
Abstract
Objective:
Attention-deficit/hyperactivity disorder affects over 5% of children and is characterised by a persistent pattern of problems with focussing or maintaining attention and/or hyperactivity-impulsivity. The censusADHD Study is a richly phenotyped nationwide cohort of Australian children with attention-deficit/hyperactivity disorder. The overarching aims of the study are to examine attention-deficit/hyperactivity disorder medication utilisation patterns and treatment response, the impact of children’s attention and behavioural problems on caregivers, and costs related to attention-deficit/hyperactivity disorder.
Methods:
Families of potential attention-deficit/hyperactivity disorder cases aged between 6 and 11 years were identified using Pharmaceutical Benefits Scheme prescription records for attention-deficit/hyperactivity disorder medications held by Services Australia and sent a study information letter. Data were collected from 1574 primary caregivers via online survey in 2015, including the behavioural profile of the child, the child’s medication use and experiences with side effects and the impact of the child’s behaviour on the caregiver. Approximately 81% of caregivers also consented to record linkage of the child’s Pharmaceutical Benefits Scheme and Medicare Benefits Schedule claims to directly assess prescription dispensing history and health service usage to estimate costs to the family and Medicare health system.
Results:
Boys were diagnosed with attention-deficit/hyperactivity disorder earlier (p = 0.021), more likely to present as the combined and predominantly hyperactive subtypes (p = 0.001) and at higher risk of experiencing a school suspension (p < 0.001) or expulsion (p = 0.043). Overall, children presenting as the combined subtype had higher rates of psychiatric comorbidities (p < 0.001). Finally, prescription costs for each family and the Pharmaceutical Benefits Scheme significantly increased in the year following attention-deficit/hyperactivity disorder diagnosis (p < 0.001).
Conclusion:
Research examining the psychosocial and financial impact of attention-deficit/hyperactivity disorder on Australian children and their families is needed. Our findings demonstrate the importance of examining both gender and attention-deficit/hyperactivity disorder subtype presentation in future studies.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurodevelopment disorder in children and is characterised by a persistent and developmentally inappropriate pattern of inattention and/or hyperactivity-impulsivity which interferes with functioning or development (American Psychiatric Association, 2013). In 2013–2014, the 12-month prevalence of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994) ADHD in Australian children aged 4–11 years was almost double among boys (9.8%) compared with girls (5.4%) (Lawrence et al., 2015). Approximately 50% of children with ADHD will go on to suffer from other psychiatric disorders (Quinn, 2008; Taurines et al., 2010) with high levels of comorbid conduct disorder (CD) and oppositional defiant disorder (ODD), and depression, anxiety, substance use and eating disorders (Erskine et al., 2016; Gillberg et al., 2004; Quinn, 2008) later in life.
In Australia, the treatment and management of ADHD are predominantly undertaken by paediatricians (Chow et al., 2014); approximately 92% of patients with ADHD receive treatment under the care of a paediatrician rather than a psychiatrist or general practitioner (Preen et al., 2008). Current international guidelines recommend multimodal approaches that include pharmacological and psychosocial interventions for the management of ADHD (Coghill et al., 2021). While a number of pharmacological treatments are available and improve outcome, they leave patients with significant residual disability and have a number of undesirable side effects, including insomnia and growth restriction (Faraone et al., 2008). Although ADHD medications are the least prescribed class of psychotropic drugs in Australia (Stephenson et al., 2013), the prevalence of ADHD medication use among Australian children aged 3–18 years has increased between 2001 and 2015 (Raman et al., 2018). Nonetheless, while almost two-thirds of children and adolescents with ADHD in the United States take medication (Wolraich et al., 2019), only ~17–30% of Australian children diagnosed with ADHD are prescribed medication (Charles et al., 2011; Lawrence et al., 2015; Stephenson et al., 2013). As might be expected, symptom severity and parental attitudes towards ADHD/stimulant medication are the primary predictors of pharmacological treatment (Monastra, 2005). Barriers to pharmacological intervention include comorbid diagnoses and financial burden of treatment (Corkum et al., 2015). In the period from 2012 to 2015, more than 135,000 and 500,000 prescriptions, on average, were written per calendar year for the two most commonly prescribed ADHD medications in Australia (dexamphetamine and methylphenidate, respectively). The prescription of these medications requires authorisation from Medicare Australia, and until 2005, dexamphetamine was the only Pharmaceutical Benefits Scheme (PBS)-listed medication for ADHD.
