
Abstract
Objectives:
Guided by minority stress theory, we explored the association between sexual identity, justice system involvement, self-harm and suicide attempts, among a cohort of incarcerated adults in Australia.
Methods:
A sample of 2698 adults incarcerated in Queensland and Western Australia were surveyed between 1 August 2008 and 12 August 2016 about their current psychological distress, mental health diagnoses, contact with mental health services, and lifetime and recent self-harm and suicide attempts. We used multivariable logistic regression to explore the relationship between sexual orientation, prior criminal justice system involvement, mental health and demographic factors.
Results:
Five percent of the sample identified as gay, lesbian or bisexual, with 37% of lesbian, gay, bisexual and other same-sex attracted individuals reporting that they had self-harmed (vs 14% of heterosexual peers; χ2 = 52.4; p < 0.001) and 49% reporting a history of at least one suicide attempt (vs 23%; χ2 = 49.2; p < 0.001). Lesbian, gay, bisexual and other same-sex attracted people were 2.1 times (95% confidence interval: [1.4, 3.3]) and 1.8 times (95% confidence interval: [1.2, 2.8]) more likely to report a history of self-harm and suicide attempt, respectively, than non–lesbian, gay, bisexual and other same-sex attracted respondents.
Conclusion:
Intersectionality theory suggests that people who are navigating two or more marginalised identities often experience a compounding of internal and external stressors. Consistent with that theory, lesbian, gay, bisexual and other same-sex attracted people who experience incarceration may be at particularly high risk of self-harm and suicidal behaviour. Custodial settings should both improve cultural competency for frontline staff working with lesbian, gay, bisexual and other same-sex attracted individuals and improve access to mental health services during incarceration.
Introduction
Lesbian, gay, bisexual and other same-sex attracted (LGB+) people are at higher risk of self-harm and suicide than their heterosexual peers (King et al., 2008; Skerrett et al., 2015; Taylor et al., 2019). Although LGB+ people comprise a small minority of the Australian population – approximately 3.5% of the adult population – the Australian Institute of Health and Welfare has designated them as a population at increased risk of health disparities, particularly those related to psychological distress (Australian Institute of Health and Welfare, n.d.; Wilson et al., 2020). Surveys of GB+ people further support these disparities; 5% of Australian GB+ men (compared to 2% of heterosexual men) and 26% of LB+ women (compared to 2% of heterosexual women) reported lifetime self-harm, and 13% of GB+ men (compared to 4% of heterosexual men) and 25% of LB+ women (compared to 5% of heterosexual women) reported a lifetime suicide attempt (Swannell et al., 2016).
Despite these findings, ‘there is nothing inherently “suicidogenic”’ about same-sex attraction (Skerrett et al., 2015: 884). Instead, ‘minority stress’, or the cumulative stress resulting from ongoing exposure to social stigmatisation, prejudice and discrimination, can result in self-loathing, depression, loneliness, self-harm, suicidal ideation or suicide attempts (Swannell et al., 2016).
Minority status and social stigmatisation are often reinforced within society through institutions, most powerfully, the criminal justice system. Through incarceration, fines and labelling (e.g. ‘offenders’), the criminal justice system is uniquely posed to reinforce negative stereotypes about minority groups, including LGB+ people. Same-sex behaviour and relationships have historically been criminalised in Australia and other Western societies (Carroll, 2016). Even today, following the decriminalisation of same-sex attraction, LGB+ people continue to be overrepresented within the criminal justice system. A recent survey of men and women in prisons in Queensland and New South Wales found that over 9% identified as LGB+ compared to 3.5% in the general population (Butler et al., 2012).
Overrepresentation of same-sex attracted people in prisons likely derives from two factors: first, situational same-sex attraction, whereby the deprivation to preferred, opposite-sex partners leads to more people in prison questioning their sexuality and identity (Hensley et al., 2001); second, through that continuing criminalisation of social exclusion. Asquith et al. (2017) introduced the Queer Criminal Career framework to explain this overrepresentation of queer people within the criminal justice system. Their intersectional framework suggests that LGB+ people begin experiencing social exclusion early. As young LGB+ people ‘come out,’ many face rejection from their family of origin and find themselves forced into premature independence. Youth homelessness is especially high among lesbian, gay, bisexual and transgender (LGBT+) young people, and through this experience, they often encounter the adult or youth criminal justice systems within the context of public nuisance crimes (McNair et al., 2017). Drug use, either for self-medication or for participation in queer community, and engagement in illicit labour markets, like sex work, further expose young LGB+ people to criminalisation, arrest and incarceration (Simpson et al., 2019). Once incarcerated, such social exclusion continues. Prisons – and how they are arranged – are situated to uphold rigid gender dichotomies and favour heterosexist norms. LGB+ people whose lives do not conform to these dichotomies and norms encounter ostracism, discrimination and violence, including greater risk of sexual and physical assault while incarcerated (Baćak et al., 2018). LGB+ people already face considerable barriers in securing employment and housing; upon re-entry, the collateral consequences of incarceration make securing these necessities even more difficult (Harvey et al., 2021).
