how to sustain the gains made through a Prevention and Recovery Care service admission in the long term.
Introduction
Recovery-oriented practice recognises that personal recovery is an individual journey towards living a meaningful life that maintains hope and purpose for every individual (World Health Organization, 2019). There is international support for enabling personal recovery-oriented service delivery, and emerging evidence about the effectiveness of recovery-oriented practice (Meadows et al., 2019).
Prevention and Recovery Care (PARC) services are residential sub-acute mental health services in Victoria, Australia. They are guided by a commitment to recovery-oriented practice at a state and national policy level (Commonwealth of Australia, 2013; Fletcher et al., 2019). Adult PARC services offer sub-acute residential support to consumers that lasts from a few days to up to 4 weeks (Fletcher et al., 2019; Harvey et al., 2019a). They involve a partnership between Mental Health Community Support Services (MHCSS) responsible for the delivery of 24-hour psychosocial support and clinical mental health service providers (Fletcher et al., 2019). PARC services attempt to provide a safe and comfortable environment for an average of 10 consumers per service (Fletcher et al., 2019; Galloway et al., 2016; Heyeres et al., 2018). Their aim is to prevent admissions to acute psychiatric units through what is known as ‘step-up’ admissions and to avoid re-admissions following an acute admission through a ‘step-down’ stay (Farhall et al., 2021; Galloway et al., 2016; Sutherland et al., 2020; Victorian Department of Health, 2010).
These services are well advanced in Victoria (Farhall et al., 2021), but implementation and service delivery has moved at a faster pace than the development of the evidence base (Fletcher et al., 2019). While PARC services are associated with improvements in recovery-related indicators and symptom-based measures (Forwood et al., 2008; Lee et al., 2014; Ngo et al., 2020), the evidence has previously relied on small, localised evaluations and has rarely considered comparison groups or long-term outcomes (Heyeres et al., 2018; Ngo et al., 2020; Siskind et al., 2013; Thomas et al., 2017). This paucity of evidence has led to calls for rigorous research to elucidate the models under which these services operate and their impacts on consumers and stakeholders (Parker et al., 2015).
Our ongoing research programme includes seven inter-related studies that provide complementary perspectives on PARC services. We have so far shown that Victorian PARC services are operating as intended (Fletcher et al., 2019; Harvey et al., 2019a). We have also found that the services were clustered into the three sub-types with significant differences in service characteristics such as the year in which the PARC service was opened, the living environment, proportion of admissions that were step-down from an inpatient unit and the regularity with which families were invited to care meetings (Harvey et al., 2019a). Analysis of routinely collected state-wide data found that consumers admitted to PARC services share many of the same characteristics as those admitted to inpatient units, but with some important differences such as gender balance and the diagnosis most commonly recorded (Sutherland et al., 2020). In another of our studies, Farhall et al. (2021) found PARC service consumers are significantly less likely to have an inpatient admission in the 365 days following the end of their index stay and also less likely to be on a Community Treatment Order (CTO) (Mental Health Act, 2014 [Vic]). Interview data from consumers who had experience of a stay in a PARC service indicated positive experiences but with some areas for improvement (Brophy et al., 2020).
The study reported here builds on our programme of research by investigating whether a cohort of consumers who use PARC services self-report improvements in personal recovery, perceived needs for care, well-being and quality of life over a 12-month period. An emphasis on these outcomes is an important component of addressing the effectiveness of Victoria’s PARC services.
Setting
As described by Fletcher et al. (2019), there were 20 adult PARC services offering 194 beds and 6-day places across Victoria as at January 2016. Nineteen of these were sub-acute services, including a women-only service. The other adult PARC service offered a 6-month extended stay service. This study included the 19 sub-acute adult PARC services. Twelve of these were in suburban areas, four were in regional areas and three were in inner-city areas. PARC service stays are voluntary, but people on a CTO under Victoria’s Mental Health Act (2014) can access these services (Fletcher et al., 2019; Harvey et al., 2019a).