Direct healthcare costs associated with ADHD treatment and sequelae represent significant long-term economic consequences. There is also substantial economic burden driven by education and caregiver costs, including caregiver strain (Schein et al., 2022). A retrospective study (Deloitte Access Economics, 2019) examining the financial and non-financial costs of ADHD in Australia in both children and adults reported the total socio-economic costs to be $20.42 billion ($25,071 per person with ADHD) in 2019. The majority (81%) of the $12.83 billion economic costs were associated with productivity losses. Overall, total health system costs due to ADHD ($810 million) were estimated to be $1000 per individual with ADHD. In addition, total loss of well-being costs were reported to be $7.59 billion ($9394 per person). A previous study focusing on Australian children aged 4–9 years demonstrated significant excess health care costs associated with ADHD from an early age; the total Medicare Benefits Schedule (MBS) and PBS costs in 2012 associated with ADHD were estimated to be $24.7–$30.0 million dollars over 6 years (Sciberras et al., 2017).
The censusADHD Study established a nationwide cohort of 1574 Australian children living with ADHD. The overarching aims of the study are to (1) investigate the impact of children’s attention and behavioural problems on the emotional and psychological well-being of primary caregivers, (2) examine ADHD medication utilisation patterns and treatment response and (3) provide estimates of the direct and indirect financial costs related to ADHD in the Australian context. This article describes the design of the censusADHD Study and characteristics of the sample and summarises data collected on ADHD subtype presentation, psychiatric comorbidities, indicators of learning difficulties, ADHD medication use and caregiver stress.
Methods
Study design and ethics
The censusADHD Study used the mail-out service of Services Australia to recruit primary caregivers of children who had been prescribed ADHD medication. Prospective participants were identified by the Services Australia based on PBS prescription records using a query that was defined by the researchers. Recruitment letters describing the study and providing a URL link for the Study Information and Consent pages were sent in June 2015 by Services Australia to 25,920 primary caregivers of all Australian children born between 1 January 2004 and 31 December 2008 (children aged 6–11) who had been dispensed three or more prescriptions for ADHD medications in the past 5 years.
The researchers did not receive any information about who the letters were sent to or how many of the letters were undeliverable. Families with multiple children meeting criteria only received a letter regarding their eldest child. Prescriptions for the following medications were selected to identify potential participants: methylphenidate (PBS Item Codes 2172H, 2276T, 2280B, 2283E, 2387P, 2388Q, 2432B, 3440C, 8839F), dexamphetamine (1165H), modafinil (8816B) and atomoxetine (9092M, 9093N, 9094P, 9095Q, 9096R, 9289X, 9290Y). In Australia, these medications can only be prescribed by psychiatrists and paediatricians and require authorisation by Medicare Australia. Prescriptions that do not meet the requirements for authorisation are not part of the PBS database.
Ethics approval for all aspects of the project was obtained from the QIMR Berghofer Medical Research Institute Human Research Ethics Committee (P1517). In addition, the Study mail-out and access to participant MBS and PBS data were also approved by the Services Australia External Request Evaluation Committee (EREC Reference No. MI1273). The Helsinki Declaration and applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during all the phases of this research.