Collectively, these trajectories of social exclusion are illustrative of intersectionality theory – that as one person continue to inhabit multiple marginalised identities, their experiences of disadvantage are compounded and intensified (Crenshaw, 1989). Within public health, researchers have used intersectionality theory as the basis for minority stress theory, to explain how intersectionality can exacerbate inter- and intrapersonal health risks, including self-harm and suicidal ideation among LGB+ people (Brooks, 1981; Meyer, 2003). Previous research has examined the intersections of sexual orientation and race, socio-economic status, and gender identity (Baams et al., 2015; Cyrus, 2017; Lytle et al., 2014); however, minority stress theory frameworks have only recently begun considering incarceration as a type of identity (Harvey et al., 2021).
Like people who identify as LGB+, people who are incarcerated have higher rates of self-harm and suicidal behaviour than age- and gender-matched peers in the general public (Fazel et al., 2011). This elevated risk persists after release from custody (Borschmann et al., 2017; Haglund et al., 2014; Spittal et al., 2014). Among people who are incarcerated, serving a life sentence, being convicted of a violent crime and a history of detention as a juvenile can all increase the risk of self-harm, suicide attempt or suicide (Fazel et al., 2008; Haglund et al., 2014; Hawton et al., 2014; Larney et al., 2012; Spittal et al., 2014; Zhong et al., 2021). Beyond criminal justice–related factors, being male, having a mental health diagnosis and previous self-harm increased the risk of both self-harm and suicide attempt, while being married and being non-White lowered the risk (Borschmann et al., 2017; Fazel et al., 2008; Haglund et al., 2014; Hawton et al., 2014; Spittal et al., 2014; Stewart et al., 2018; Zhong et al., 2021).
The confluence of non-heterosexuality and incarceration status may exacerbate the risk of self-harm and suicidal attempts among LGB+ people who are incarcerated when compared to their heterosexual peers. Therefore, in a cohort of incarcerated people in Australia, we aimed to (1) estimate the prevalence of LGB+; (2) compare the prevalence of psychological distress, self-harm and suicide attempts between LGB+ and heterosexual people; and (3) explore the relationship between LGB+ and incarceration history towards (a) self-harm and (b) suicide attempts.
Methods
Participants
The Health After Release from Prison (HARP) study is a cohort study of 2701 men and women recruited from 12 prisons in Queensland and Western Australia, and followed prospectively through linkage with health and correctional records (Kinner et al., 2018). This paper reports findings from the baseline data, collected before release from prison. Participants were eligible if they were within 6 weeks of expected release from custody (either full discharge or on parole) and were able to provide informed, written consent. Potential participants were excluded if they were under 18 years of age, judged unlikely to be released because of unresolved charges or on remand, had previously participated in the project or if the person was deemed unsafe to interview for mental health or behavioural reasons. Women were intentionally oversampled to permit sex-stratified analyses.
Data collection
Participants completed a face-to-face baseline interview in prison between 1 August 2008 and 31 July 2010 in Queensland and between 1 May 2013 and 12 August 2016 in Western Australia. The survey collected data relating to demographics (including sexual orientation), social history (education engagement, family structure, employment), physical and mental health, self-harm history, substance use and other health-related behaviours.
Trained researchers coded in-prison medical records using the International Classification of Primary Care, Second Edition (ICPC-2) to identify all documented healthcare episodes, and associated diagnoses, during the index incarceration. Prior history of incarceration was obtained through deterministic linkage with correctional records, using a unique prisoner identification number.
The study was approved by the University of Queensland’s Behavioural and Social Sciences Ethical Review Committee (Project #2007000607), the Queensland Corrective Service’s Research Committee, the Queensland Health Human Research Ethics Committee (HREC/11/QHC/40), the University of Western Australia Human Research Ethics Committee (RA/4/20/6492), the Western Australia Department of Health Human Research Ethics Committee (2017/01), the Western Australian Aboriginal Health Ethics Committee (Project #370) and the Australian Institute of Health and Welfare Ethics Committee (EC2012/4/58).
Measures
Sexual orientation
During the baseline interview, participants were asked, ‘Which of the following best describes your sexual identity?’ Options were (1) heterosexual, (2) gay/lesbian, (3) bisexual or (4) other. Those who indicated ‘other’ were asked to provide more information. Sexuality was dichotomised into heterosexuality versus any same-sex attraction (gay, lesbian, bisexual and other).
