
Abstract
Objective:
To explore the views of psychiatrists (including trainees) regarding the current state and future direction of specialist mental health and addictions services in Aotearoa New Zealand.
Methods:
Psychiatrists and trainee psychiatrists (registrars) in Aotearoa New Zealand were surveyed in August 2021. Of 879 eligible doctors, 540 participated (83% qualified and 17% trainee psychiatrists), a response rate of over 60%. Data were analysed quantitatively and with content analysis.
Results:
Psychiatrists thought specialist mental health and addictions services had been neglected during recent reforms, with 94% believing current resourcing was insufficient, and only 3% considering future planning was heading in the right direction. The demand and complexity of on-call work had markedly increased in the preceding 2 years. Ninety-eight percent reported that people needing specialist treatment were often (85%) or sometimes (13%) unable to access the right care due to resourcing constraints. The pressures were similar across sub-specialties. A key theme was the distress (sometimes termed ‘moral injury’) experienced by psychiatrists unable to provide adequate care due to resource limitations, ‘knowing what would be a good thing to do and being unable to do it . . . is soul destroying’. Recommendations were made for addressing workforce, service design and wider issues.
Conclusion:
Most psychiatrists in Aotearoa New Zealand believe the mental health system is not currently fit for purpose and that it is not heading in the right direction. Remedies include urgently addressing identified staffing challenges and boosting designated funding to adequately care for the 5% of New Zealanders with severe mental health and addiction needs.
Introduction
Despite aspirational policy statements (e.g. United Nations General Assembly, 2007), access to mental health care remains variable and mental health conditions persist as the leading cause of global disability (World Health Organization, 2022). Australia and Aotearoa New Zealand’s rates of mental health-associated disability sit among the highest in the world (Global Burden of Disease Mental Disorders Collaborators, 2022). This has obvious human costs but also confers a heavy financial burden, with serious mental health and addiction issues costing an estimated $12 billion a year in New Zealand alone (New Zealand Ministry of Health, 2017).
The escalating demand for mental health care shows little sign of slowing down. The number of individuals seen by the specialist mental health services and non-government organisations ‘ring-fence’ funded to serve the ‘top 3%’ or those with moderate-to-severe needs (New Zealand Government, 2018a) increased by approximately 40% between 2010 and 2020 (Association of Salaried Medical Specialists, 2021b). This jump in demand has been attributed to an increasing population and improvements in data capture, as well as the increased incidence and awareness of mental health issues (New Zealand Ministry of Health, 2019). The rising demand for mental health support has put considerable pressure on the health system and beyond (Office of the Health and Disability Commissioner, 2018). Meanwhile, New Zealanders have struggled with accessing appropriate and timely mental health services, with long waits to access treatments while their mental health deteriorates (New Zealand Government, 2018b). At a time when mental health presentations were already increasing, the situation has been complicated by the effects of the COVID-19 pandemic, which disproportionately affected vulnerable groups, including people with recognised mental conditions, young people and essential workers (Bell et al., 2021, 2022; Every-Palmer et al., 2020).
Improving mental health service provision in New Zealand has been a key focus for the Government in recent years. In 2018, the final report of the Government Inquiry into Mental Health and Addiction, He Ara Oranga, made a number of recommendations, with a particular focus on prevention and early intervention and expanding access to the 20% of the population who experience mild-to-moderate mental health issues (New Zealand Government, 2018b). A major recommended strategy was a shift from ‘Big Psychiatry’ to a less medically driven ‘Big Community’. ‘This is all very well as far as it goes’ explained Mulder and colleagues, ‘but runs into a major flaw: “big” psychiatry in New Zealand is actually rather small’ (Mulder et al., 2022). Specifically, they pointed to New Zealand’s comparatively low number of psychiatric beds per capita; in 2020, New Zealand had 32 beds per 100,000 people, compared to the Organisation for Economic Cooperation and Development (OECD) average of 65 beds. In addition, the country has for many years had the lowest number of psychiatrists per capita compared with 10 other similar countries including the United Kingdom, Australia and Canada (Association of Salaried Medical Specialists, 2021b). Mulder et al. (2022) concluded, ‘it would have been more accurate for the [He Ara Oranga] Report to have used the term “Small Psychiatry”, which would have helped explain the problems facing the public sector’.