Online survey
Data were collected from June to September 2015. Caregivers (n = 1574) gave self-reported responses to a series of online questionnaires relating to themselves and the index child. Caregivers provided information about their child’s behaviour, treatment history, medication effectiveness and side effects, education history and performance. The child behaviour section collected parental reports of ADHD under two scenarios: (1) when the child was not taking medication or being treated for ADHD using the Vanderbilt ADHD Diagnostic Parent Rating Scale (VADPRS; Wolraich et al., 2003) and (2) when the child was taking medication or being treated for ADHD using the Strengths and Weaknesses of ADHD Symptoms and Normal Behaviour Rating Scale (SWAN; Swanson et al., 2012). The VADPRS is an ADHD rating scale that comprises 18 items corresponding to DSM-IV ADHD diagnostic criteria. Caregivers indicated the frequency of 18 ADHD behaviours (items 1–18), considered in an age-appropriate context, on a 4-point scale (0 = never, 1 = occasionally, 2 = often, 3 = very often) and the functional impairment of these behaviours on eight performance items (items 48–55) using a 5-point Likert-type scale (1 = excellent, 2 = above average, 3 = average, 4 = somewhat of a problem, 5 = problematic). A child was considered to have ADHD if the caregiver endorsed a score of 2 or 3 on at least 6 symptoms on the inattention subscale (items 1–9), at least 6 symptoms on the hyperactive/impulsive subscale (items 10–18) or met both of these conditions.
Additional VADPRS subscales screen for DSM-IV ODD (items 19–26) and CD (items 27–40). Of note, item 40 (‘Has forced someone into sexual activity’) was excluded in the censusADHD survey. VADPRS items 41–47 screen for anxiety and depression symptoms. The VADPRS instrument is well validated, has good internal consistency for each subscale (α > 0.90) (Anderson et al., 2022; Bard et al., 2013; Wolraich et al., 2013) and correlates (r = 0.79) with the total ADHD score of the Computerized Diagnostic Interview Schedule for Children (Wolraich et al., 2013).
Data on autistic spectrum disorder (ASD) were collected using a standard screening questionnaire (10-item Autism Spectrum Quotient [AQ10]; Allison et al., 2012). Caregivers completed the Disruptive Behavior Stress Inventory (DBSI; Johnson and Reader, 2002) which assesses the frequency and severity of 40 child behaviour–related stressors experienced by parents of children with ADHD. The stressors comprised family-related events, changes, hassles and disruptions. Caregivers responded yes (1) or no (0) to each item to indicate if they had experienced the stressor in the past 6 months. For any yes response, a rating of the degree of stress associated with the stressor was provided on a 4-point Likert-type scale (0 = not at all stressful, 1 = somewhat stressful, 2 = moderately stressful, 3 = very stressful) while the degree of stress for no responses was rated 0. The yes/no responses across the 40 items are summed into a Stress Experience score (range = 0–40) and a Stress Degree score is calculated by summing the stressfulness ratings (range = 0–120). Caregivers also provided information about the impact of their child’s behaviour on their financial, emotional and occupational well-being. Figure 1 provides an overview of the censusADHD study and Supplemental Table S1 summarises the instruments used in the survey.