Justice system involvement
We dichotomised baseline sentence length into those who served ⩽365 days versus 366+ days in custody before release as prior studies have found an increased rate of injury, including self-harm, among those released from shorter sentences (Young et al., 2018). History of juvenile detention was dichotomised, as was whether the index incarceration was a violent crime. Violent crimes were coded on the basis of the Australian and New Zealand Standard Offence Classifications and included any criminal acts within divisions 01-06 (Australian Bureau of Statistics, 2011).
Mental health
The baseline survey included the Kessler Psychological Distress Scale (K10) (Andrews and Slade, 2001). This 10-item Likert-type scale survey explores the presence and severity of anxiety and depressive symptoms in the past 4 weeks and has been widely used and validated (Andrews and Slade, 2001), including among Indigenous people (Bougie et al., 2016). Total scores were classified as low or no psychological distress (10–15), moderate distress (16–21), high distress (22–29) and very high distress (30–50) for descriptive statistics (Andrews and Slade, 2001) and then dichotomised into those with very high distress compared to all others (Australian Bureau of Statistics, 2012). Participants were asked to self-report if they had ever been diagnosed with a mental illness, and if so, the nature of the diagnosis/es. These questions followed the wording from the National Survey of Mental Health and Wellbeing (Australian Bureau of Statistics, 2008).
Self-harm and suicidal behaviour
Participants were asked whether they had ever attempted suicide and/or ever deliberately harmed or injured themselves. If respondents answered yes to either question, they were asked two additional questions: (1) ‘How many times [have you tried to kill yourself/deliberately harmed or injured yourself?’] and (2) ‘How long ago was the last time?’ For this second question, responses were dichotomised into events that happened within the past 12 months versus those that happened more than 12 months ago.
Demographics characteristics
Biological sex (male vs female), age (⩽24; 25–40; 41–60; 61+ years), Indigenous status (Aboriginal, Torres Strait Islander and/or South Sea Islander vs non-Indigenous), years of schooling completed (10th grade or above vs less than 10th grade) and marital status (married or partnered vs not married or not partnered) were included. Age at the time of the baseline interview was calculated from the date of birth obtained from correctional records. All other demographic characteristics were self-reported.
Statistical analysis
Chi-square tests were performed for all categorical demographic, criminal justice system involvement, mental health, and self-harm and suicidal behaviour variables, using sexuality (LGB+ vs heterosexual) as the grouping variable. One-way analyses of variance (ANOVAs) were used when comparing means of continuous variables, including age, number of self-harm episodes and number of suicide attempts. As this population is highly vulnerable, data were suppressed if any one response had fewer than 10 individual respondents.
Tests compared the difference between groups on the basis of sexual orientation (LGB+ vs non-LGB+), whereas multivariable logistic models were constructed based on previous research showing factors associated with self-harm or suicide attempts (Borschmann et al., 2017; Fazel et al., 2008; Haglund et al., 2014; Hawton et al., 2014; Larney et al., 2012; Spittal et al., 2014; Young et al., 2018; Zhong et al., 2021). These variables included sexual orientation and all criminal justice variables (sentence length, violent crime and juvenile record). In addition, the models were adjusted for demographic characteristics (sex, Indigenous status, age, marital status and educational attainment) and mental health factors (psychological distress as measured by K10 and the history of mental health diagnosis). The model on suicide attempts was additionally adjusted for previous history of self-harm. All statistical analyses were carried out in Stata 14 (College Station, TX, USA).
Results
Sexual orientation
The final sample included 2698 individuals; three respondents were excluded from the final sample as their sexual orientation was not recorded. Five percent (n = 133) identified as LGB+, with the majority of these (n = 84; 63%) identifying as bisexual. Non-heterosexuality was more common among women, with 12% (n = 65) of all female respondents indicating that they were bisexual, and a further 5% identifying as lesbian (n = 26). Conversely, more male respondents identified as gay (1.1%; n = 23) than bisexual (0.9%; n = 19) (Supplemental Material Table S1).
Justice system involvement and demographic characteristics
The typical respondent in the sample was male, aged 26–40 years, had left school before 10th grade and was not married (Table 1). Thirty-six percent identified as Aboriginal and/or Torres Strait Islander. Half had been convicted of a violent crime and were sentenced to less than a year in prison. Two-thirds had been incarcerated at least once prior to their index incarceration, and 62.0% had a prior history of youth detention (Table 1). There was no significant difference between LGB+ and heterosexual respondents with respect to justice system involvement or demographic characteristics, with the exception of sex. Findings using a trichotomised version of the sexuality variable (lesbian/gay vs bisexual vs heterosexual) were similar (Supplemental Material Table S2).
Demographic characteristics by sexual orientation.