Following publication, the He Ara Oranga report received some criticism from mental health experts for a perceived comparative neglect of the needs of those with serious mental illness and the resourcing of specialist mental health and addiction services (Allison et al., 2019; Royal Australian and New Zealand College of Psychiatrists, 2019). However, He Ara Oranga was hopeful that ‘demand for specialist services will reduce as issues are dealt with earlier, before they escalate . . .’ (New Zealand Government, 2018b). To date, this optimistic prediction does not seem to have transpired. As 2021 Committee members of Tu Te Akaaka Roa (the New Zealand committee of the Royal Australian and New Zealand College of Psychiatrists [RANZCP]), the authors of this paper were receiving increasing reports from members concerned about demand, resourcing and workforce shortages in their areas. With increasing access problems and expanding wait times for specialist mental health and addiction services also being reported in the media (Meier and Lourens, 2021), we considered it timely to canvas the experiences of the frontline psychiatry workforce in a systematic way.
Aim
The aim of this study was to collect data from psychiatrists regarding their views about the state of mental health services in New Zealand. The targeted domains for inclusion were a follow:
The configuration and funding of the mental health and addiction system
The resourcing of inpatient and secondary mental health and addiction services
The acuity and complexity of mental health and addiction presentations
The changes in the last 2 years in mental health and addiction services
What was working well in the mental health and addiction system
What changes, if any, participants would recommend.
Method
The study was approved by the University of Otago Human Ethics Committee (reference D21/230). The survey was fielded from 27 July to 24 August 2021. The sampling frame was all clinicians practising psychiatry in New Zealand either as vocationally registered psychiatrists, provisionally vocationally registered psychiatrists or psychiatry trainees (registrars). Both members and non-members of the RANZCP were eligible to participate. There were around 870 eligible people within the eligible population.
A cross-sectional survey design was used. The survey was designed to be brief, so to encourage participation and to ensure compatibility across media platforms. The content was refined using the ‘group mind’ process, with 10 colleagues iteratively testing and rigorously critiquing pilot versions, with successive improvements made based on their comments (Bradburn et al., 2004).
The Survey Monkey® questionnaire was distributed by email (from the RANZCP’s mailing list) and took approximately 13 minutes to complete. After viewing the information sheet, consenting to participate and successfully completing the eligibility questions, participants then anonymously answered questions about their experiences of mental health services in New Zealand. Demographic information collected included age, gender (male, female, gender diverse), area of specialisation, years of experience and ethnicity. Additional free text boxes were provided. Please see Supplementary File 1 for the survey questions.
Analysis
Numerical data were quantitatively analysed using Microsoft Excel® software. Percentages reported represent the response to each question and not the total number of participants (participants could skip questions and a small number of participants did not respond to every question). For measures where the absolute numbers are low, these were not broken down by other demographic variables. Free text data were analysed using manifest and latent content analysis (Hsieh and Shannon, 2005). Content analysis can capture the meanings within data, including data from questionnaires and involves establishing categories and identifying the frequency by which they occur (Crowe et al., 2015).
Data were analysed in the first instance by M.L.G. and S.E-.P. To enhance trustworthiness, key ideas and themes were shared and developed through successive iterations of the manuscript with co-authors (H.T., O.H., M.L., M.J. and S.R.). In terms of positionality, all authors were affiliated with the RANZCP. M.L.G. was a policy analyst, and all other authors were psychiatry members of Tu Te Akaaka Roa, the New Zealand committee of the RANZCP.
Results
There were 540 responses in total, representing a response rate of approximately 61%, and 90% of participants completed the whole survey. Eighty-nine participants (17%) were still training as psychiatrists (psychiatry registrars/residents). Participant demographics are summarised in Table 1. The sample was generally representative of New Zealand vocationally registered psychiatrists (46.4% of the RANZCP membership in New Zealand are female and 4.4% identify as Māori). However, there was relative underrepresentation of trainees, with 17.1% of participants being registrars compared with 26.5% of the New Zealand RANZCP membership.
Demographics of participants.