Methods
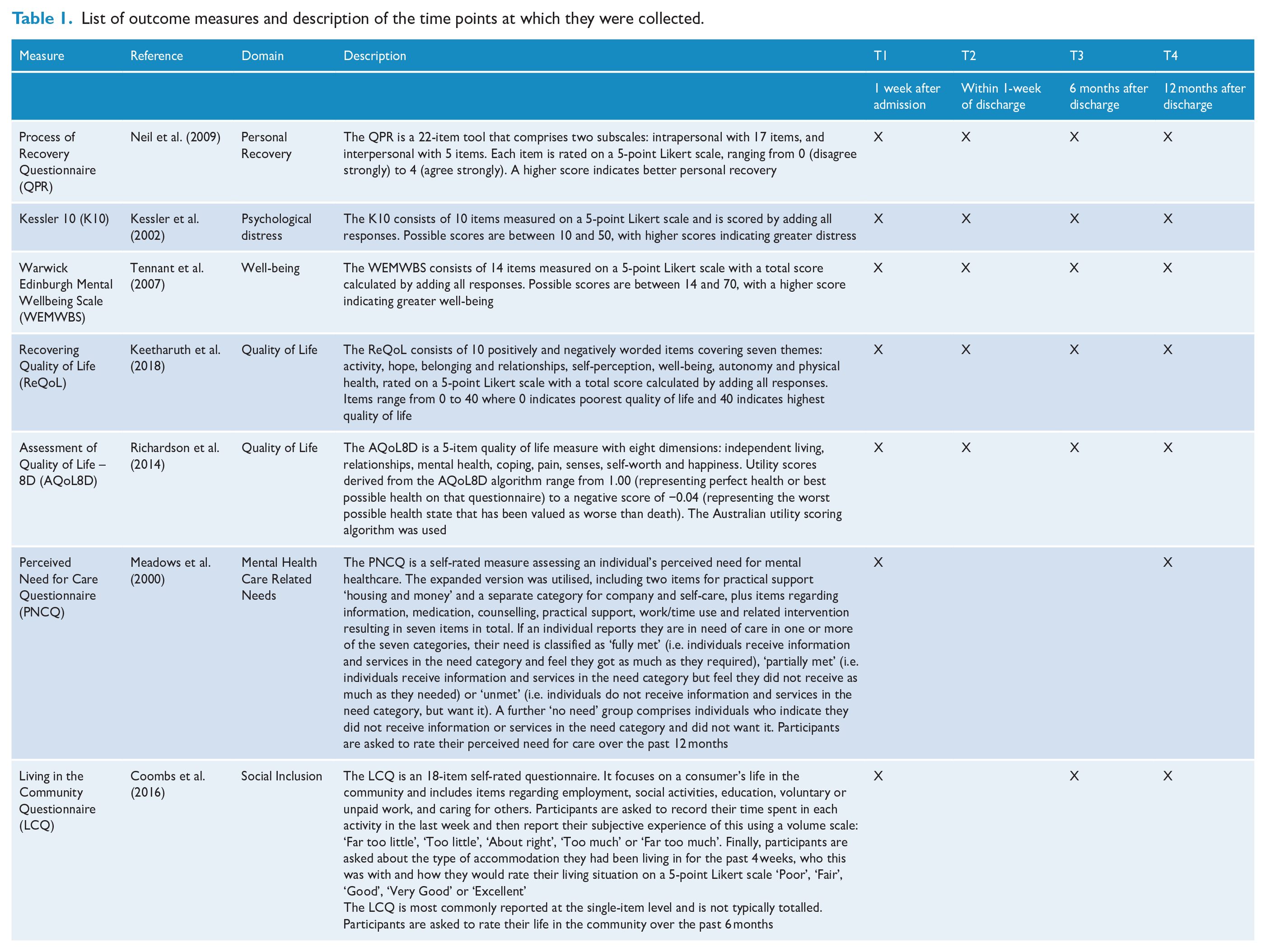
This study used a longitudinal cohort design with repeated measures to examine the trajectory of self-reported personal recovery and other outcomes for consumers who had a residential stay in a PARC service from May 2017 to April 2018. The last 12-month follow-up (T4) was conducted in May 2019. Researcher-facilitated surveys were conducted with these consumers at four time points. The survey questions assessed self-reported personal recovery, mental health, well-being and quality of life at all time points, and perceived needs for care at T1 and T4. Table 1 describes the time points and measures. Ethics approval was obtained via the Victorian Human Research Ethics Multi-site process (HREC/16/MonH/393) for each of the participating services.
List of outcome measures and description of the time points at which they were collected.
Consumer eligibility
We recruited consumers within 1 week of their admission to any of the 19 PARC services during the recruitment phase. Eligible consumers were aged 18 years or over, able to provide informed consent and had sufficient English proficiency to take part in the researcher-facilitated survey at T1. Participants were not eligible to join the study if they had been at the PARC service for longer than 1 week.
Procedures for recruitment
At T1, recruitment was conducted by a team that included consumer researchers (i.e. researchers with lived experience of mental distress and mental health service use). Consumer researchers were integral to the project team to enable a strong mix of skills and to enhance consumers’ comfort and trust in engagement and retention (Morrison and Stomski, 2015). Each researcher was responsible for a regional cluster of PARC services to maximise interview timeliness, minimise travel costs and enable relationship building and consistency. Recruitment relied on consumers opting into the study based on a convenience sampling approach. Each researcher regularly visited the allocated PARC service, introducing the study to staff and consumers at staff and community meetings. A flyer was also provided for display in communal areas. The researcher then returned to the PARC service to conduct the survey with consumers who told them they would like to participate.
T1 data were collected through a survey accessed by an iPad. While the participant operated the iPad and answered the structured survey, the researcher was on hand to answer queries as required. When requested by the participant, the researcher operated the iPad and asked the survey questions in the format of a structured interview. Following being sent the survey at T2, T3 and T4, participants were contacted by a consumer researcher and were asked to return the completed survey via post, email or over the telephone, based on their preference. A minority of participants were assisted by the consumer researcher over the telephone at T4 to complete the Perceived Need for Care Questionnaire (PNCQ) component of the survey due to its complexity. To acknowledge their contribution, each consumer received a $25 voucher after completing the T1 survey and $10 after completing the T2 surveys. Consumers received a $20 voucher on completion of the T3 and T4 surveys due to the longer time commitment.
Strategies to maximise retention and ongoing engagement at follow-up included telephone contacts by a consumer researcher to support and prompt completion of surveys at each time point; options for telephone, mailed or emailed survey completion; a regular project newsletter sent to participants to sustain interest in the study and to prompt communication with the project team regarding changes of contact details; and a catered engagement event for participants to meet the research team.
