
Abstract

Introduction
Kaua e piki ko koe kau ake, engari e piki kātahi, me tōu iwi
[Don’t climb the mountain by yourself but have your people climb with you]
This whakataukī (Māori proverb) reminds us that to achieve improvements in mental health, we should strive for equity for all of our communities. It will resonate with many working in mental health on both sides of the Tasman.
New Zealand and Australian psychiatrists share a friendly rivalry over the patrimony of the pavlova and strong collegial relationships professionally. We belong to the same binational College, we subscribe to this journal and we hold many of the same values. However, we have also been shaped by different sociocultural winds and currents, which can sometimes lead to misunderstanding. As New Zealand psychiatrists active in Australasian governance and research, we have found that despite openness to hear more from our Australian colleagues, New Zealand’s legacy of colonisation is not well understood nor are the legal obligations to uphold our founding document, Te Tiriti o Waitangi. In this editorial, we seek to briefly explain how breaches of this treaty and colonisation have led to inequities for Māori, which are especially pronounced in mental health. We explain how over recent decades there has been an increased focus on righting past wrongs and better upholding the rights of Māori, an ethnicity with which 17% of New Zealanders identify. 1 Currently, this is evident in sweeping reforms to the health system and health research funding streams. We explore what this means for the joint enterprise of ‘Australian and New Zealand psychiatry’. Lastly, we consider the role of journals such as this one in giving voice to research that is responsive to Indigenous mental health and wellbeing. We find that historically this journal has not included the diverse perspectives of Indigenous researchers and our wero (challenge) is to do better in the future.
Brief history of Māori and European arrival in Aotearoa
The first settlers to Aotearoa New Zealand arrived from Polynesia between 1200 and 1300 AD. They discovered the motu (country) through deliberate exploration of the Pacific Ocean, using the stars, ocean currents and prevailing winds as navigational tools. Following the discovery of Aotearoa, small tribal groups started arriving in large waka (canoes). Now known as Māori, historically these tribes did not characterise themselves by a collective pan-tribal term, identifying instead through their tribal landmarks (land, mountains, sea and rivers), which then linked them to their whānau, hapū and iwi (family and tribe). The same system existed in First Nations people of Australia. However, with the arrival of Europeans, the Indigenous people started using the term ‘Māori’ meaning ‘ordinary’ or ‘common’ to distinguish themselves from the uncommon foreign settlers (Pākehā). This wave of European immigration started after the arrival of the Endeavour captained by James Cook in 1769. Following Cook’s visit, European whalers and sealers began settling in Aotearoa, followed by traders in ever greater numbers. By the 1830s, the British government was being pressured to reduce the lawlessness of the European settlers and to pre-empt France, who was contemplating the value of Aotearoa as a potential French colony. In 1835, He Whakaputanga o te Rangatira o Nu Tireni – The Declaration of Independence of the United Tribes of New Zealand – attested that New Zealand was an independent Māori nation.
The treaty – Te Tiriti o Waitangi
On 6 February 1840, the British Consul to New Zealand, William Hobson, invited Māori chiefs to assemble at Waitangi to sign a treaty with the British Crown. The resulting treaty – Te Tiriti o Waitangi – was eventually signed by over 500 chiefs. It envisaged a relationship of mutual benefit between those who were here (tangata whenua) and all those who were to come (tangata tiriti). It was an agreement to an on-going power-sharing relationship, in which the autonomy/rangatiratanga of hapū/iwi (subtribes and tribes) was affirmed. However, the English and Māori versions stipulated different things: the former mandated that the Crown would have full control New Zealand’s territories, whereas the latter (signed by the Māori chiefs) indicated that Māori would retain full sovereignty over their tribal lands.
Breaches of Te Tiriti and the effects of colonisation on mental health
Crown breaches of Te Tiriti have had severe and destructive consequences. Through land wars and land confiscation, economic deprivation, mass European immigration, cultural marginalisation, forced social change and structural racism, Māori culture, economies, populations and rights have been diminished and marginalised across more than seven generations (Moewaka Barnes and McCreanor, 2019).