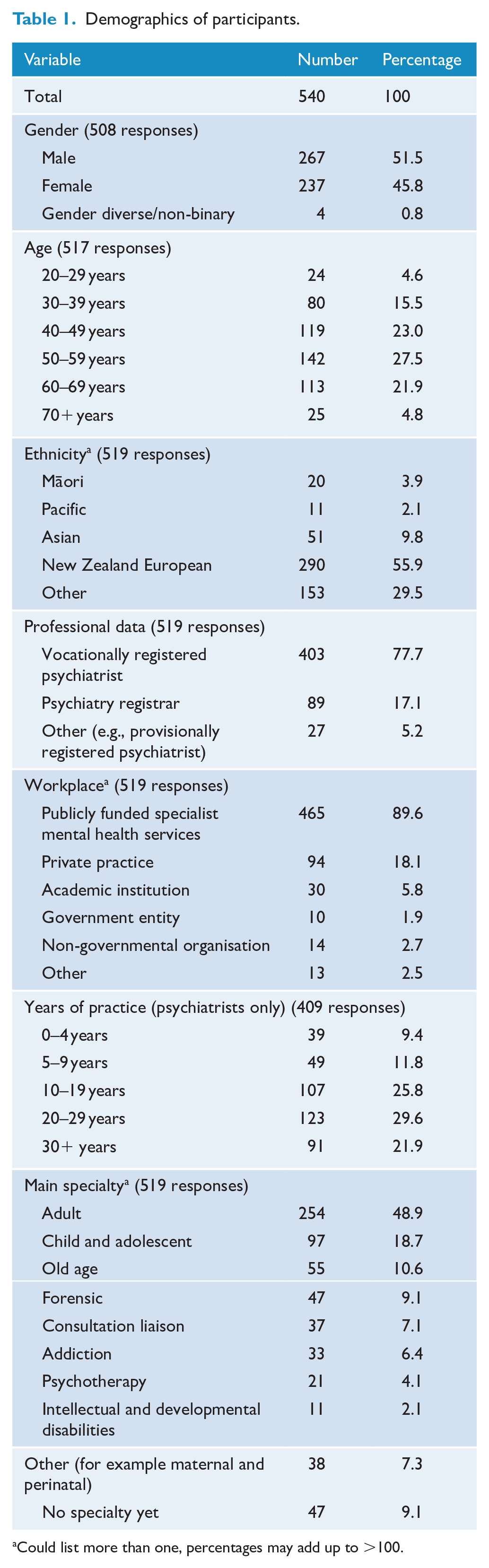
Could list more than one, percentages may add up to >100.
Participants were asked for their views on the current state and direction of the mental health and addiction system. Results are summarised in Table 2. A clear majority (82%) said that the configuration was currently not fit for purpose, and a similar proportion (88%) said that funding was not fit for purpose. A majority disagreed that the system was ‘heading in the right direction’ (71% in relation to configuration and 75% in relation to funding).
Frequency of agreement to survey questions.
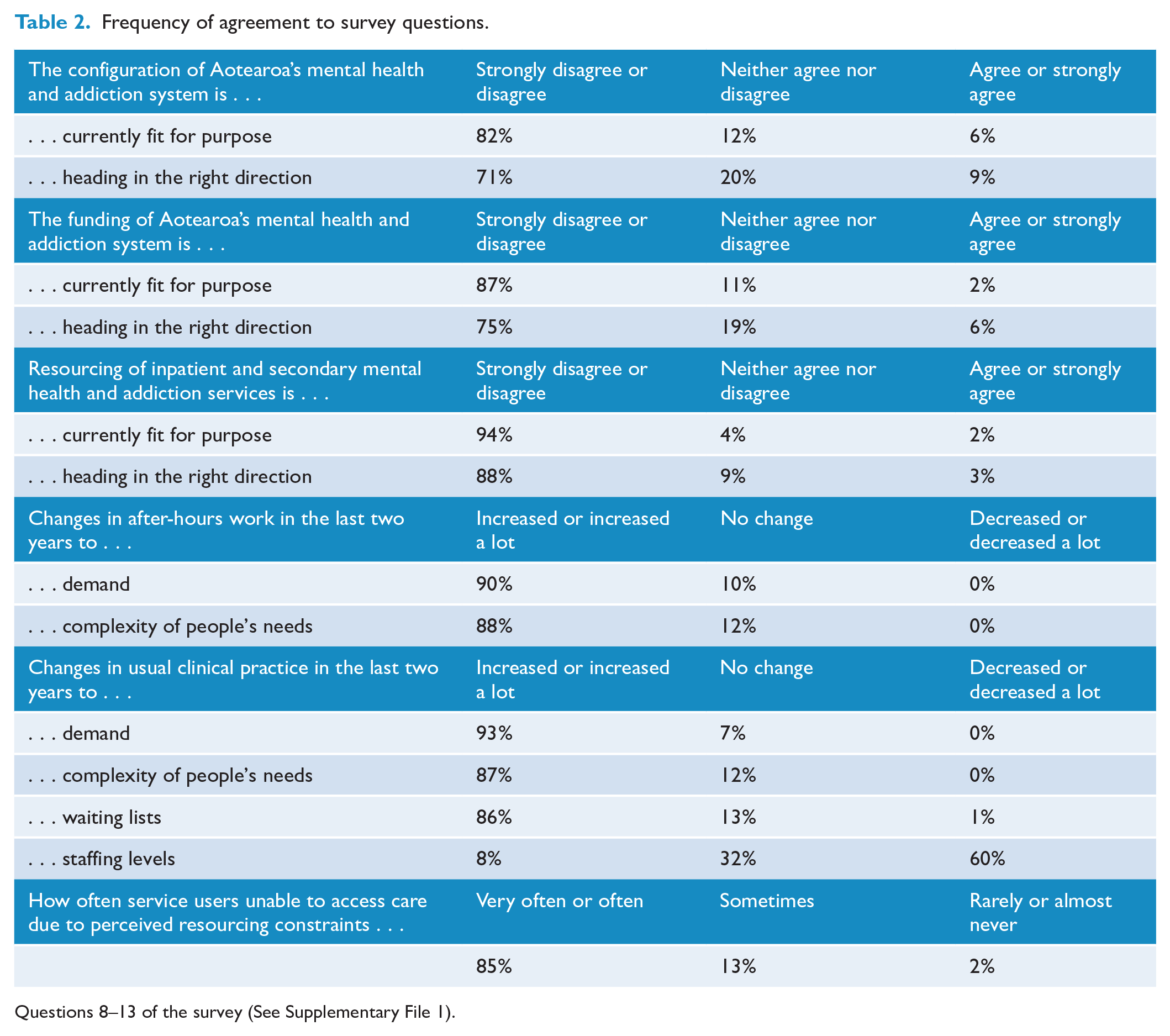
Questions 8–13 of the survey (See Supplementary File 1).
Regarding the configuration of services, psychiatrists commented that services were often disjointed and constructed in a way that did not work well for service users. Many participants also commented on a poorly integrated system for addressing the broader social determinants of mental health.
Many participants discussed the increased funding for primary mental health care in the 2019 budget. Participants were generally supportive of this investment, but noted that in their experience, it had not led to any tangible reductions in pressure on secondary services but it conversely had increased referrals from primary care. While improvements in primary care were considered helpful to address some peoples’ needs, service users with serious and complex mental health issues were thought to also need the support of specialist services, with this population currently being underserved.
The pervasive rhetoric seem[s] to centre around there being plenty of service[s] for the severely mentally ill and the mild to moderate group missing out. Making two hungry people fight over scraps is an unacceptable tactic. The severely mentally ill are [being] very poorly served.
The cohort which uses specialised psychiatric care is not the same that benefit from primary interventions. They need highly trained and structured treatment programmes which are not accessible through primary care providers.
Resourcing of secondary mental health and addiction services
Across all of the questions, the highest level of consensus was regarding current resourcing of inpatient and secondary mental health and addiction services – 94% of participants disagreed or strongly disagreed that resourcing was currently fit for purpose. Most participants also disagreed that this was heading in the right direction. The number of participants who thought that resourcing was fit for purpose or heading in the right direction was striking small – only 2% and 3%, respectively. No specialists in old age, consultation-liaison, intellectual disability, addiction, or psychotherapy expressed positive views in this domain.