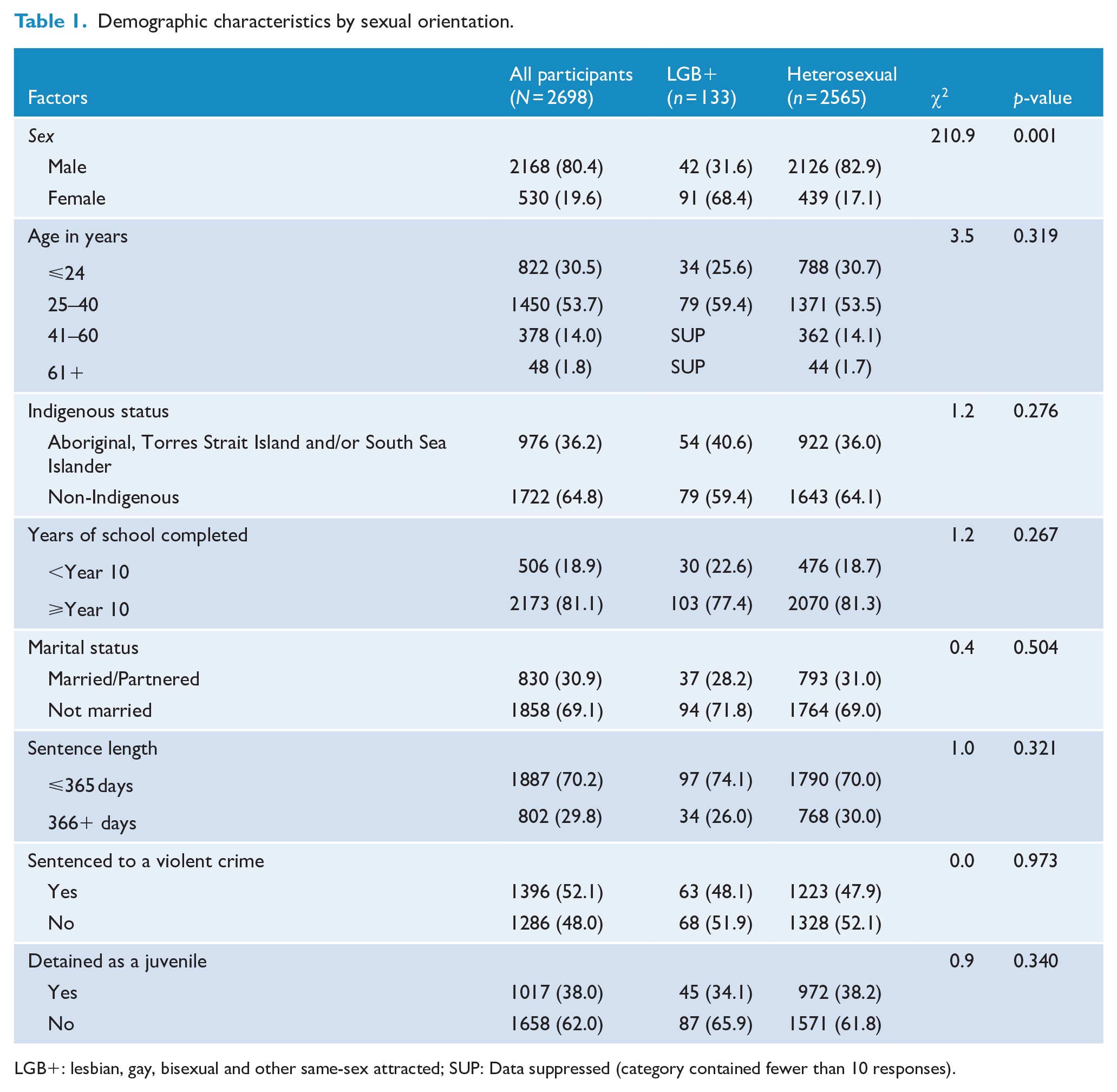
LGB+: lesbian, gay, bisexual and other same-sex attracted; SUP: Data suppressed (category contained fewer than 10 responses).
Mental health, self-harm and attempted suicide
Compared to heterosexual peers, LGB+ respondents reported poorer mental health. They were more likely to report high or very high levels of psychological distress (51.1% LGB+ vs 32.0% heterosexual; χ2 = 20.9; p < 0.001) and twice as likely to report having a diagnosed mental illness (65.4% vs 34.6%; χ2 = 23.8; p < 0.001).
LGB+ participants were more likely to report histories of self-harm and suicidal behaviour; 37.1% (vs 14.0% of heterosexual respondents; χ2 = 52.4; p < 0.001) indicated that they had deliberately injured or harmed themselves in the past and 49.2% (vs 22.5% of heterosexual respondents; χ2 = 49.2; p < 0.001) indicated that they had attempted suicide. Among those who reported histories of self-harm and/or suicidal behaviour, LGB+ respondents also reported a greater number of episodes, and that such episodes had occurred more recently than their heterosexual peers (Table 2). Bisexual respondents were significantly more likely than lesbian or gay respondents to report self-harm (45.8% bisexual vs 22.5% lesbian/gay; χ2 = 7.2; p < 0.007) but not more likely to report suicidal behaviour (Supplemental Material, Table S3).