The enduring impacts on Māori are a root cause of persisting health inequities (Harris et al., 2018; Reid et al., 2019). This is especially evident in mental health. Māori experience significantly higher rates of mental illness, higher rates of suicide and greater prevalence of addictions. However, these inequities have emerged only from 1970s onwards.
Multiple studies over the last two decades have shown higher rates of mental distress among Māori compared with non-Māori. Further, Māori are 30% more likely than other ethnic groups to have their mental illness undiagnosed, have lower access to treatment in primary care and poorer outcomes for those who access mental health services (Cunningham et al., 2018).
Righting past wrongs: Health reform and research priorities
Over recent decades, there has been increased focus on upholding the treaty, compensating for past harms and abuses, restoring mana and correcting injustices and inequities. Since 1970s, there have been Treaty settlements and the transfer of assets in forestry, fisheries, broadcasting, etc., back to tangata whenua.
Health reform is currently a major focus. The status of Māori health equity was challenged in the Waitangi Tribunal through the WAI 2575 claim. Outcomes of the landmark decision signified a new phase for Māori health and a system-wide focus on cultural safety and equity. Aotearoa is undergoing the most significant health restructure in decades, with a major objective being to achieve better and more equitable health outcomes, particularly for Māori. The Pae Ora (Healthy Futures) Bill will disestablish all 20 district health boards and transfer all their functions to Health New Zealand and a Māori Health Authority. The bill also provides a framework for recognising iwi–Māori partnership.
Work is also currently underway to ensure a more representative health workforce. For example, at Otago Medical School where two of the authors of this editorial work, Te Kauae Parāoa (the former ‘Mirror on Society’ selection policy) promotes and facilitates academic equity for Māori students and for students from four other under-represented and priority categories (students with rural, refugee, Indigenous Pasifika and low socio-economic backgrounds). The aim is to achieve a health workforce that reflects the ethnic and socioeconomic diversity of the society it serves. Consequently, there has been a tremendous growth in the proportion of Māori medical graduates at the University of Otago, of whom 20% identified as Māori in 2021. The downstream benefits of this are yet to be realised in mental health and shamefully for us as a profession, only 4.4% of New Zealand psychiatrists are Māori.
In 2021, the Royal Australian and New Zealand College of Psychiatrists (RANZCP) affirmed its commitment Whānau Ora (a Māori response to the delivery of social and health services to improve outcomes for Māori family and communities), and in 2022, the College produced a position statement to committing to give effect to the principles of Te Tiriti across its membership and the organisation (RANZCP, 2022).
Although historically the interests of Māori were often ignored or overlooked by mental health researchers, contemporary locally produced research is increasingly likely to be Māori responsive. As identified in the 2017–2027 Health Research Strategy, treaty principles are fundamental to all health researches in the country. The reasons for this are to honour the obligations defined in Te Tiriti o Waitangi and to correct the inequitable health outcomes experienced by Māori. All Health Research Council grant proposals are now scored against the Māori Health Advancement Criteria that contain four domains: (1) Relationships with Māori, (2) Significance to Māori, (3) Research team contains appropriate Māori expertise and (4) Research is conducted in a Māori sensitive way (according to tikanga). Research proposals require consultation with Māori prior to ethics approval. Hence, we can expect much more Māori responsive mental health research to originate from Aotearoa in coming years, as research that does not meet the criteria is unlikely to be funded or approved.
How is this journal doing in supporting Indigenous mental health research?