Information sought from participants
The primary outcome measure was the Questionnaire about the Process of Recovery (QPR) (Neil et al., 2009). Secondary outcome measures were the Kessler 10 (K10; Kessler et al., 2002), the Warwick Edinburgh Mental Wellbeing Scale (WEMWBS; Tennant et al., 2007), the Recovering Quality of Life (ReQoL; Keetharuth et al., 2018), the Assessment of Quality of Life–8D (AQol8D) (Richardson et al., 2014), the PNCQ (Meadows et al., 2000) and the Living in the Community Questionnaire (LCQ) (Coombs et al., 2016). These measures focused on psychological distress, social inclusion, mental health–related needs, well-being and quality of life. All measures are summarised in Table 1 (see Supplemental Appendix A for details).
Socio-demographic information was collected from participants at T1, including age, gender, country of birth, highest level of education completed, marital status, whether they had children, ethnicity and legal status.
In addition, participants were asked if they would consent to the researchers accessing their routine mental health service–related data from the Client Management Interface/Operational Datastore (CMI/ODS), an electronic data system for recording service use of individuals admitted to state-funded public mental health services in Victoria. These data were used to identify whether the participants’ PARC service stay at T1 could be classified as a ‘step-up’ or ‘step-down’ admission for each consumer who provided consent to access this information.
Statistical analysis
Survey data from the QPR, K10, WEMWBS, ReQoL, AQoL8D, LCQ and the PNCQ were analysed using STATA 15 (StataCorp, 2017) to observe patterns of change over time.
Patterns of missing data were examined to inform decisions on multiple imputation. This involved examining associations between missing values and demographic measures in addition to traditional tests of randomness.
Changes in scores on most of the measures (QPR, K10, WEMWBS, ReQoL and AQoL8D) were assessed over time using mixed-effects linear regression with random intercept effects to account for the repeated measures from individuals. Models were derived from the dataset with missing outcomes replaced by multiple imputations as described below. For each of these five outcome measures, we examined model outputs and means with 95% confidence intervals. Intervention effects were estimated from the models. Time point was included in the models as a categorical variable (T1, T2, T3, T4) to enable examination of short-term impacts of PARC services between T1 and T2 and long-term impacts between T1 and T3, and T1 and T4. Demographic variables (covariates) known to be related to mental health, such as gender, age, highest education level and marital status, were investigated for inclusion into the final multivariable model by conducting a series of univariate linear regressions with the full dataset involving each consumer demographic variable and the primary outcome. If p ⩽ 0.20, these variables were included in our final regression model as covariates. This p-value was chosen to minimise inadvertently excluding covariates that might show relationships in the final model. Covariates were modelled as fixed effects.
Subgroup secondary analysis (exploratory findings only)
Differences in longitudinal trend were analysed between genders, age groups and location to determine whether certain subgroups maintained progress made during their stay. Outcomes for subgroups of ‘step-up’ and ‘step-down’ participants were analysed when that could be confirmed. Subgroup analyses were investigated by repeating the analyses using an interaction term between time and group (‘step-up’/‘step-down’) in the main regression. If the interaction term produced a p-value < 0.1, then the subgroup analyses were conducted. The subgroup analyses compared the mean total scores for each outcome measure in the ‘step-up’ and ‘step-down’ subgroups. Due to possible under powering, these subgroup analyses were designated as exploratory only. Furthermore, we used the typology of Victorian PARC services to examine whether the regression results would be different if we specified that the PARC services were clustered into the three sub-types as we previously reported (Harvey et al., 2019a); however, there were no significant differences found.
Results
The results include data from 298 consumers at T1, 183 consumers at T2, 127 consumers at T3 and 114 consumers at T4. Forty-two participants were recruited from the 3 inner-city PARC services, 181 from the 12 suburban PARC services and 67 from the 4 regional PARC services.
Missing data and multiple imputation
There were 40–53% of values missing for key outcome variables (Supplemental Appendix B). Missing data were found to be associated with respondents’ highest level of education (completing high-school only associated with more missing data) and age (younger ages associated with more missing data); therefore, missing at random was assumed. Ten data imputations were generated using multivariate regression and strata of education (i.e. a dichotomised median split), time point (T1, T2, T3 and T4) and intervention status (pre = T1; post = T2–T4). Results from the observed dataset and the imputed dataset were compared to ensure the validity of imputation (Supplemental Appendix B). T2 data collection was originally planned to occur within 1 week of discharge from the PARC service, but difficulties in obtaining information about discharge dates and contacting participants post-stay meant that T2 data collection extended beyond 1-week post-discharge for most consumers. The mean (SD) days from discharge to T2 data collection was 22.97 (34.86). T3 data collection was originally planned for 6 months after discharge from the PARC service, and T4 data collection for 12 months after discharge. As with T2, T3 and T4 data collection extended beyond the planned time points due to challenges in locating participants and supporting them to complete and return the survey. Thus, the mean number of days between discharge and T3 was 204.07 (SD = 44.96), and between discharge and T4 was 391.04 (SD = 29.62); therefore, each time period for data collection was extended by approximately 3 weeks.