Free-text comments on resourcing were made by 190 participants. The most common themes were inadequate staffing and/or the lack of inpatient beds.
On call ‘crisis’ work
After-hours work was a particular source of consternation. For participants who worked on an acute on-call roster, 90% reported that demand in their after-hours work had increased or increased a lot and 88% reported that complexity of people’s needs after-hours had increased or increased a lot. A small number of participants reported that demand and complexity had not changed (9% and 12% respectively), but not a single participant reported they had reduced.
Over 120 participants left free-text comments regarding after-hours work. A key theme was the distress psychiatrists experienced by not providing adequate mental health crisis services to people in crisis.
Being on call is now the worst part of my job and it makes me consider resigning my job. The main problem . . . is the lack of inpatient beds that are available . . . it is knowing what would be a good thing to do and being unable to do it, and then making an alternative plan that you know is a bad one but you have no other options - that is soul destroying.
It is extremely stressful to consistently be having to provide sub-standard care for people in need, not to mention the lack of recovery time before returning back to work for your day job. I have begun to dread being on call . . .
On call is a disaster. I resent having to undertake this much complex work with such limited resource . . . This feels hopeless and abusive for patients and staff.
Other key themes mirrored a perceived paucity of available inpatient beds and understaffing. Comments on after-hours staffing shortages highlighted that this was not confined to a lack of psychiatrists; there were shortages of all mental health professionals needed to provide care. Participants reported that bed shortages meant that acutely unwell people were either not admitted, or were discharged precipitously to create space for the next admission, which then created a cycle of crisis-driven reactive care. Participants described the lack of beds as self-perpetuating – when people have to wait longer to access treatment, they become more unwell in the interim, and then it takes longer to recover (which further reduces capacity).