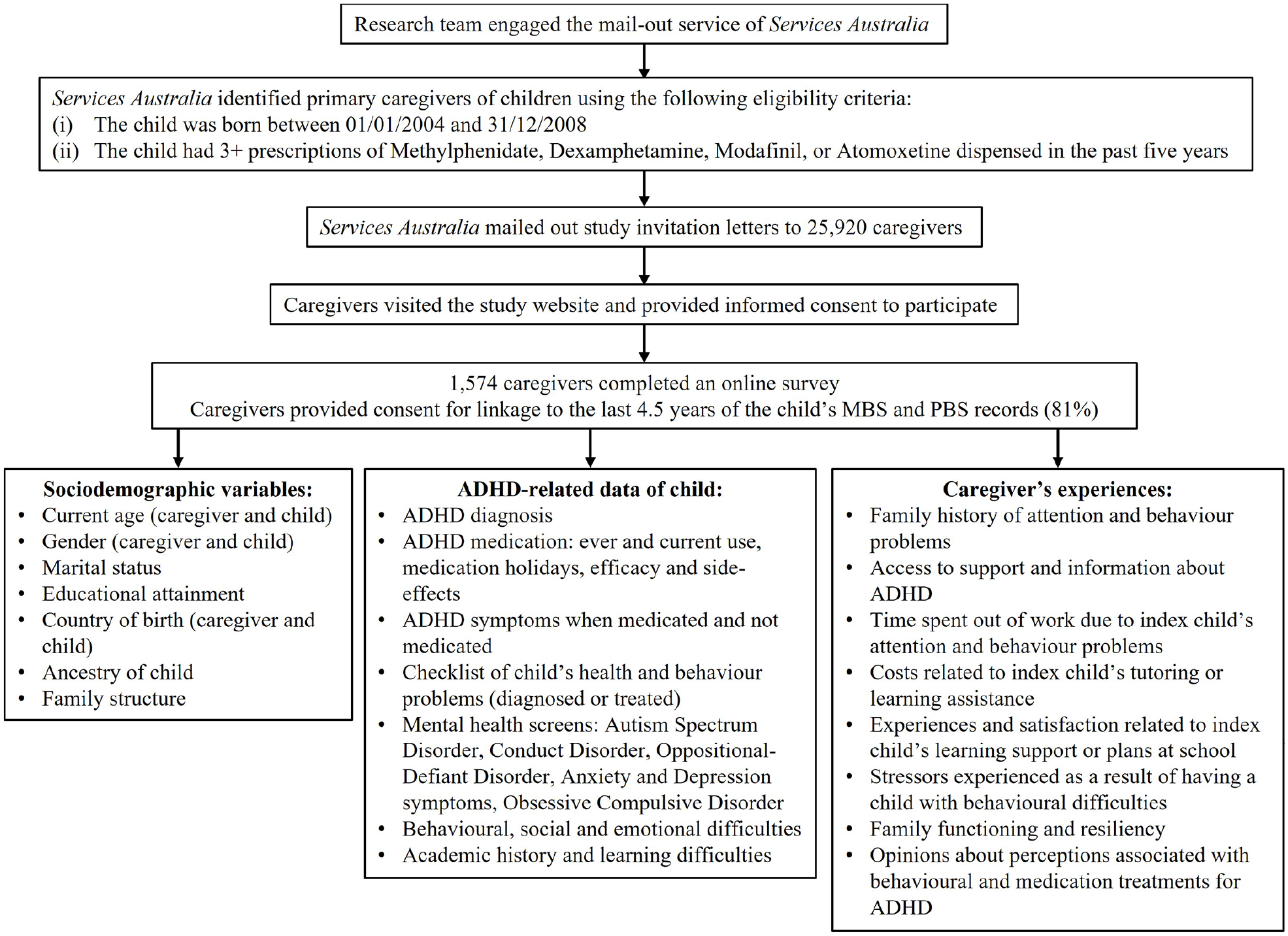
Overview of the censusADHD Study recruitment strategy and data collected.
Data linkage
Caregivers were asked to give consent to allow the study to access the child’s PBS and MBS records to directly assess prescription dispensing history and health service usage and to estimate costs to the family and Medicare health system. For those children for whom we have received caregiver consent (n = 1278), approval was requested in 2017 for linkage to their electronic PBS and MBS records held by Services Australia. The PBS and MBS are the mechanisms by which the Australian government subsidises the cost of medicines and health services, respectively, and the research databases contain records for most Australians for the past 4.5 calendar years. PBS data contain records of pharmacy transactions for all drugs listed on the PBS schedule and dispensed to eligible Medicare card holders. MBS data contain records of health services, Medicare service provider identifiers, diagnostic procedures and tests provided outside of the hospital setting. Both databases use a unique coding system that can be searched. Overall, these records are a rich source of health care utilisation and cost data (to the family and the Medicare health system), providing the costs to government and to the individual for each prescription and health service within the specified data extraction window (1 January 2012–1 March 2015).