Mental health and self-harm histories, by sexual orientation.
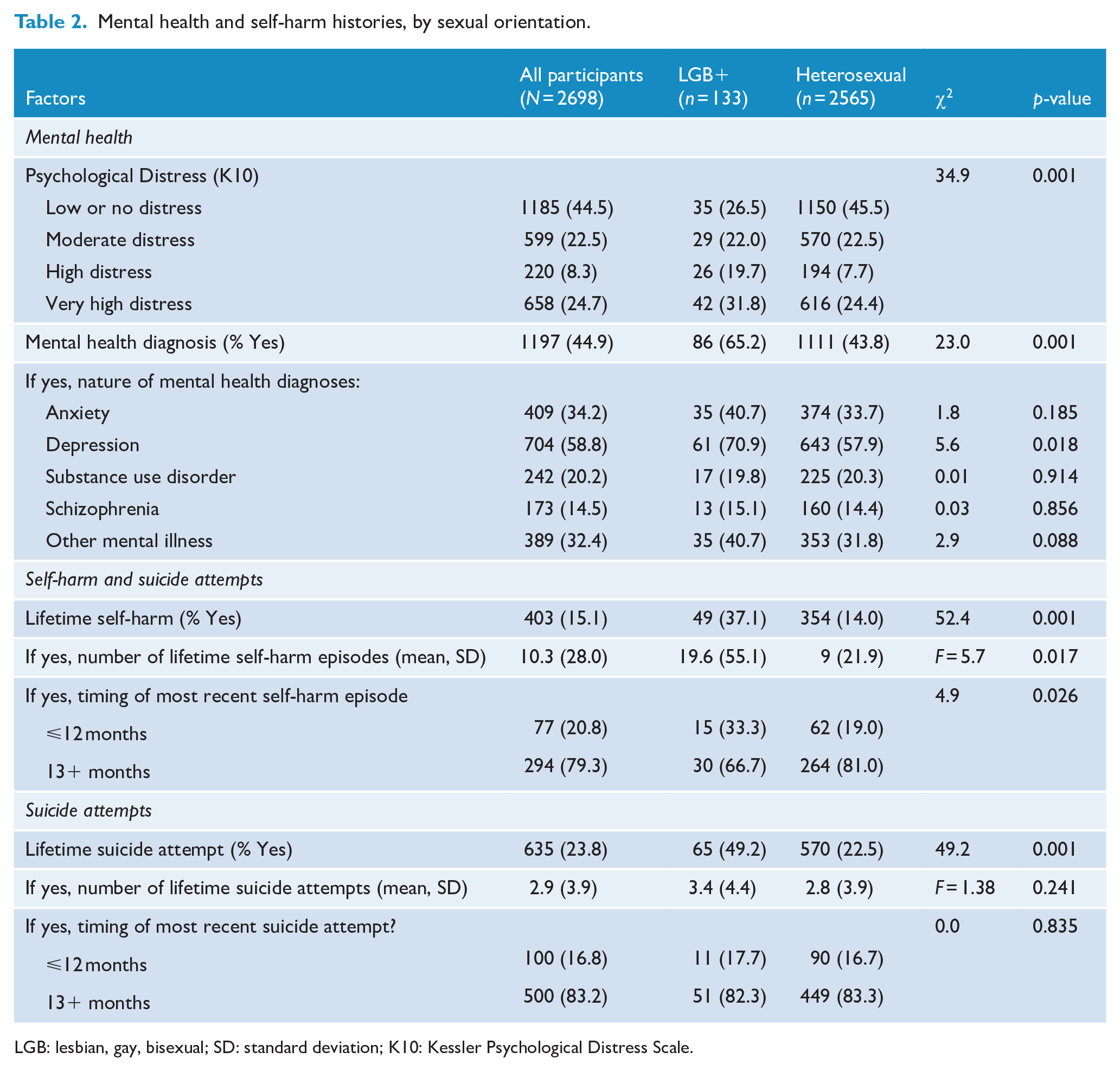
LGB: lesbian, gay, bisexual; SD: standard deviation; K10: Kessler Psychological Distress Scale.