The main stress on call is a resource issue not a complexity issue. Service users are presenting more often with worse symptoms than two years ago, but this is not due to them being more complex than two years ago, but because they have been unable to receive adequate treatment due to demand.
Approximately one-third of participants mentioned substance use, housing and/or other socioeconomic factors as contributing to both demand and complexity. These factors were thought to complicate the support of people in crisis and make it more difficult for them to recover in the community. Consequently, people got ‘stuck’ in inpatient facilities or there was a ‘revolving door’ of frequent readmissions.
We have difficulties with getting people discharged from hospital as they have no proper accommodation, therefore when you are on call there are often no beds to admit acute patients into. This makes the entire crisis-response system less efficient, and crisis patients end up waiting longer for service. Homelessness also makes it more difficult to keep [people] well in the community, leading to more crisis presentations.
[There is] huge unmet need and complex needs including housing instability, severe deprivation, complex unmet physical health needs and significant unmet need for addiction services.
In participants’ usual area of clinical practice
Similar patterns were reported in psychiatrists’ ‘usual area of practice’, with 93% reporting demand had increased or increased a lot, 87% reporting complexity of people’s needs had increased or increased a lot, and 86% reporting waiting lists had increased or increased a lot.
Conversely, few participants reported an increase in staffing levels (60% reported staffing had decreased or decreased a lot, and 32% reported no change). Some elaborated this was a relative decrease – e.g., there might have been an increase in staff numbers, but this had not kept pace with increasing numbers of people accessing care.
Almost two-thirds of comments discussed staffing pressures. Many were concerned about the impact of burnout and stress on recruitment and retention of staff. Again, this was seen as self-perpetuating – staff were leaving due to stress, which put further strain on the remaining staff.
There were a few statistically significant (but still relatively minor) variations across different sub-specialties. For example, adult (n = 236) and child and adolescent (n = 91) practitioners were more likely than other sub-specialties to report that staffing levels had decreased (64% and 59%), compared with 42% of old age (n = 52) and 45% of addiction psychiatrists (n = 33), p = .05). A subgroup analysis of the 97 child and adolescent participants has been published elsewhere (Every-Palmer et al., 2022). Around 86% of old age psychiatrists (n = 51) reported an increase in demand and 75% reported an increase in waiting lists, which was lower than other sub-specialties (90–97%, p = .05).
Service users’ access to care
Participants were asked ‘Thinking of your area(s) of usual clinical practice in the last two years, how often are patients/consumers unable to access the right mental health care at the right time because of resourcing constraints?’
Most people (85%) reported this occurred often or very often. Similar results were seen across different sub-specialties (see Figure 1). However, there were some statistically significant differences – old age psychiatrists (n = 53) were less likely than other sub-specialties to report service users were ‘often/very often’ unable to access the right care (70%), while consultation-liaison psychiatrists (n = 35) were more likely to report this (100%).
