
Abstract

In 1990, obsessive-compulsive disorder (OCD) was ranked in the 10 most disabling of all illnesses, alongside conditions such as osteoarthritis and chronic obstructive pulmonary disease (Murray et al., 1996). That was the last time OCD was assessed as a discrete entity in the Global Burden of Disease studies. In the interceding 30 years, the Australia healthcare system has seen world-leading advances in clinical research driven by collectives for dementia, psychosis, eating disorders and autism. People with OCD and related disorders (OCRDs) have not yet benefitted from this type of evolution in research and service provision. COVID-19 has underscored the urgency for action by triggering presentations of new cases and deterioration of previously well-managed symptoms. The time for action on OCD is now. We propose radical transformation of clinical research and service resourcing and organisation in Australia by way of strengthened collaboration between consumers, carers, clinical services, professional bodies, policymakers, and researchers.
Prevalence and burden
OCD affects 1 in 50 people in their lifetime, that is, 140 million people globally, including 500,000 people across Australia (Ruscio et al., 2010). It is associated with functional impairments across home life, social life, work/school and overall quality of life in addition a $3.4 billion annual loss to the Australian economy, accounting for both direct (e.g. healthcare) and indirect (e.g. lost productivity) costs (McCallum et al., 2019). Fortunately, we know what age most people will develop OCD symptoms – during the two peaks of onset in late childhood or early adulthood respectively – and so targeted early detection and intervention is indicated for this critical window.
Need for clinical service enhancement
In addition to high prevalence and severity, OCD is associated with a long duration of illness. Moreover, Australian data show that people with OCD wait 9 years for treatment (Cooper et al., 2022). The reasons for these delays to diagnosis and treatment include factors relating to patients (e.g. secrecy), clinicians (e.g. training and supervision) and services (e.g. adequate resourcing) (Cooper et al., 2022). Fortunately, OCD can be reliably detected through brief, routine screening measures, which can address some of these factors. Indeed, universal screening for OCRDs has been proposed in other countries, such as the United Kingdom, based on the high prevalence, burden, lifespan course and delays in access to care. We propose that there is a demand for routine screening of OCD in Australia.
If detected, there are validated, reliable assessment and diagnosis measures, assessing symptoms, severity, family accommodation, global functioning and quality of life. More importantly, there are numerous evidence-based treatment options for OCD, including psychological therapy, medications and neurostimulation. Cognitive-behavioural therapy with exposure and response prevention (ERP) is the first-line evidence-based treatment. ERP achieves treatment response in approximately two-thirds of patients across the lifespan, although remission rates are somewhat more favourable in children and adolescents – underscoring the need for early intervention. Selective serotonin reuptake inhibitors are more accessible than ERP and offer a moderate effect size. Repetitive transcranial magnetic stimulation and deep transcranial magnetic stimulation have an emerging evidence-base, supported by RCTs, particularly for treatment-resistant OCD (Lusicic et al., 2018). The major bottleneck in treating the OCRDs is therefore not the absence of efficacious treatments but rather the absence, or inadequacy, of implementation of these treatments in the community. Treating OCRDs requires a specialised skillset, with almost 200 unique competencies identified to effectively assess and treat OCD alone (Sookman et al., 2021). As such, clinical skill capacity-building and maintenance is essential.
Despite the strong evidence base for assessment and treatment options, Australia has no state-wide or national services, service plans or clinical guidelines for management of OCRDs. In 2006, the evidence base for OCD was already considered sufficient to develop UK clinical guidelines for OCD (National Collaborating Centre for Mental Health, 2006). Australian clinical guidelines and state-based service plans (including supported training and supervision of clinicians) would increase implementation of evidence-based practice. As with any mental health diagnosis, patients in Australia with OCRDs can access rebates for up to 10 individual treatment sessions per year with a referral from a medical doctor, funded by the Australian government’s Medicare’s Better Access scheme. However, the proven adequate ‘dose’ of ERP is upwards of 13 hours. The eating disorder movement has shown how effective advocacy can be in this space (Box 1).
Government-funded state-wide or national specialist public mental health services.
