
Abstract

To the Editor
Australia’s suicide rates have been largely unchanged for decades, despite multiple suicide prevention strategies, several national mental health plans, new mood disorder–specific national organisations (e.g. Beyond Blue) and rising antidepressant use (Jorm, 2019). The National Suicide Prevention Trial (NSPT) (2016–2021) was the latest such trial, funded by the Australian Government (Page et al., 2023). Conducted over 12 regional sites across Australia, its aim was to develop individualised suicide prevention strategies targeting specific at-risk demographic groups.
Page et al. (2023) evaluated the effectiveness of this trial by comparing both suicide rates and self-harm hospitalisation rates following the implementation of the NSPT, comparing these rates with control regions. This study identified no significant reduction in suicide rates (relative risk = 0.98, 95% confidence interval [CI] = [0.91, 1.06]) in the intervention group compared to control sites, with similar findings for self-harm–related hospitalisations (relative risk = 0.99, 95% CI = [0.96, 1.02]).
In examining the lack of impact of suicide prevention strategies in Australia, Jorm (2019) concluded that there was likely a role for considering broader social factors beyond clinical services for reducing Australia’s suicide rates. Jorm’s (2019) conclusion compels consideration of the role of social factors beyond clinical services for reducing suicide rates. This is further supported by the finding that suicide rates in the lowest quintile socioeconomic areas have increased between 2010 and 2021 by 41%, from 13 to 18.4 per 100,000 population (see Figure 1), with the second lowest quintile also increasing by 13% from 11.9 to 13.5 per 100,000 population (Australian Institute of Health and Welfare [AIHW], 2022). This contrasts with the relative stability of suicide rates in quintiles 3 and 4 and reduction of suicide rates in quintile 5 (16%) for the same time period (AIHW, 2022). Of note (Figure 1), the suicide rate ratio between quintile 1 and quintile 5 has grown markedly from 1.4 to 2.3 times difference.
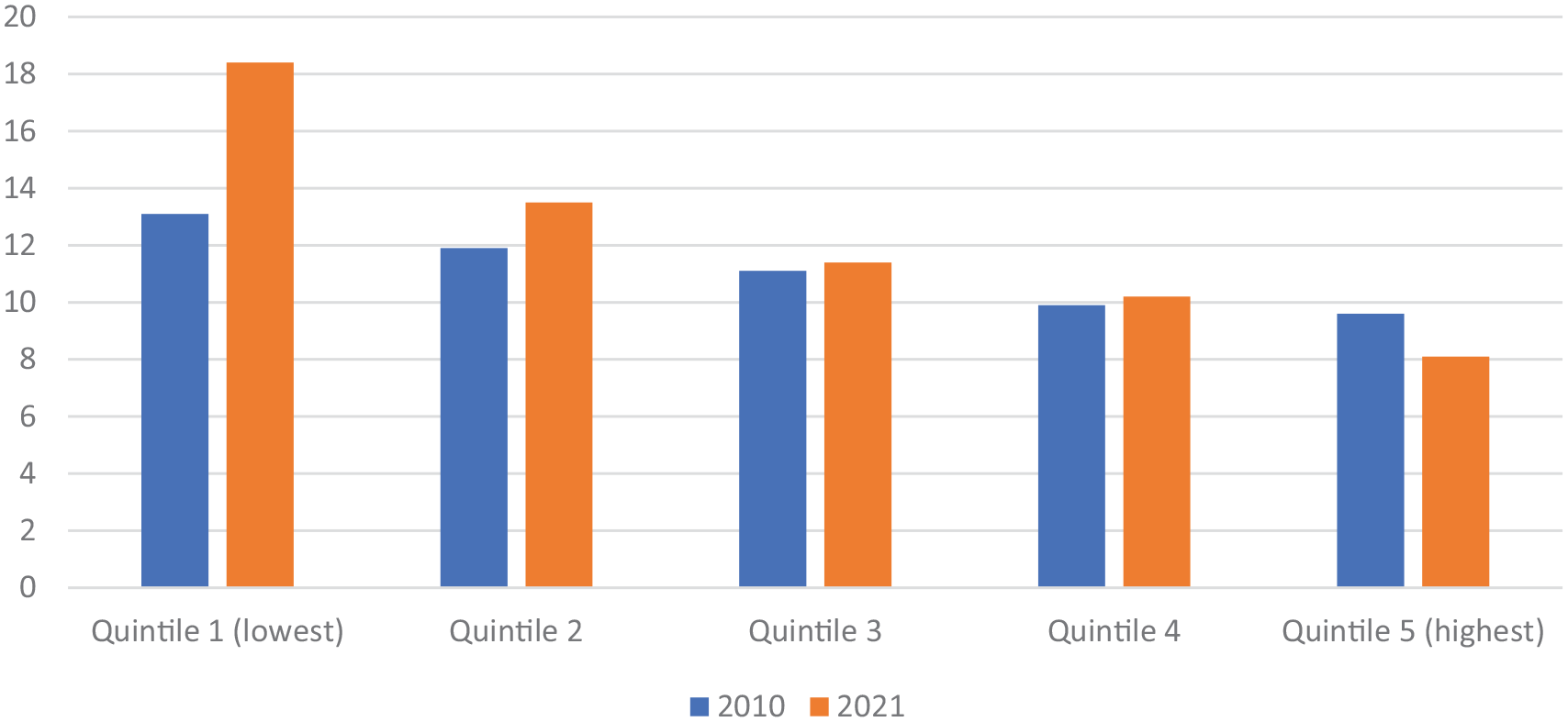
Suicide rates per 100,000 population in Australia by socioeconomic status region.
Durkheim’s classical perspective identified the importance of social integration and social connectedness in reducing suicide rates at the population level (Durkheim, 2006). Social integration has both micro- and macro-components (Zimmerman, 2002), where microlevels involve personal relationships and social support that they can avail during stressful life events, while macrolevels involve the bonds an individual has to the wider society. Herein, we argue that higher levels of welfare support for the lowest socioeconomic status (SES) groups could result in greater social integration by reducing relative inequality and therefore reduce Australian suicide rates in this vulnerable population group and related regions.