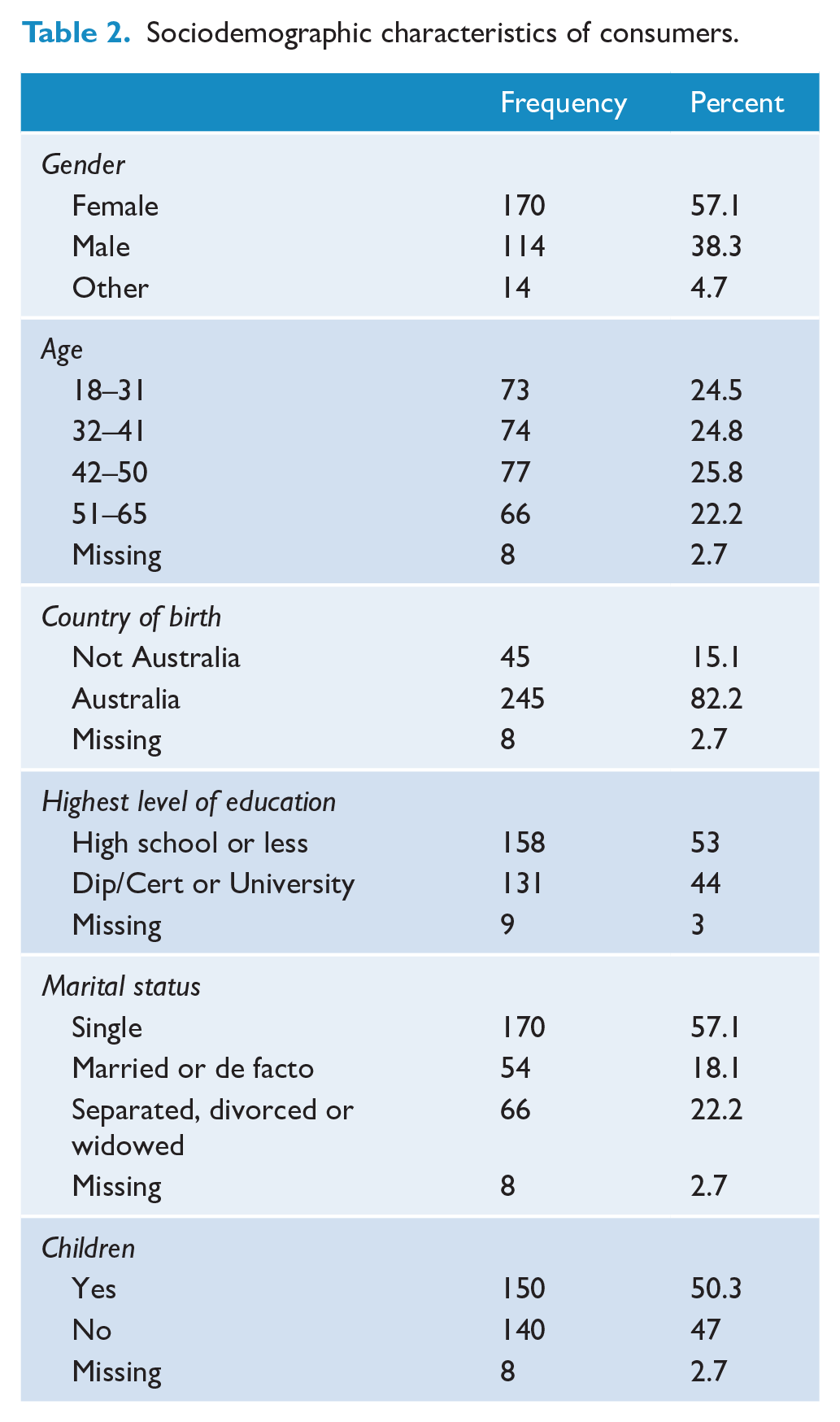
The sociodemographic characteristics of the 298 study participants are shown in Table 2.
Sociodemographic characteristics of consumers.
There were 72 (23.8%) participants who provided data on the primary outcome (QPR) at all four study time points: 97% (290/298) at T1, 61% (183/298) at T2, 42% (125/298) at T3 and 38% (113/298) at T4. See Supplemental Appendix B for frequency and percent of study participants with missing total scores at each time point for all outcome measures.
Table 3 shows the model adjusted mean scores for the primary and secondary outcomes with 95% confidence intervals. The mean QPR score showed significant improvement at all later time points compared with T1. The greatest increase occurred from T1 to T2. Scores were trending back towards T1 at the two subsequent time points. K10 scores significantly improved from T1 to all later time points, indicating decreased distress among participants at T2, with improvement at both T3 and T4. WEMWBS, ReQoL and AQoL8D scores significantly improved from T1 to T2. The improved scores for these measures were then sustained at each subsequent post-intervention time point (Supplemental Appendix C). Figure 1 shows the descriptive trends for each of the outcome variables. Averaged across all measures, T1 to T2 revealed a mean improvement of d = 1.79 with the trend reversing from T2 to T3, d = −0.05, and a small mean improvement evident from T3 to T4, d = 0.23 (Supplemental Appendix D).
Model adjusted means calculated from the mixed effects linear model, for the QPR, K10, WEMBMS, ReQoL and AQoL8D.