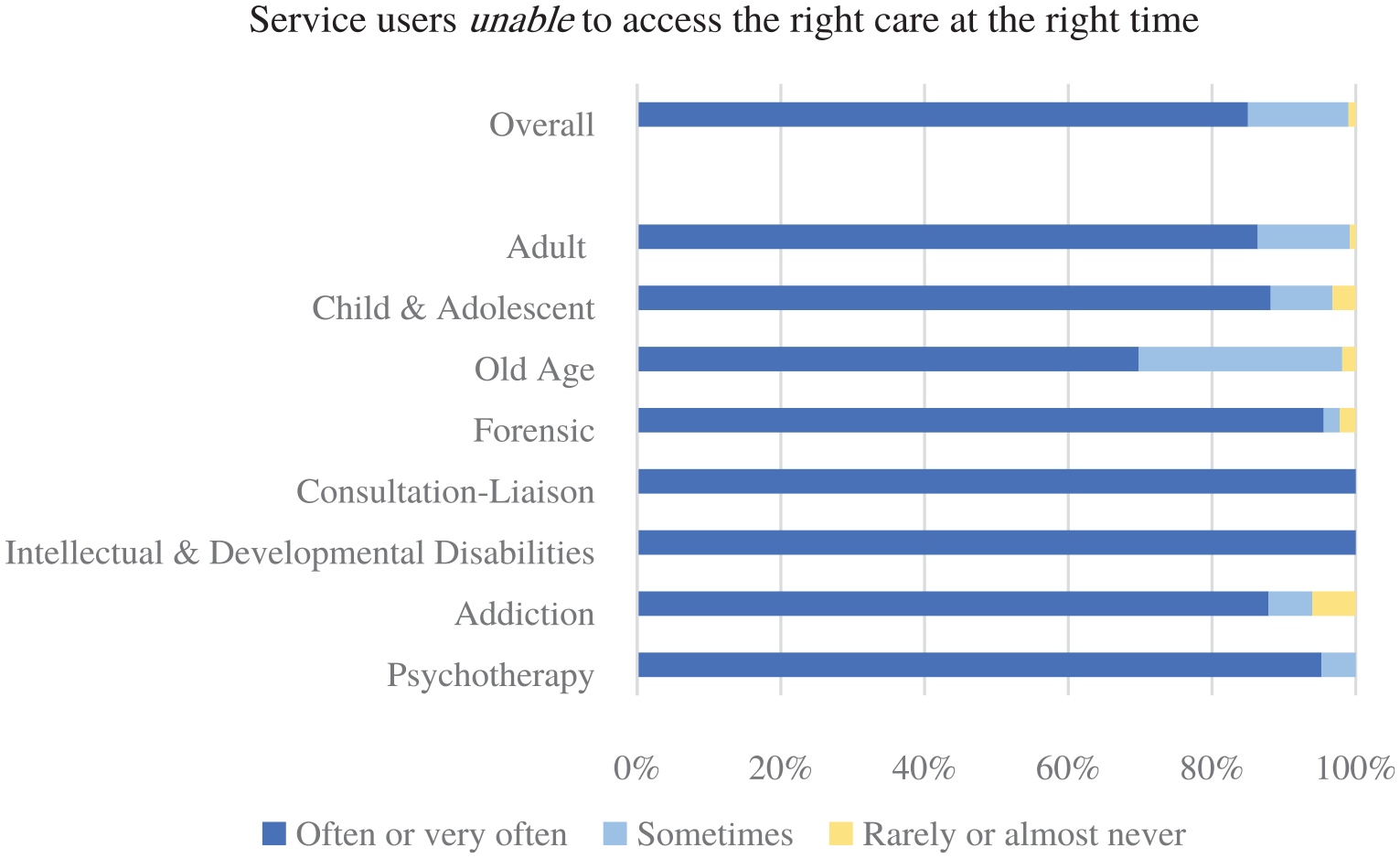
How often patients/service users are unable to access the right mental health care at the right time because of resourcing constraints reported by specialty area.
Of the 150 participants who provided additional comments, over a third mentioned a shortage of psychologists or psychological therapies as key barriers to people accessing the care they required.
What is working well?
When asked ‘Thinking of your area(s) of clinical practice, what are some things that are currently working well?’, participants often referred to their team or the commitment of staff (44% of responses). Others reported how much they enjoyed working with service users.
There are lots of hard working/committed team members who do their best for the clients and each other.
The current staff! Those mental health professionals that are sticking at it, going above and beyond their duties. They need to be recognized and valued.
Many participants applauded the movement over time from a medico-centric model towards a more holistic multidisciplinary approach, with the evolution of valuable new cultural and peer-support workforces.
. . . holistic approaches, continued therapeutic empathy, appreciation for the person behind the illness, and commitment to the public.
Māori and Pacific cultural workers, and more and more Māori, Pacific and Asian staff trained and coming to join [mental health services]
What would psychiatrists change to improve services?
More than 430 participants provided a suggested priority to improve the mental health and addiction system (total n = 837 suggestions, with an average of two suggestions per participant). Many participants provided non-specific responses; ‘increase staffing’, ‘more funding’ or ‘the whole system needs change’ were common themes. However, a number of participants provided detailed responses and specific ideas.
Workforce issues received the greatest number of mentions (n = 158). Participants described significant and pervasive workforce shortages across the board with inadequate numbers of regulated mental health and addiction staff (all professions) and peer-support workers to meet current demand. Recruiting additional staff or creating more positions was mentioned 120 times. Employing more multidisciplinary staff was emphasised as important to ensure the diverse needs of people seeking support could be met. Addressing the acute shortages of mental health clinicians who could deliver evidence-based psychological therapies in the public system was viewed a priority.
Increasing the number of psychologists employed or alternatively, increasing the number of psychiatric registrars [trainees] and encouraging them to do more therapy.
Participants also emphasised the importance of valuing and retaining existing staff, noting the risk of burnout and job dissatisfaction leading to a self-perpetuating downwards spiral of workforce attrition.
Turnover of staff is a major issue. Each time a disillusioned staff member leaves, their caseload is distributed among already stressed remaining clinicians.
Improve inpatient facilities
A desire for more acute resources and improved inpatient facilities was another strong theme. Participants described a disconnect between the demand for inpatient beds and the number of beds currently available.