Linkage of these data with the information from the online survey will allow investigation of the direct financial costs related to ADHD treatment in the Australian context. Pharmaceutical prescription records also provide a means to validate caregiver-reported ADHD medication use by the child.
Statistical analyses
Data quality control and basic statistical analysis, including descriptive statistics analysis, were conducted using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). Significance of differential responses between participants with caregiver stress and healthcare utilisation was assessed using Student’s t tests and chi-square tests. Association between consent to PBS and MBS record linkage and traits including the age and sex of the caregiver and child, educational attainment of the caregiver and the ADHD subtype presentation of the index child was assessed using chi-square tests.
Results
The majority of the 1574 primary caregivers were the child’s mother (87%), 36% of caregivers had university degrees and the average age of caregivers was 40.6 ± 7.1 (range = 25–73) years. Demographic characteristics of the caregivers across ADHD diagnoses of the index child are provided in Supplemental Table S2. Educational attainment levels (74.2% with a post-school qualification) were higher than that observed in the Australian census data (67.4%) (Australian Bureau of Statistics, 2015), indicating that caregivers with higher education levels were more likely to participate in the study.
Caregiver stress
The mean Stress Experience and Stress Degree scores of caregivers were 21.0 ± 9.7 and 46.1 ± 28.5, respectively. Female caregivers reported significantly higher levels of stress than male caregivers on both the Stress Experience (p = 0.012) and Stress Degree (p = 0.003) scales. Consistent with findings observed in the Johnson and Reader’s (2002) study, a significant effect of the child’s ADHD subtype presentation on the Stress Experience, F(3, 1465) = 71.0, p = 7.5E-43, and Stress Degree, F(3, 1465) = 76.7, p = 4.5E-46, scales was found. Overall, caregivers of children with combined ADHD subtype showed higher levels of stress (Stress Degree mean score = 52.3 ± 27.9) than caregivers of children with hyperactive (39.0 ± 23.4), inattentive (33.2 ± 23.9) and sub-threshold symptom (20.4 ± 21.1) subtypes. A similar pattern was observed for the Stress Experience score.
Data linkage
Overall, 1278 caregivers (81%) consented to the study accessing their child’s PBS and MBS records. Overall, data linkage was obtained for ~93% of these children; errors in data provided by caregivers resulted in 7% of consent forms being rejected. PBS and MBS data linkage was obtained for 1195 and 1184 children, respectively, resulting in 1021 children with both MBS and PBS records, 21 children with MBS records only and 64 children with PBS records only in the data extraction window.
The likelihood of a caregiver consenting to PBS and MBS record linkage was significantly associated with combined annual household income (p = 3.96E-11) whereby caregivers who chose not to answer the question about their annual household income were less likely to provide consent for record linkage. The index child’s ADHD subtype presentation was also associated with the likelihood of caregiver consent (p = 0.016); caregivers of children with sub-threshold ADHD symptoms were significantly less likely to provide consent (Supplemental Table S3).
The majority of index children were male (78.0%), born in Australia (93.8%) and aged between 6 and 11 years (9.5 ± 1.3 years) (Table 1). The ethnicity/ethnicities of the index child was provided by caregivers who were asked to describe the geographic region(s) where the child’s ancestors came from using a prompt list of 20 regions; the ethnicity of the children was 92.7% Caucasian, 7.6% Australian Aboriginal and/or Torres Strait Islander peoples, 4.0% Eastern and South Eastern Asian, 3.0% Māori and Pacific Islander, 1.2% South Asian ethnicity, 1.7% Middle Eastern, 1.8% African and 0.8% American First Nations. Due to the strict regulation of ADHD medication prescribed through the PBS system, the vast majority of children (93.6%) meet full criteria for DSM-IV ADHD according to caregiver responses on the VADPRS (Wolraich et al., 2003), with the remaining 6.4% showing a high level of ADHD symptoms but not meeting full criteria.
Basic demographic, ADHD diagnosis and selected characteristics of index children across gender.