Unfortunately, our track record is not great. Te Kaunihera mō ngā kaupapa Hauora Hinengaro Māori and the New Zealand National Office of the RANZCP undertook a review of research published by the Australian and New Zealand Journal of Psychiatry (ANZJP) between January 2019 and December 2020 (Table 1). Of 24 editions containing a total of 266 published articles, only 4 (1.5%) contained reference to Māori (which may have included mention of Māori ethnicity data) and only 3 had at least one author who could be identified as a Māori researcher. Overall, it was concluded that the ANZJP has historically published few research articles that contribute to the understanding Māori mental health, uncover the particular challenges facing Māori or articulate Te Ao Māori perspectives on mental health.
Review of articles published in the Australia and New Zealand Journal of Psychiatry between 2019 and 2020, looking for Māori content and authorship.
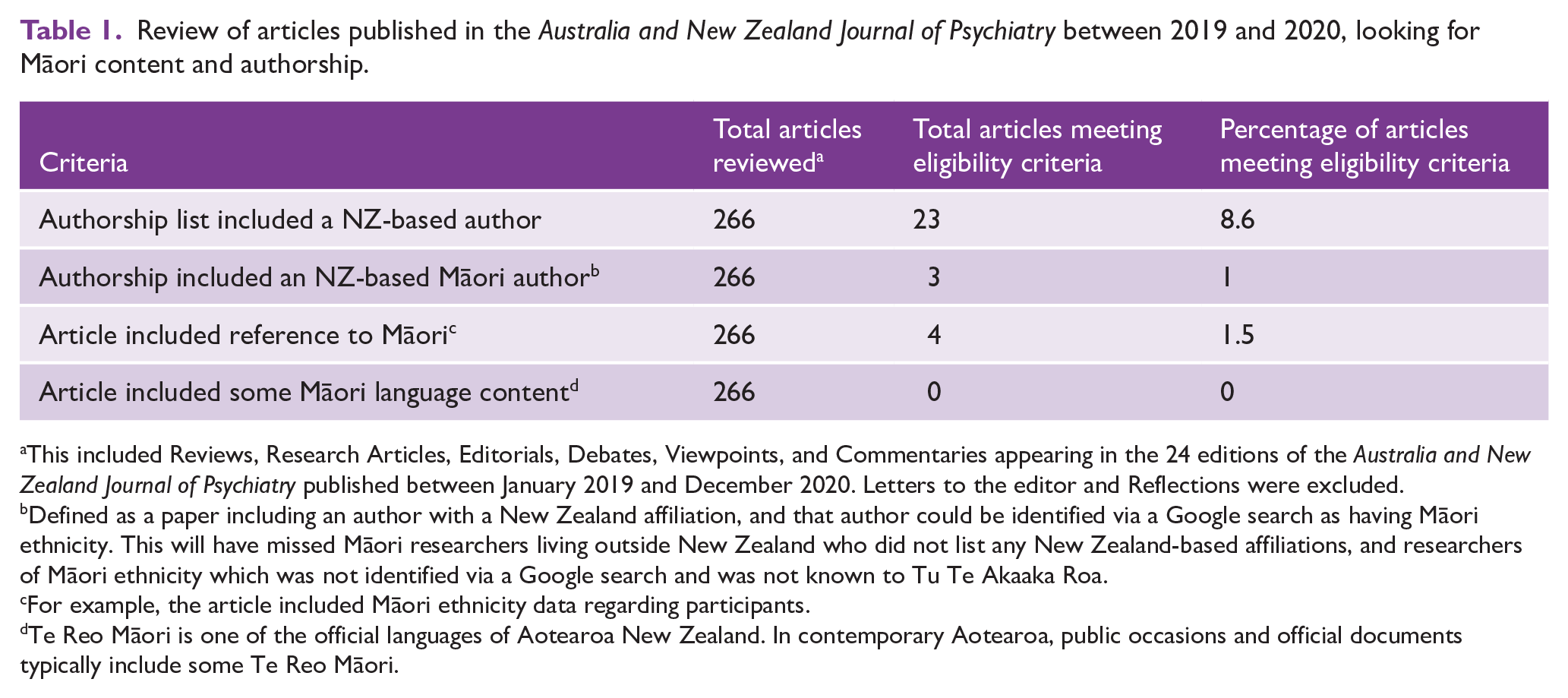
This included Reviews, Research Articles, Editorials, Debates, Viewpoints, and Commentaries appearing in the 24 editions of the Australia and New Zealand Journal of Psychiatry published between January 2019 and December 2020. Letters to the editor and Reflections were excluded.