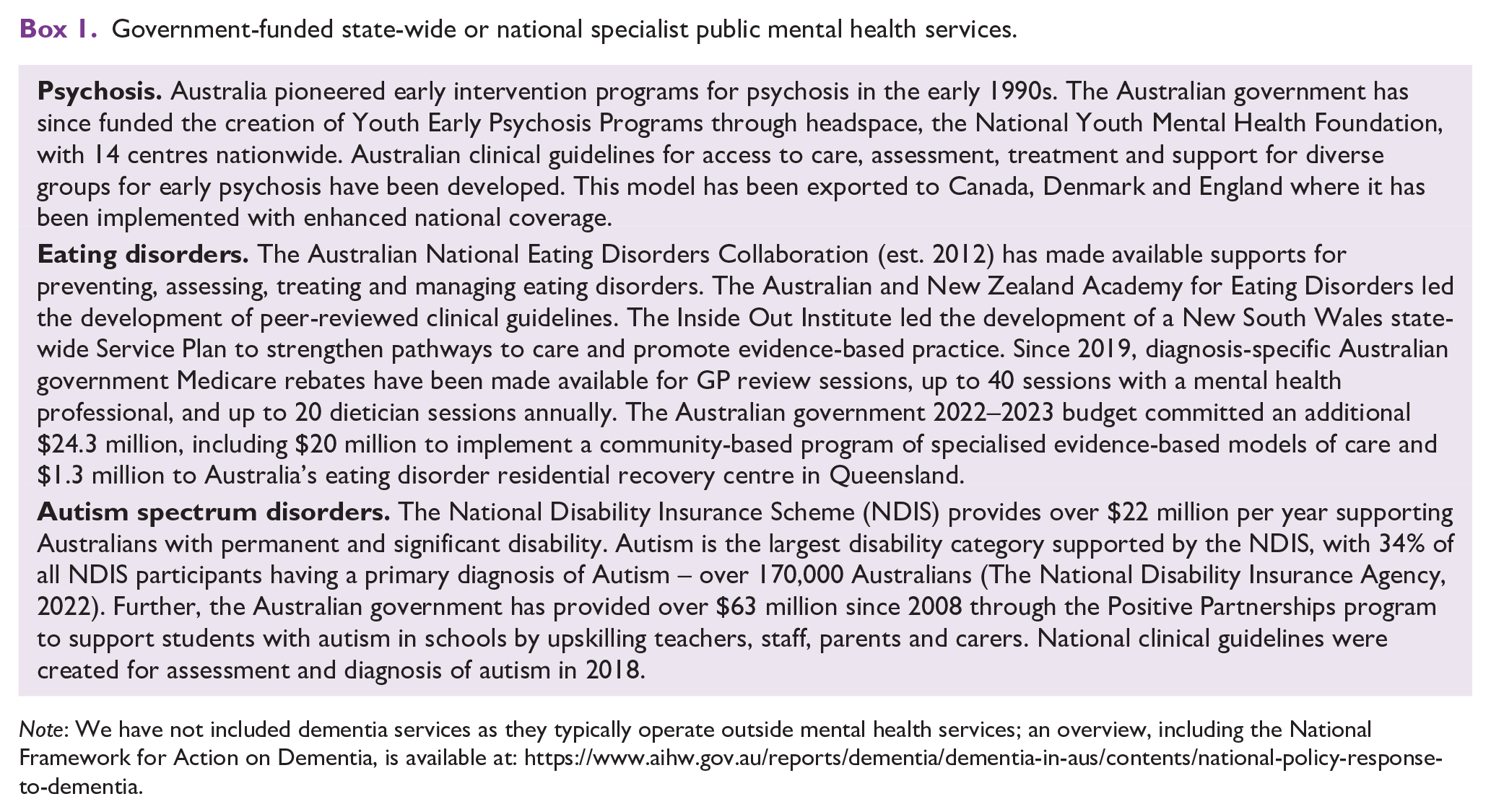
Note: We have not included dementia services as they typically operate outside mental health services; an overview, including the National Framework for Action on Dementia, is available at: https://www.aihw.gov.au/reports/dementia/dementia-in-aus/contents/national-policy-response-to-dementia.
Need for boosted research funding
Despite their overall high efficacy, many people with OCRD have an insufficient response to first line or other currently available treatments – even in the controlled setting of clinical trials. Our aim as researchers and clinicians must be to select the treatment with the highest chance of success. Within OCD, there is substantial heterogeneity of presentation and treatment response – understanding this heterogeneity could hold the key to accurate selection of existing treatments for each patient in addition to development of novel or augmented treatments for non-responders. Further, to boost the effectiveness of treatments, more research is necessary to uncover how to best implement these evidence-based treatments in routine clinical care, including how to best train and supervise clinicians to ensure effective implementation. Beyond improving the effectiveness of treatments, research should also seek to improve the cost-effectiveness, timeliness and scalability of treatments.
For further research to occur, one requirement is adequate research funding. There is documented discrepancy between the funding of mental health disorders relative to other medical conditions – that is, disproportionate to their prevalence, economic impact and the burden of illness (Batterham et al., 2016). Within mental health research, starting in the early 1990s, national advocacy efforts for psychosis were amplified and dedicated service plans and treatment teams were created. In more recent years, eating disorders and autism advocacy has followed a similar trajectory, spurring increased research funding and subsequently the creation of specialist services (Box 1).
National Health and Medical Research Council (NHMRC) data (2013–2021) show that whereas eating disorders funding, for example, has shown incremental growth over the past decade, OCD resourcing remains relatively static and low (Figure 1). In comparison, dementia funding demonstrates the power of advocacy including mechanisms to ring-fence research funding for specific areas of need – an approach that could be applied to OCRDs and other highly prevalent and burdensome mental illnesses, for example, anxiety disorders, major depressive disorder.