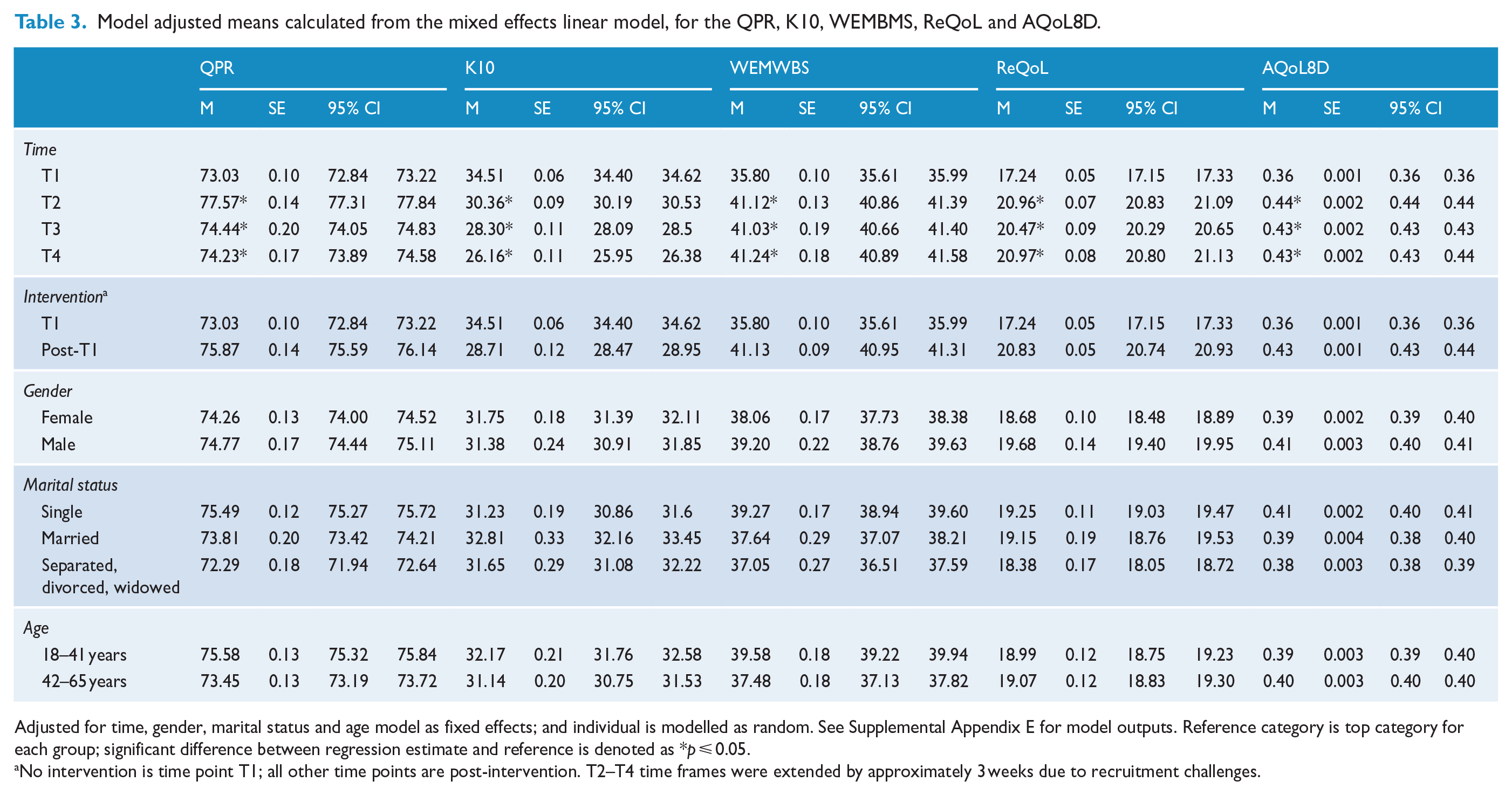
Adjusted for time, gender, marital status and age model as fixed effects; and individual is modelled as random. See Supplemental Appendix E for model outputs. Reference category is top category for each group; significant difference between regression estimate and reference is denoted as *p ⩽ 0.05.
No intervention is time point T1; all other time points are post-intervention. T2–T4 time frames were extended by approximately 3 weeks due to recruitment challenges.

Mean trajectory with standard error of outcome measures over time points.
We examined consumers’ self-reported perceived need across the seven categories of the PNCQ at T1 and T4 (Supplemental Appendix E). We did not ask participants to complete the PNCQ at T2 and T3 because it required participants to identify their needs over the last 12 months. At T1, the least commonly reported perceived need was for ‘practical support’ and the most commonly reported need was for ‘medicines’, which was also rated as the most commonly met need, whereas the ‘work and time-use’ category was reported as the least met need. At T4, consumers indicated that their perceived need for ‘work and time use’ was their least commonly reported need and the most commonly reported need remained ‘medicines’, which was also rated as the highest met need, whereas the ‘self-care’ category was reported as the least commonly met need. In addition, fewer consumers reported wholly unmet need at T4 as compared with T1. Partially met needs also consistently trended downwards across time.
All changes to the PNCQ proportion of met need were in a positive direction; a greater proportion of consumers reported that their needs were met at T4 as compared with T1, which covered the year prior to entry into the study (Figure 2). The greatest positive change was observed for the practical support need category.