Ensure inpatient units are fit for purpose and regularly upgraded in line with other hospital areas.
Some noted that a plan was needed to develop more rehabilitation services and intermediary services for service users to be able to transition better between services suited to their current needs. Some participants described the inpatient units in their areas as unfit for purpose and in dire need of refurbishment or replacing.
Increase funding for specialist services
Specialist services (including services for older people, infants, children, adolescents and intellectual disability) were identified as in urgent need of increased funding/resourcing to adequately support the demand for services. It was noted that funding should be based on adjustable models aligned with health need and population dynamics, rather than fixed models. Others commented that more funding should be directed towards prevention and mental health funding should be ring-fenced.
Improve integration of primary and secondary services
Some 47 mentions were made regarding primary mental health and addiction services. Participants felt greater integration was required between primary and secondary services for the system to work effectively, and primary care required greater support from secondary care. This included more training, increased access to psychotherapy and more psychiatry and psychology consultations to support GPs.
Improve relationship between primary to secondary care including increasing training for GPs, perhaps embedding a psychologist in GP practices.
Several participants stated that greater investment in primary care increased the workload and stress on the secondary sector by driving more referrals; therefore, a whole-of-system approach is required. Several participants noted people might not be able to afford to see a GP for ongoing mental health care and would present to EDs or crisis services instead.
I do think that an increase in funding directed to primary care is the right direction. However, there is a misconception that if you treat things in primary care this will translate to less demand on acute services, when the opposite is the case.
Address underlying social determinants
As well as addressing health system issues, there was a strong desire to direct funding towards addressing the social and economic factors that drive poor mental health outcomes and inequities such as institutional racism and colonialism, poverty, violence and abuse, homelessness, poor quality housing, substance use, inequitable access to education and health care and to supporting parenting skills (n = 64).
Multi-agency response to address social determinants of mental health particularly housing, education, social deprivation - these are driving the complexity and prevalence of crisis presentations.
Invest in wrap around services for disadvantaged children - inconsistent care placements, cultural disconnection, and trauma are setting children up for a lifetime of hardship, disadvantage and contact with MHS [mental health services] which may have been preventable.
Investing in correcting the socioeconomic determinants of mental health was considered a priority. The housing crisis was mentioned eight times, and it was noted that more houses are required to address poverty and homelessness.
More robust clinical governance
Many psychiatrists felt they ‘weren’t being listened to’ and were undervalued. Some 39 participants voiced concerns that service design decisions were being made by people with limited understanding of the complexities of mental illness and substance use. Other participants reported not feeling trusted by managers. It was considered that better clinical ‘leadership’ rather than ‘management’ would result in a more effective healthcare system and greater satisfaction and retention of staff.
Discussion
Our study indicates that psychiatrists in New Zealand are pessimistic about the state of mental health and addiction services. Most psychiatrists think the system is not fit for purpose and believe that people are unable to access mental health care due to resourcing constraints. These concerns exist in an environment where psychiatrists report escalating demand, increasing complexity, growing waitlists and reduced staff levels.
These issues are not new (Association of Salaried Medical Specialists, 2021b; Meier and Lourens, 2021; Monasterio et al., 2020); nor are such concerns unique to psychiatrists in New Zealand. However, the country should be in a somewhat unique position to improve its mental health and addiction system following a major government inquiry into mental health and addiction in 2018 (New Zealand Government, 2018b), substantial funding injections via recent government budgets (New Zealand Ministry of Health, 2022a, 2022b) and a recent overhaul of the health system (New Zealand Ministry of Health, 2022c).
The government-promoted premise that increased upstream intervention would reduce the need for specialist services is contentious. Thus far, ‘upstream’ has meant increasing access to brief and novel forms of primary care support (19, 20). To date, this has had little discernible impact on more than a decade’s worth of increasing demand for psychiatrists and specialist mental health services (18). It has been estimated that for specialist services ‘the average funding per client in real terms actually has decreased by an estimated 38% from 2008/09 to 2019/20’ (Association of Salaried Medical Specialists, 2021b). The true prevalence of moderate-to-severe mental illness is closer to 5% than the 3% ring-fence set in the 1990s. In Te Rau Hinengaro, an epidemiological survey of high prevalence mental health conditions undertaken in 2003 to 2004, 4.7% of the adult population had severe mental health needs in any year (Oakley Browne et al., 2006). Ring-fenced funding for specialist mental health services should be increased to cover the 5% of the population with significant needs.