Defined as a paper including an author with a New Zealand affiliation, and that author could be identified via a Google search as having Māori ethnicity. This will have missed Māori researchers living outside New Zealand who did not list any New Zealand-based affiliations, and researchers of Māori ethnicity which was not identified via a Google search and was not known to Tu Te Akaaka Roa.
For example, the article included Māori ethnicity data regarding participants.
Te Reo Māori is one of the official languages of Aotearoa New Zealand. In contemporary Aotearoa, public occasions and official documents typically include some Te Reo Māori.
It is not clear from this audit whether this absence of Māori-relevant mental health research is simply because few such articles have been submitted, or whether such articles are more likely to face negative editorial and peer review due to ignorance, unfamiliarity or racism. We note that Māori research may not be modelled on western paradigms of scientific or medical endeavour and consequently may not be valued within a western biomedical framework as contributing to evidence (Reid et al., 2017).
Indigenous Australian research through the same lens
If you are Australian, you may well be thinking that the issues raised in this editorial should equally apply to Australia and Indigenous Australians. We agree. Australia also has a dark history of colonisation and pervasive discrimination, which has led to similar restrictions on self-determination and marked inequities, including poorer mental health, for its First Nations people. We have focused on Aotearoa because this is what we know – we are New Zealanders, and three of us identify as Māori. We do not presume to have knowledge into the experiences of Indigenous Australians and defer to those with the expertise to comment. However, we strongly suspect that if the audit described in the previous section was repeated looking at Aboriginal and Torres Strait Islander research and researchers, the findings would be the same. In the following section, we make recommendations which we hope will better support and promote all Indigenous mental health researches in this journal.
What role can the ANZJP play in uplifting Indigenous mental health?
The ANZJP positions itself as the ‘leading psychiatry journal of the Asia-Pacific region’. If we aspire to this goal, then we must include all peoples within the journal including our Indigenous Peoples. We have suggested four possible (non-exhaustive) remedies that this journal might take as first steps to better promote Indigenous mental health research.
Firstly, the journal should increase opportunities for Indigenous communities who are impacted by mental health inequities to have their research published. This might include special topics or invited pieces from Indigenous researchers.
Secondly, we suggest the ANZJP’s advisory board should be broadened to include more Indigenous mental health experts. This month marks the appointment of one of the authors of this editorial (CL, Te Atiawa) as Associate Editor with a focus on Indigenous mental health. The journal is interested in appointing more experts in Indigenous mental health to the board and we welcome further expressions of interest or suggestions.
Thirdly, the editorial board should make the expectations of the Journal explicit with regard to the use of ethnicity data and non-discriminatory language. The ANZJP should think about adopting the CONSIDER statement, which synthesises international evidence to provide a checklist for the best practice reporting of health research with and involving Indigenous peoples to advance Indigenous health outcomes (Huria et al., 2019).
Lastly, the audit described in Table 1 should be repeated in two years’ time interval to measure progress.
Conclusion
It is a positive step that our College has formally recognised the importance of He Whakaputanga and Te Tiriti; however, this needs to be converted to tangible action. Without our profession championing excellence in Indigenous mental health research and addressing the inequitable representation of our First Nations content, few Māori and Aboriginal and Torres Strait Islander psychiatrists will choose a career in academic research. Because research informs mental health treatments and health policy, the absence of a diverse Indigenous voice will ultimately disadvantage Indigenous people, the mental health and wellbeing of our countries, and our profession. Our wero (challenge) is to do better! Readers, hold us to account.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.