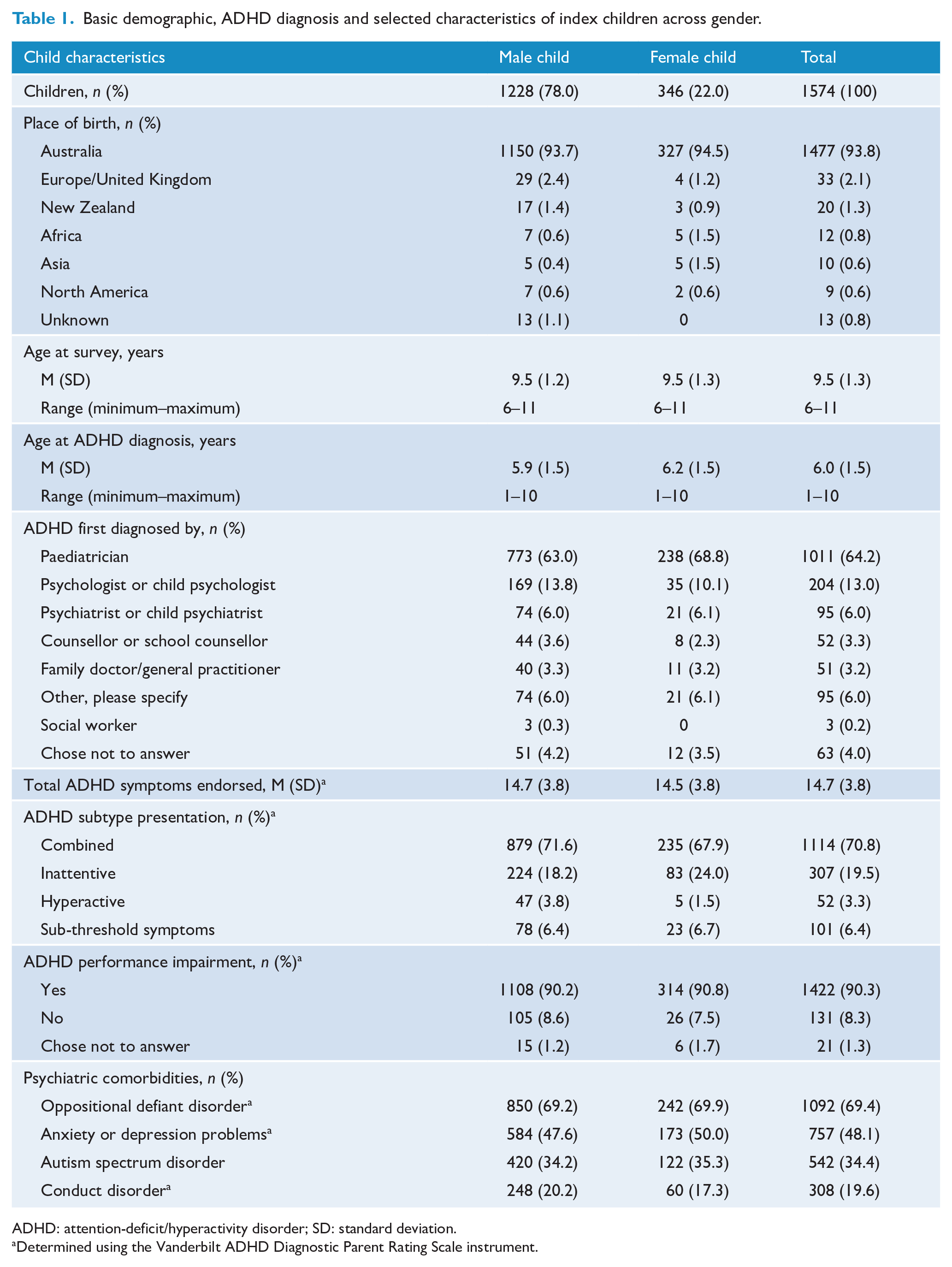
ADHD: attention-deficit/hyperactivity disorder; SD: standard deviation.