Zimmerman (2002) identified that increases in US state-level per capita expenditure (between 1960 and 1995) on public welfare support correlated with decreases in state-level suicide rates, while adjusting for divorce rates, population change rates, unemployment rates, population density, racial composition and sex ratios. Norstrom and Gronqvist (2015) identified across 30 countries that, during significant economic recessions, countries with more equitable unemployment protection programmes experienced relative stability of suicide rates compared to countries with less equitable programmes.
Maslow’s psychological paradigm reminds us that fulfilment of basic needs facilitates capacity to satisfy higher emotional needs such as fostering close interpersonal relationships. Therefore, greater welfare support may not only increase microlevels of social integration by fortifying personal relationships but also increase macrolevels of social integration, because policies such as access to universal healthcare, childcare, sufficient unemployment protections and active labour market programmes allow individuals opportunities to meaningfully participate and maintain sense of connection with the wider society.
Zimmerman argues that suicide may not just be a public health or social problem; it might also be a political problem (Zimmerman, 2002). The need for enhanced welfare support and increases to the minimum wage received extensive advocacy prior to the latest Australian government budget release. The government responded with modest increases to unemployment benefits, rental assistance and enhanced bulkbilling incentives for primary healthcare and supported increases to the minimum wage (The Commonwealth of Australia, 2023). It is our view that enhanced welfare support and increases to the minimum wage for the lowest quintile SES will likely have population-level impact on lowering suicide rates in low SES populations and the regions in which they live, as enhanced welfare support may improve social integration among low SES populations in Australia. It is important to note that being employed significantly reduces suicide risk (Norstrom and Gronqvist, 2015). Therefore, this increased welfare support will need to be accompanied by active labour market policies that provide job training and incentives to be employed. It is also likely that other personal and society wide benefits will result from providing additional welfare support in deprived neighbourhoods.
It would be important for further research to evaluate the effects of specific welfare policies on Australian suicide rates at a regional level and compare these with similar countries providing differing levels of welfare support. The results of the NSPT prompt us to reflect on the value of nationwide implementation of such trials. Public policy which specifically addresses and targets relative socioeconomic disadvantage may have more impact on reducing suicide rates compared with current localised approaches to suicide prevention in Australia. Cost–benefit analysis of increasing welfare support, including an analysis of health and mental health outcomes, crime rates, educational and vocational outcomes, would be important. Such analysis will guide optimal welfare policies to improve a range of outcomes particularly in socioeconomically deprived neighbourhoods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.