Factors associated with self-harm and suicide attempt
After adjusting for covariates, LGB+ people had greater odds of both self-harm (adjusted odds ratio [aOR]: 2.2; 95% confidence interval [CI]: [1.4, 3.3]) and suicidal behaviour (aOR: 1.8 times; 95% CI: [1.2, 2.8]) (Table 3). The odds of self-harm were also higher among women, those who had been convicted for a violent crime, those who had been incarcerated as a juvenile, those who reported a history of mental illness and those who reported high or very high levels of psychological distress. Similarly, the odds of reporting a suicide attempt were greater for people aged 41–60 years, those with a history of juvenile incarceration, those with a history of self-harm, those with mental health diagnosis and those reporting high or very high levels of psychological distress.
Logistic models of factors associated with self-reported self-harm and attempted suicide among Australians who are incarcerated.
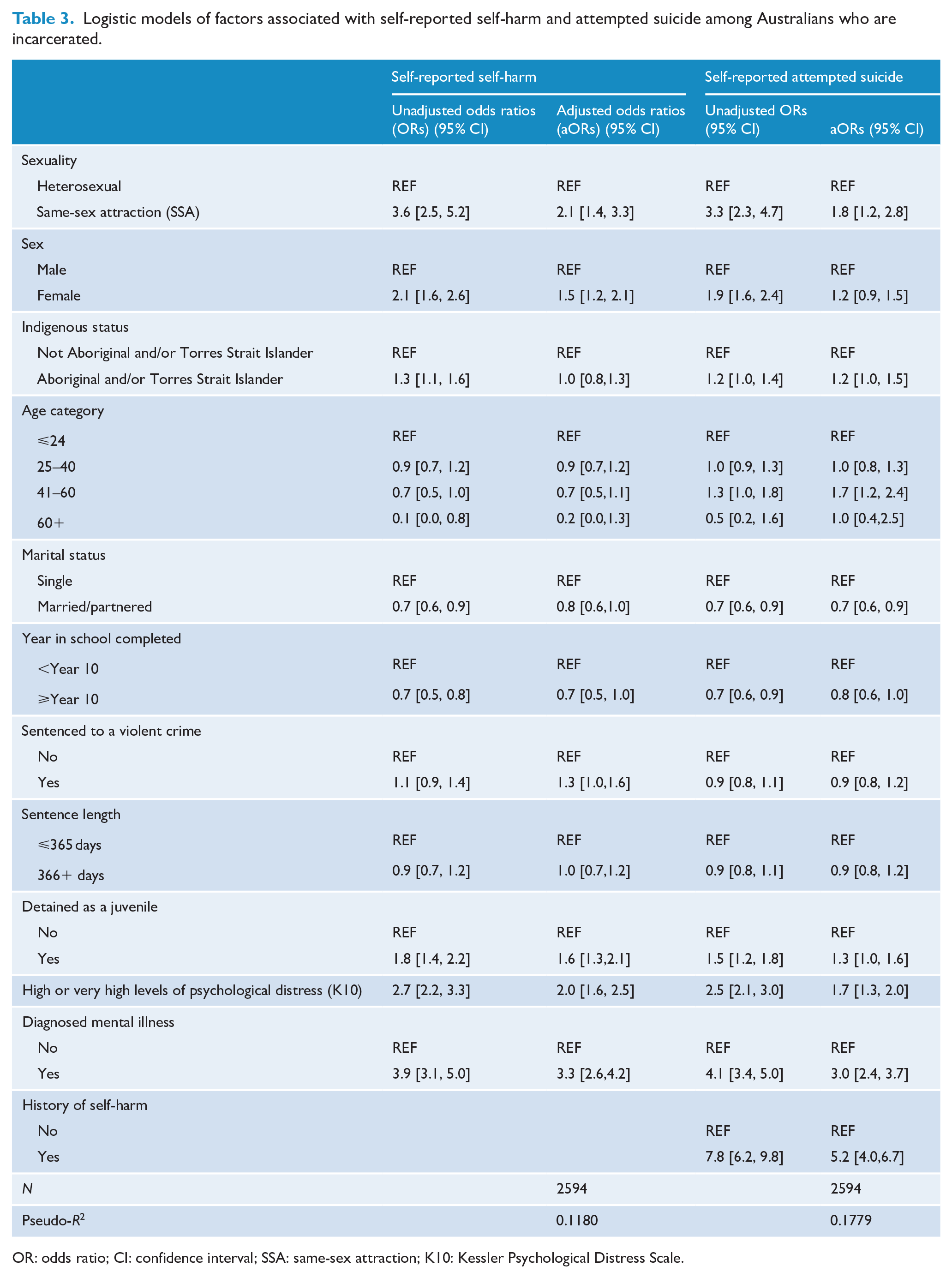
OR: odds ratio; CI: confidence interval; SSA: same-sex attraction; K10: Kessler Psychological Distress Scale.
Discussion
Despite comprising 5% of our sample, LGB+ respondents who were incarcerated in this study accounted for 12% of those with a history of self-harm and 10% of those with a history of suicide attempt. After adjusting for covariates, LGB+ people in prison had approximately twice the odds of having engaged in self-harm or suicidal behaviour, compared with their heterosexual peers.