Determined using the Vanderbilt ADHD Diagnostic Parent Rating Scale instrument.
Of the 1334 families with two or more children, 25.3% reported having more than one child with ADHD. A history of childhood ADHD or attention problems was also reported for 27.8% of the mothers and 33.1% of the fathers, and almost 1 in 4 children (22.8%) had at least one parent with a lifetime history of ADHD and both parents for 2.4% of children. Furthermore, ADHD severity, as indexed by VADPRS symptom score, was higher (p = 0.002) for children who had one or more parents with a history of ADHD (15.2 ± 3.5 symptoms) versus those whose parents reported no history of ADHD (14.5 ± 3.8 symptoms).
ADHD subtype presentation
Overall, the majority of children (70.8%) presented with combined ADHD subtype, followed by predominantly inattentive (19.5%) and predominantly hyperactive (3.3%). Of note, ADHD subtype presentation differed between boys and girls (p = 0.021), with boys more likely presenting as the combined and predominantly hyperactive subtypes (Table 1).
ADHD diagnosis
Approximately 85% of the children were diagnosed with ADHD by the age of 7. The mean age at ADHD diagnosis was approximately 5 months earlier (p = 0.001) among boys (5.9 years) than girls (6.2 years) and differed between ADHD subtypes (p = 1.8E-13) where predominantly hyperactive children were on average diagnosed earliest (at 5.7 years old) and predominantly inattentive children were diagnosed latest (at 6.5 years old). Overall, boys were consistently diagnosed earlier than girls across all ADHD subtypes. The majority of children were first diagnosed with ADHD by a paediatrician (66.7%), followed by psychologists (13.5%) and psychiatrists (6.3%), and this did not differ (p > 0.05) by gender or ADHD subtype presentation.
ADHD medication usage and side effects
Caregivers were presented with a list of the five most commonly used ADHD medications in Australia along with their common brand names: Dexamphetamine (dexamphetamine sulphate); short-acting Ritalin/Ritalin 10 (methylphenidate); long-acting Ritalin, Ritalin-LA and Concerta; Strattera (atomoxetine) and Modavigil (modafinil). They were asked to indicate which medications the index children had ever taken and were currently taking. A total of 1488 (94.6%) children were currently taking ADHD medication. Among those children, the mean number of medications taken was 1.2 (SD = 0.5, range = 1–3), with the most commonly prescribed medications being short-acting and long-acting Ritalin which were used by 29.8% and 56.9% of the children, respectively.
Approximately 17.3% of the children had taken only one of the five listed ADHD medications over their lifetime, with caregivers reporting almost 25% having taken three or more different medications (Table 2). The pattern of supplied prescriptions for ADHD medication in the linked PBS records from 2012 to 2015 (a 3-year 2-month window) was similar to that reported by caregivers; the mean number of medications ever supplied was 1.9 (SD = 0.7, range = 1–4), with 63.4% of children having been prescribed two ADHD medications and 11.0% having been prescribed three or more different medications.
ADHD medication use reported by gender.