In the context of the COVID-19 pandemic, there has also been limited additional funding to boost immediate care for those with moderate-to-severe issues, and this has led to increased concern and risk of burnout among a perennially limited pool of psychiatrists (Chambers and Frampton, 2022). A long ‘tail’ of pandemic-related psychological sequelae is anticipated, and gains from any type of upstream prevention efforts may take decades to manifest (Clift et al., 2022). As a result, there is likely to be continued demand for current or greater levels of specialist (including psychiatric) services for quite some time.
While our study demonstrated concern about the future of our mental health and addiction system, participants highlighted the strengths of a committed, multidisciplinary workforce, with increased cultural and peer-expert capacity. Most feedback highlighted the need to boost access to specialist staffing and services in the short-term, while improving longer-term health and non-health-related upstream prevention of mental health and addiction issues. In terms of psychiatry, psychiatry training schemes across the country have noticed a significant upswing of interest in the discipline, with more eligible candidates than there are places available (Alan Faulkner, Chair RANZCP New Zealand training committee, February 2023, personal communication). If more positions were to be funded – as is required – there is a promising talent pool available to fill them.
Participants recognised that all levels of the health system are inter-related and that focusing on part of the system (such as primary care) means the pressure point is just moved to a different area. Providing adequate facilities that match the service user’s journey is also a key requirement. In particular, the participants noted a lack of long-term community facilities for those with more complex presentations and challenges in finding appropriate accommodation to discharge service users who need support.
Our study derives these views and suggestions from the doctors working at the coal-face of New Zealand’s mental health and addiction system. Strengths of our study include the high response rate and the collection of quantitative and qualitative feedback. Limitations include the subjective nature of findings, finite depth of questioning and potential selection bias (those doctors with stronger opinions were probably more motivated to take part). This survey only recruited psychiatrists. It would be useful for future research to also seek the views of service users, families and other mental health clinicians.
As noted by Braun and Clark (Braun and Clarke, 2006), data are not coded in an epistemological vacuum. Six (from seven) of this study’s authors were psychiatrists, and we were all members of the New Zealand Committee of the RANZCP. The framing of the questionnaire and our interpretation of free text themes may have been biased by our professional backgrounds and positionality. Furthermore, words/text do not operate as external signs of internal meaning for the individual participant but rather as a pre-determined system for the allocation of meaning (Crowe, 1998). Perceptions are dynamic, so the same questionnaire may have elicited different responses at different points in time. However, our results can be triangulated with a survey of New Zealand psychiatrists published by the Association of Salaried Medical Specialists in November 2021 that reported similar increases in caseload, complexity and dissatisfaction with the resourcing of specialist mental health services (Association of Salaried Medical Specialists, 2021a). In addition, in that survey, 45% of psychiatrists said they would leave their current job if they could. These data alongside our representative sample and high response rate give validity to our finding that New Zealand psychiatrists are very concerned about the current state and future direction of their mental health and addiction system.
Further exploration of the perspectives of the non-psychiatric workforce and patients/service users is needed to better understand to what extent the views of psychiatrists are role-dependent or a genuine reflection of the state of specialist services. Longitudinal studies, perhaps using the integrated data infrastructure (IDI) may help determine the veracity of the premise that upstream intervention will reduce demand for specialist services.
Conclusion
The majority of psychiatrists believe specialist mental health and addiction services in New Zealand are not currently fit for purpose and that they are not heading in the right direction. Remedies include boosting ring-fenced funding to reflect the 5% of New Zealanders with severe mental health needs; actively addressing the critical workforce pipeline (including the number of psychiatrists); and urgently improving the experiences of mental health staff. A skilled and adequately staffed multidisciplinary workforce that includes peer support and cultural capability is an extant strength. This workforce needs to be grown and nurtured to achieve the highest attainable standard of mental health for the people of New Zealand.
Me mahi tahi tātou, mō te oranga o te iwi katoa (we work together for the well-being of everyone).
Supplemental Material
sj-docx-1-anp-10.1177_00048674231170572 – Supplemental material for Not heading in the right direction: Five hundred psychiatrists’ views on resourcing, demand, and workforce across New Zealand mental health services
Supplemental material, sj-docx-1-anp-10.1177_00048674231170572 for Not heading in the right direction: Five hundred psychiatrists’ views on resourcing, demand, and workforce across New Zealand mental health services by Susanna Every-Palmer, Marion L Grant, Hiran Thabrew, Oliver Hansby, Mark Lawrence, Matthew Jenkins and Sarah Romans in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors thank Rosemary Matthews, Corban Avery, and all the members of Tu Te Akaaka Roa/the New Zealand National Committee, RANZCP, for invaluable support with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.