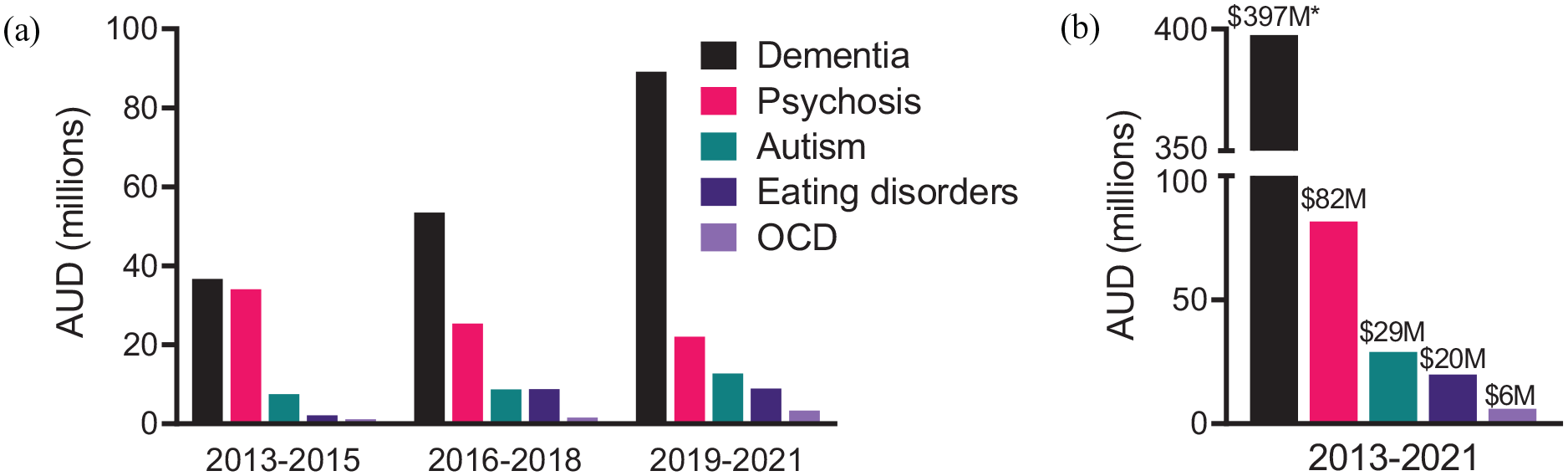
NHMRC funding across mental health diagnoses (2013–2021).
Need for strengthened collaboration and advocacy
A vital component to enhancing research and clinical service funding and organisation is the strengthening of collaboration between researchers, clinicians, consumers and their carers and leveraging of this collective to advocate for people with OCRDs. This type of collective coordination from fields including psychosis, eating disorders demonstrates the power of this approach enhancing awareness of the burden carried by people with OCRD and their families in addition to the quality of clinical care for consumers. Professional societies including the Royal Australian and New Zealand College of Psychiatrists, Australian Psychological Society, Society for Mental Health Research, Australian Mental Health Think Tank and Biological Psychiatry Australia have an opportunity to help strengthen ties within the OCRD field in Australia, perhaps leveraging international collectives to more successfully lobby government. However, the onus is also on researchers, clinicians and service providers to collaborate and to seek out the perspectives and knowledge of those with lived experience of OCRDs and their carers.
Co-authors IP, JG and LF have begun this vital work by collaborating across research institutions, with public health service providers, hospitals and patients and carers with the formation of OCD BOUNCE. This collaboration has led to increased screening for OCRDs within public health services, piloting of group and intensive ERP within routine care and providing specialised case consultation, training and supervision to clinicians. However, we recognise that these collaborations are still in their infancy and far more work is needed to truly revolutionise OCRD clinical research and service provision in Australia.
Conclusion
Despite its substantial functional and economic consequences, OCRD in Australia are under-diagnosed, under-researched, under-treated and under-funded. We must radically re-imagine the resourcing and organisation of OCRD assessment, treatment and research to address the substantial burden attributable to these disorders. Treating OCRD early and effectively results in more clients being relieved of symptoms and reduces family burden, disease burden and lifetime morbidity. OCRD researchers, clinicians, patients and carers can jointly advocate for commensurate research funding and the development and implementation of state or national service plans and specialised capacity-building and quaternary treatment services, which can leverage the existing well-validated screening and assessment measures and evidence-based and cost-effective treatments. Further research is also needed to increase the effectiveness of treatments for non-responders, to better understand the heterogeneity across OCD and to establish how to best train clinicians to detect, assess and treat OCD – among myriad other vital and necessary research questions. All of this has the potential to dramatically improve the quality of life for people living with OCD.
Footnotes
Acknowledgements
The authors thank Professor Henry Brodaty, Professor Phillipa Hay and Professor Patrick McGorry for their comments on this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KD was supported by project grant funding from Mindgardens Neuroscience Network. All other author were employed as academic staff at their affiliated institutions.