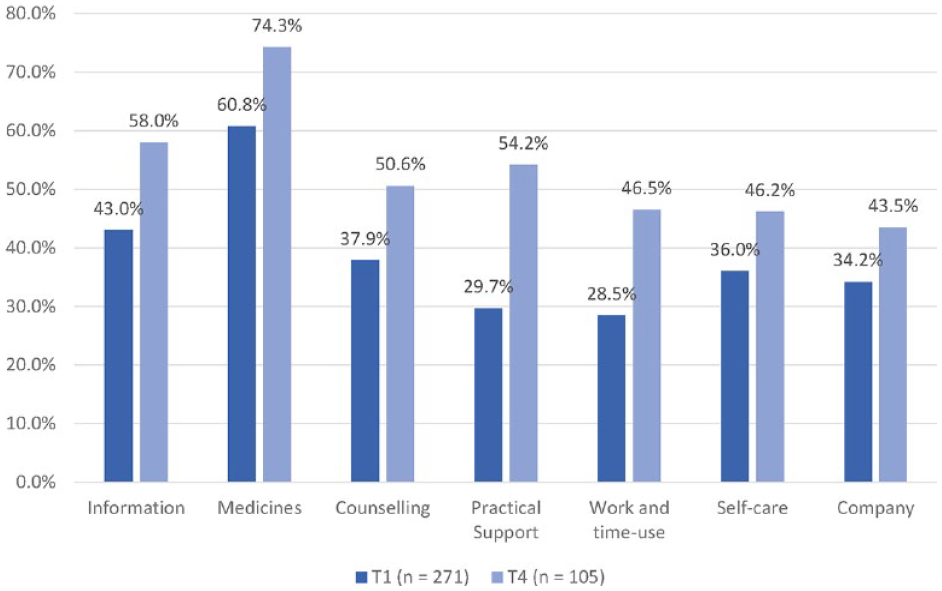
Proportion of met needs from T1 to T4 (PNCQ; calculated as met needs/(unmet needs + partially met needs + met needs).
Frequency analysis for six areas of social inclusion on the LCQ for T1, T3 and T4 are presented graphically in Figure 3 (with a detailed frequency table in Supplemental Appendix F). At T4, 65% of participants rated their living situation in the previous 4 weeks as being ‘good’, ‘very good’ or ‘excellent’ compared with 55% at T1. Similarly, 55% participants reported their socialising was about right at T4 compared with about 40% at T1. In one domain (employment), there was an inconsistent pattern of improvement over time. More than 50% of participants reported too little time in employment at T3, whereas at T1 and T4, a larger percentage (approximately 60%) of participants were reporting about the right time in employment. Too few participants completed the questions about ‘caring for others’, ‘voluntary and unpaid work’ and ‘education’ to make any meaningful inferences.
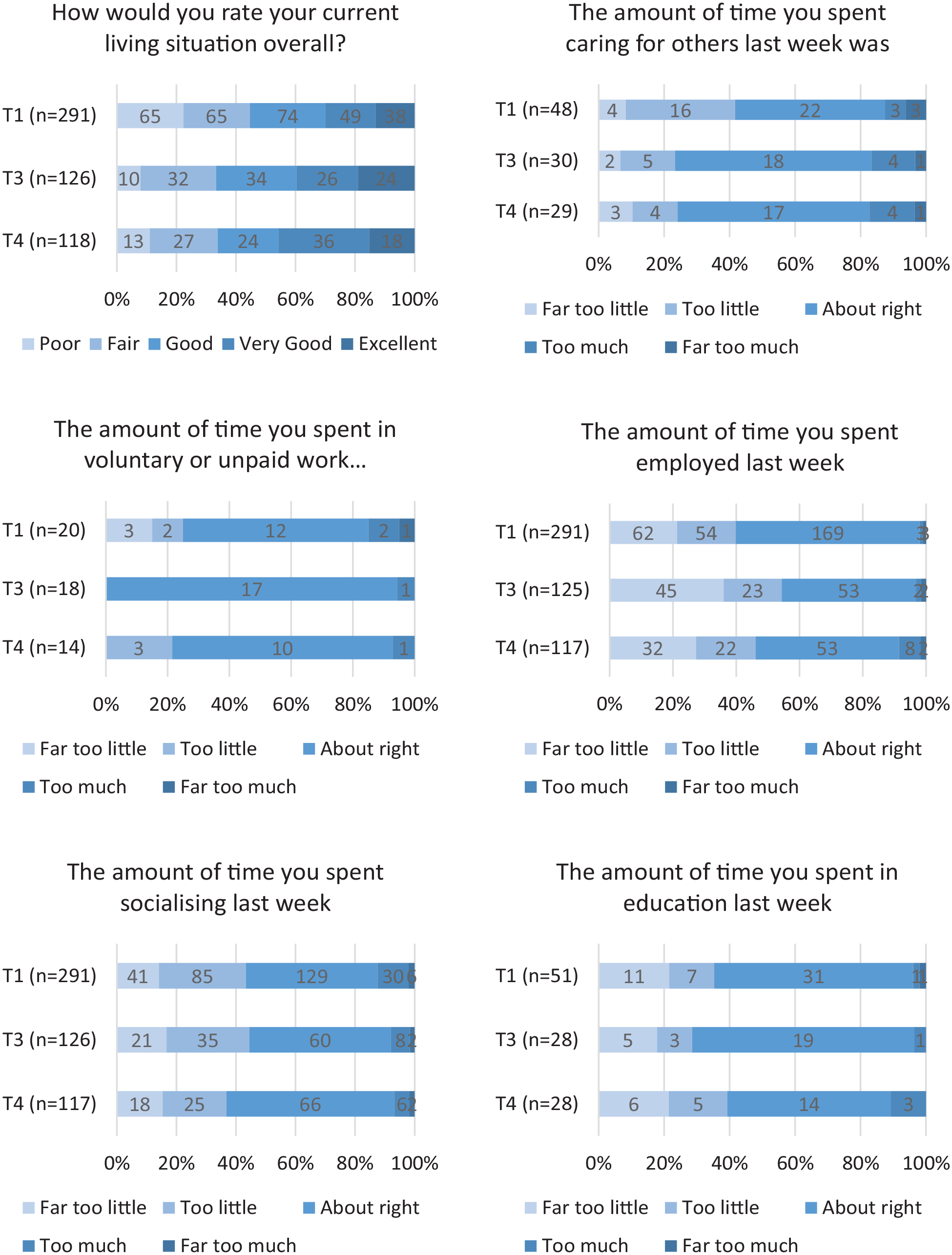
Responses to living in the community questionnaire over time.