This study also lends some support for investigations into the overrepresentation of LGB+ people in prison; between 3% and 4% of all adults within Australia identify as LGB+ (Wilson et al., 2020). The 5% reported here, then, is higher than the proportion of LGB+ people estimated within the general Australian population though smaller than the 9% of LGB+ people found in a previous survey of prisoners (Butler et al., 2012). Butler and colleagues’ findings were in part driven by the larger proportion of men who identified as bisexual (3.1% Butler vs 0.9%) and another 2% of respondents who identified as ‘queer/other’. This additional option, as well as the computer-assisted interview format, may have led to more respondents – especially men – feeling more comfortable identifying as same-sex attracted. Despite our efforts to create a safe, confidential and non-judgemental space for interviews, we expect that reporting of LGB+ status is underestimated within this sample.
In addition, our interview script focused on sexual identities – not behaviour or even attraction. Other surveys that have asked about general attraction and behaviour have identified an even larger proportion of people in prison who acknowledge same-sex attraction without claiming such identities (Richters et al., 2012, 2014) For example, in the Butler et al. (2012) study, 63% of women in prison identified as heterosexual, but 41% reported only have sexual experiences with the opposite sex. Identifying as gay, lesbian or bisexual may be especially difficult in prison; identity rather than behaviour has emerged as a strong indicator of in-prison abuse (Harvey et al., 2021; Meyer et al., 2017). LGB+ people face a greater risk of verbal, sexual and physical assault in prison than either heterosexual peers or peers who have same-sex relations (e.g. men who have sex with men; women who have sex with women) (Harvey et al., 2021; Meyer et al., 2017). Such abuse may serve as a precursor for the psychological distress, self-harm and suicidal behaviours documented here.
Incarceration itself, then, can present additional external and internal stressors, including risk of assault, separation from family and friends, deprivation and loneliness. We hypothesised that the intersection of these two marginalised identities –sexual minority status and incarceration – may lead to a greater likelihood of self-harm and suicidal behaviour than either identity on its own, as suggested by intersectionality and minority stress theory. To that end, our hypothesis was supported; approximately one-third of LGB+ people who were incarcerated had self-harmed and one-half had attempted suicide. This is substantially higher than the 8% (self-harm) and 5% (suicide attempt), respectively, reported by the broader Australian general public (Martin et al., 2010) and also higher than the finding that 5% of Australian GB+ men and 26% of Australian LB+ women, respectively, had self-harmed, and 13% and 25% had made a suicide attempt in their lifetime (Swannell et al., 2016). Along the other axis, three previous Australian studies found that between 18% and 37% incarcerated adults had self-harmed over their lifetime and between 21% and 47% had reported a suicide attempt (Butler et al., 2018; Larney et al., 2012; Stewart et al., 2018). Within the context of this literature, our findings suggest that LGB+ people who are incarcerated are reporting much higher prevalence of self-harm and suicide attempts than LGB+ respondents within the general public, and that our results are at the high end of previous studies involving people who are incarcerated.
In addition, consistent with previous studies (Li et al., 2013; McLean, 2008; Taylor et al., 2019), we found that bisexual respondents were more likely than their lesbian and gay peers to report recent self-harm. Compared to Taylor and co-authors’ recent survey of bisexual Australians in the general public, our sample was less likely to report lifetime self-harm (45.8% here vs 58.7%, Taylor et al., 2019) but almost twice as likely to report a suicide attempt (50.6% vs 27.8%). This finding is worthy of more investigation; many studies, including this one, have grouped bisexual people in with lesbian and gay respondents in response to concerns over statistical sensitivity. Yet bisexual people face rejection, biphobia, and constantly needing to assert and defend their queerness within both communities (Li et al., 2013; McLean, 2008). Qualitative research that focuses exclusively on bisexual people and their experiences in prison may help to further illuminate this finding.
The risk of self-harm and suicide attempt among LGB+ people who are incarcerated may also underscore how traditional solutions to address poor mental health may not be appropriate in all settings. Until recently, the prevailing public health logic has been that coming out ultimately improves mental health in the long-term (Morris et al., 2001). More recent research, though, questions those assumptions, suggesting that these benefits only occur if there are strong, safe support systems (van der Star et al., 2019). Prisons are unlikely to provide such an environment; in their work on LGB+ men’s decisions to ‘come out’ while incarcerated, Yap and colleagues found that coming out resulted in verbal and physical abuse. LGB+ men instead often made the decision to withdraw from broader prison communities, stay closeted or engage in sexual relationships for protection (Yap et al., 2020). Many described that these decisions further exacerbated loneliness and stress. When LGB+ men revealed their sexuality to prison staff, they were often moved into protective units, reducing their access to programming, visits, and generating unwanted attention and stigmatisation. Serving time in protective units, particularly those that resemble solitary confinement, can also contribute to poor mental health and self-harm (Cloud et al., 2014; Kaba et al., 2014). Thus, returning to the closet may be an unfortunate risk mitigation strategy that LGB+ people use to exert some control over their incarceration (e.g. electing to serve their time in the general population). Future research should consider not only LGB+identity, but also ‘outness’ and social support when examining mental health, self-harm and suicide risk.