‘Step-up’ and ‘step-down’ comparison and subgroup analysis
A total of 233 participants (80.3%) consented to have their CMI data linked to their survey data. Of this group, 96 participants were categorised as having had a ‘step-down’ stay in a PARC service and 137 participants were categorised as having had a ‘step-up’ stay.
In the total sample and the ‘step-up’ sample, the mean total score for the QPR increased significantly between T1 and T2, and T1 and T4, but not between T1 and T3. In the ‘step-down’ sample, no significant change was evident between T1 and any other time point.
Discussion
The findings reported here show benefits for consumers of a stay in PARC services with consistent evidence of significant improvement in personal recovery, quality of life, mental health and well-being over a subsequent 12-month period.
In relation to this study’s primary outcome measure, the QPR, the overall trend was significant personal recovery gains between the stay at the PARC service and post exit. We noted that these gains were difficult to sustain, particularly at the 6-month follow-up time point, but at 12 months the mean scores were still higher than at admission to the PARC; however, QPR scores indicated consumers having a ‘step-up’ stay were more likely to experience gains in personal recovery during their time at the PARC service compared with the step-down subgroup. Both subgroups shared similar scores on exiting the PARC service despite ‘step-up’ consumers reporting lower QPR scores on entry. The ‘step-down’ group indicated stable recovery scores from T1 to T2, perhaps suggesting that the PARC service supported them to sustain any gains made on the inpatient unit; however, it appears that for both groups recovery gains were difficult to sustain. This pattern suggests recovery-related outcomes, such as connectedness, hope, identity, meaning and purpose, and empowerment (Leamy et al., 2011), are enhanced during a PARC service stay but may not endure over time. While the ‘step-down’ group appeared to revert to below baseline levels, the ‘step-up’ group appeared to slip back after 12 months with very similar scores being noted between the groups 12 months after leaving the PARC service.
In other studies investigating the impact of PARC type services, the K10 has been used as an outcome measure. The results for the K10 in this study indicate a reduction from very high to high levels of psychological distress. Ngo et al. (2020) and Thomas et al. (2017) found improvements similar in the K10 from baseline to exiting the service. By comparison, the strength of our study is in the size of the follow-up cohort and the findings regarding whether the gains on the K10 made at PARC services are sustained over a 12-month period. At the descriptive level (see Supplemental Appendix G), gains were made on the K-10 following both ‘step-up’ and ‘step-down’ admissions; however, unlike a smaller study of a single service elsewhere in Australia (Thomas et al., 2017), there was no evidence to suggest greater gains were made by ‘step-up’ participants.
Scores on all measures apart from the K-10 indicate that some gains ‘plateau’ within 6–12 months after being discharged from a PARC service. Significant differences were not found in outcomes between people in relation to age, gender or marital status.
Positive outcomes were also indicated by the PNCQ. The results suggest that following a stay in a PARC service, a greater proportion of consumers perceive their needs to have been met. Consumers also assess the provision of services as more adequate in the period between T1 and 12 months later at T4. Potentially, a PARC services stay facilitated access to improved opportunities to have their needs met. The PNCQ results suggest perceived needs for medication are by far the most consistently met of consumers’ identified needs in these services (Harvey et al., 2019b; Morgan et al., 2017). Nevertheless, one in four reported an inadequately met need for medication, which is consistent with previously reported survey findings by Morgan et al. (2017), in which the vast majority of people living with psychoses were taking medication but also indicated their treatment with medication was suboptimal. Similarly, the pattern of unmet needs in our study is very similar to other findings about people living with psychosis (Migliorini et al., 2022). PNCQ results indicate that other perceived psychosocial needs are not adequately addressed over time in the specific areas of social connection (company), self-care, and work and time use. This contrasts with unmet needs for practical support decreasing by a greater proportion between T1 and T4. This finding is consistent with the long-term outcomes identified in the QPR. Possibly, without being able to adequately meet needs in relation to work and time use and company, consolidating and extending gains in personal recovery may be limited, even though needs for social interventions, including practical support, are increasingly being met and there is a reduction in psychological distress. It is noteworthy that 12 months post a PARC service stay, the lowest total score for met need was that of company. It appears that social isolation and loneliness may be a key factor that needs to be addressed and might account for the lack of consolidation or, in the case of the QPR in particular, a decline in outcomes.