Although our study engages an intersectional lens to examine sexual orientation and incarceration, we also wish to note this examination is incomplete. We have primarily focused only on one axis of identity – sexual orientation. While we have employed an intersectional framework, we have not considered how additional identities or experiences of marginalisation, namely, cultural heritage (including race or ethnicity) or gender, may further exacerbate or mitigate our findings. Both Aboriginal and/or Torres Strait Islander people and women were overrepresented among LGB+ respondents within this study. Community-based research has found that additional experiences of marginalisation can increase risk of poor mental health, with young, queer people of colour being more likely than their White peers to report suicidal ideation and self-harm (Cyrus, 2017; Lytle et al., 2014). Similar studies that focus on gender have found similar patterns with regard to greater proportions of LGB+ women and trans and gender-diverse people reporting self-harm, attempted suicide and psychological distress than their heterosexual counterparts (Gorden et al., 2017; Hout et al., 2020). However, Australian research on these issues, both in the general public (Treharne et al., 2020) and in prison (Wilson et al., 2017), is limited. Further research that considers cultural background and gender as additional axes of identity is needed.
Limitations
While this study is among the first quantitative studies to look at the experiences of incarcerated LGB+ people and their mental health, there are several limitations of note. First, as noted, this study focuses on identity rather than behaviour or attraction; we acknowledge that this is a limitation. Future surveys should incorporate questions that better capture human sexuality, including comparisons on the basis of behaviour as well as identity (e.g. men who have sex with men/women who have sex with women vs LGB+ vs heterosexual respondents). Second, the study design was cross-sectional. Longitudinal or qualitative timelining research on the experiences of LGB+ people in prisons and following release would be especially useful in constructing interventions. Third, as noted, our study does not comment or consider the role of cultural background (including race and ethnicity) and/or gender on our findings. With regard to gender, we recommend that future surveys adopt the multi-tiered questions about gender and sexuality, as recommended by the Australian Bureau of Statistics, to allow more consideration of the unique experiences of sexual minorities, intersex, and trans and gender-diverse people (Australian Bureau of Statistics, 2021).
Conclusion
Same-sex attracted people who are incarcerated are at an increased risk of self-harm and suicidality. Once incarcerated, LGB+ people face two types of marginalisation, arising both from their identity as a gay, lesbian or bisexual person and from their status as a person who is incarcerated. Cumulatively, navigating these identities may lead to an increase in the likelihood of self-harm and suicide attempts. However, research suggests prisons are not safe places for LGB+ people to be ‘out’, the solution that is often recommended to address self-harm and suicide risks. Beyond merely improving access to mental health services, prisons need to develop cultural competency among their staff on the basis of sexuality (Gorczynski, 2021; Herbert, 2020). Such programming should emphasise how social stigma can contribute to an increased risk in mood disorders, self-harm and suicide risk. By improving mental health services and developing safer environments where LGB+ people are empowered in their decision to disclose their sexuality, correctional environments may serve as an opportunity to connect to services rather than environments that further harm.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221104744 – Supplemental material for Self-harm and suicide attempts among incarcerated lesbian, gay and bisexual people in Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674221104744 for Self-harm and suicide attempts among incarcerated lesbian, gay and bisexual people in Australia by Katie Hail-Jares, Craig Cumming, Jesse T Young, Rohan Borschmann, Nick Lennox and Stuart A. Kinner in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The author(s) wish to thank Professor David Preen for his input and involvement in this project and early drafts of the manuscript. They also wish to acknowledge and thank the many people who participated in this research project. The findings and views reported in this article are those of the authors and should not be attributed to the governments or departments involved in the research. Any errors of omission or commission are the responsibility of the authors. Thank you to the people of Western Australia and Queensland for the use of their administrative data in this research. The authors also wish to thank the staff at the Western Australian Data Linkage Branch, the Department of Justice and the Department of Health; the Queensland Corrective Services and Queensland Health; and the Australian Institute of Health and Welfare.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: J.Y. receives salary and research support from a National Health and Medical Research Council Investigator Grant (GNT1178027). S.K. receives salary support from National Health and Medical Research Council Senior Research Fellowship APP1078168.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Passports project was funded by the National Health and Medical Research Council (Award Nos ACPP409966 and APP1002463).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.