The apparent focus on meeting medication needs is consistent with recent findings from a Royal Commission into Victoria’s Mental Health System. The Royal Commission described Victoria’s mental health system as having an over-reliance on medication, in part due to the under resourcing and lack of focus on therapeutic interventions and recovery-centred treatment, care and support (State of Victoria, 2021). The Royal Commission called for more recovery-oriented care and it appears that PARC services are supporting this aspiration, as indicated by the QPR findings.
Strengths
This study involved consumer researchers who assisted with recruitment of a sizable number of people who were PARC service consumers. Outcomes were self-reported and did not rely on administrative data or service providers’ assessment of change (Ngo et al., 2020; Thomas et al., 2017). We were able to follow consumers for a 12-month period and therefore looked at outcomes over an extended period, and although this study had high attrition often expected in these studies (Homman et al., 2021), the size of our initial cohort did partly compensate for this. Finally, our efforts to keep people engaged ensured a relatively large sample of participants across the four time points.
Limitations
We did not have a control group and therefore could not make comparisons with non-PARC service users. This represents an opportunity for future research, potentially adopting a stepped-wedge randomised controlled trial (RCT) design such as that conducted in the Principles Unite Local Services Assisting Recovery (PULSAR) study (Meadows et al., 2019). We also experienced high levels of missing data, although our analysis attempted to reduce the impact of missing data by imputing missing values across all time points. We lacked information about the proportion of eligible consumers who consented to participate during the recruitment period and we also relied on a convenience sample that may not have been representative of the PARC service user population, despite some evidence to the contrary (e.g. Sutherland et al., 2020). In comparing our participants to Sutherland et al.’s (2020) large cohort study, we identified a similar proportion of males and females and age distribution, with the highest proportion of participants in the 32- to 50-year-old age group.
Conclusion
This study reports positive outcomes associated with an admission to Victoria’s PARC services in relation to personal recovery, well-being and psychological distress, especially post-discharge. We found that the greatest personal recovery gains were evident for people who were admitted directly from the community (i.e. step-up) rather than those whose stay followed an inpatient admission (i.e. step-down). The findings suggest further attention needs to be given to how to sustain the gains made through a PARC service admission over time. Further exploration into whether consumers are supported in an ongoing way in community care post a PARC service stay is needed. Gains are likely to be impacted by factors including opportunities for social inclusion and ongoing access to recovery-oriented services in the community (State of Victoria, 2021). The findings provide support for the continued expansion of sub-acute services offering residential treatment and support.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241242943 – Supplemental material for A longitudinal study of the impacts of a stay in a Prevention and Recovery Care service in Victoria, Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674241242943 for A longitudinal study of the impacts of a stay in a Prevention and Recovery Care service in Victoria, Australia by Lisa Brophy, Justine Fletcher, Shrinkhala Dawadi, John Reece, Vrinda Edan, Joanne Enticott, John Farhall, Ellie Fossey, Bridget Hamilton, Carol Harvey, Graham Meadows, Cathrine Mihalopoulos, Emma Morrisroe, Richard Newton, Victoria Palmer, Ruth Vine, Shifra Waks and Jane Pirkis in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We acknowledge and thank the consumers, carers and family members, and mental health professionals who have participated in the project along with the Lived Experience Advisory Panel, Clinical Services Advisory Group and national and international advisors. This investigation was conducted by a team of researchers working alongside partner investigators from the Victorian Department of Health and Human Services and all the MHCSS involved in providing PARC services in Victoria at the time of the study: Break Thru, Ermha, Life Without Barriers, Cohealth, Wellways, Mind Australia Limited and Neami National. Our thanks to Greta Baumgartel, Simon Jones, Michelle Kehoe, Rosemary Callander, Tess Hall, Anastasia Ossukhova, Elizabeth Vercoe, Francesca Kupperman and Maria Katergaris for providing research assistance across the life of the project.
Author’s Note
Graham Meadows is now affiliated to Centre for Mental Health and Community Wellbeing, Melbourne School of Population and Global Health, The University of Melbourne, Melbourne, VIC, Australia; Monash Centre for Health Research and Implementation, Monash University, Melbourne, VIC, Australia; Department of Psychiatry, Monash University, Melbourne, VIC, Australia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This publication is based on data collected in the Building the Evidence Base for Prevention and Recovery Care (PARC) Services project. The project was funded by an NHMRC partnership grant (GNT1115907) in a partnership between academic institutions, Mental Health Community Support Services (MHCSS), clinical or area mental health service providers and the Victorian Government.
Ethics Approval and Consent to Participate
Ethical approval for the project was granted from Monash Health, our primary Human Research Ethics Committee (HREC/16/MonH/393). Governance approval was also required from all health services involved. In total, governance approval from 13 health services was obtained to allow us to collect data from 19 adult PARC services around Victoria. We also sought and received ethical approval from each partner organisation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.