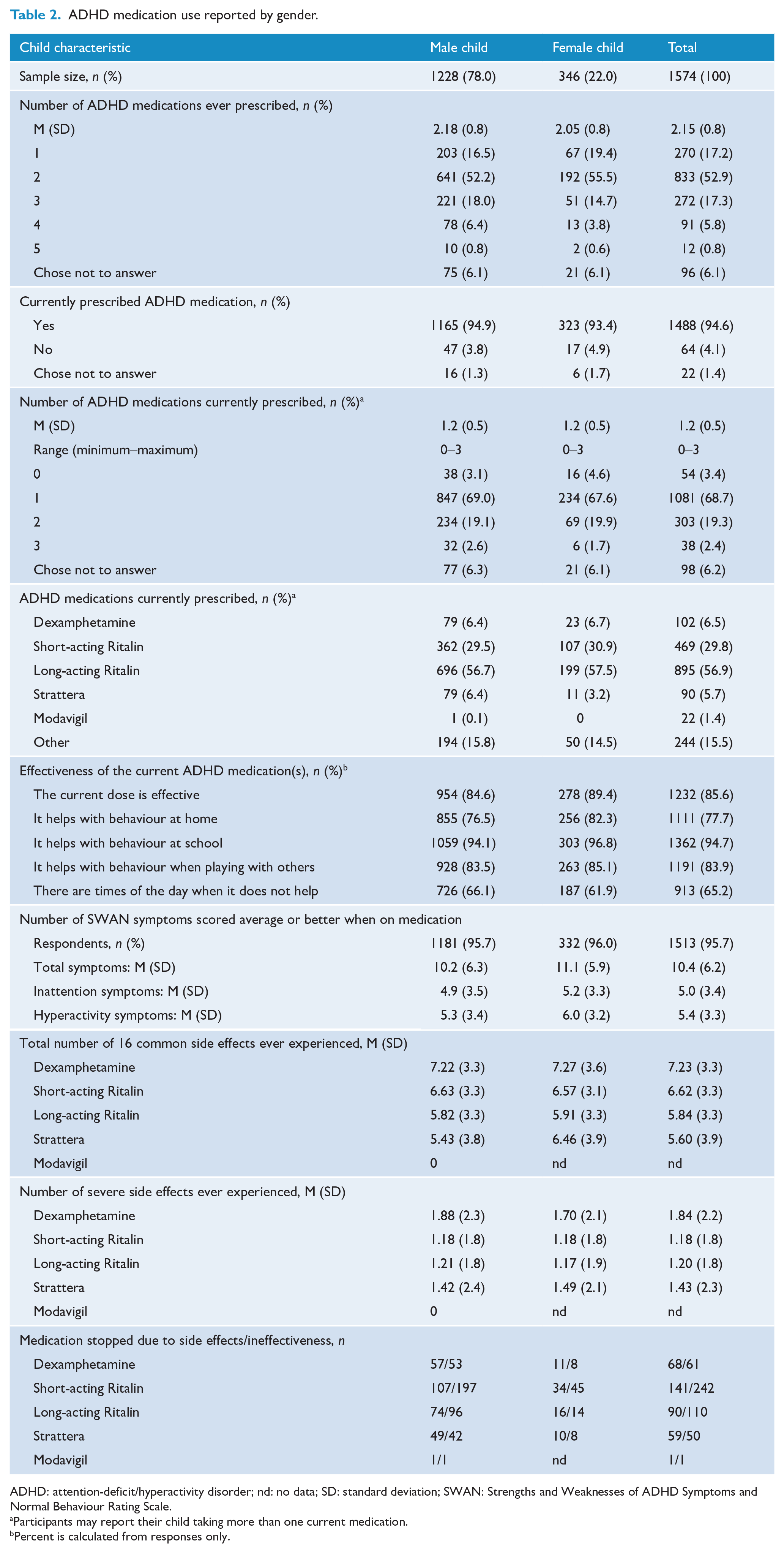
ADHD: attention-deficit/hyperactivity disorder; nd: no data; SD: standard deviation; SWAN: Strengths and Weaknesses of ADHD Symptoms and Normal Behaviour Rating Scale.
Participants may report their child taking more than one current medication.
Percent is calculated from responses only.
Overall, the majority of caregivers endorsed that the child’s current medication was effective in a number of scenarios, including at school and home. Finally, the severity (none, mild, moderate, severe) of the 16 most common side effects (headache, stomach ache, change of appetite, trouble sleeping, irritability, social withdrawal, extreme sadness/unusual crying, dull/tired/listless behaviour, tremors/feeling shaky, repetitive movements, picking at skin or fingers/nail biting/lip or cheek biting, seeing or hearing things that aren’t there, weight loss, blood pressure issues, dizziness) across the five medications listed is summarised in Table 2 and Figure 2. Table 2 also presents the number of caregivers who endorsed whether their child stopped taking ADHD medications due to side effects or ineffectiveness.
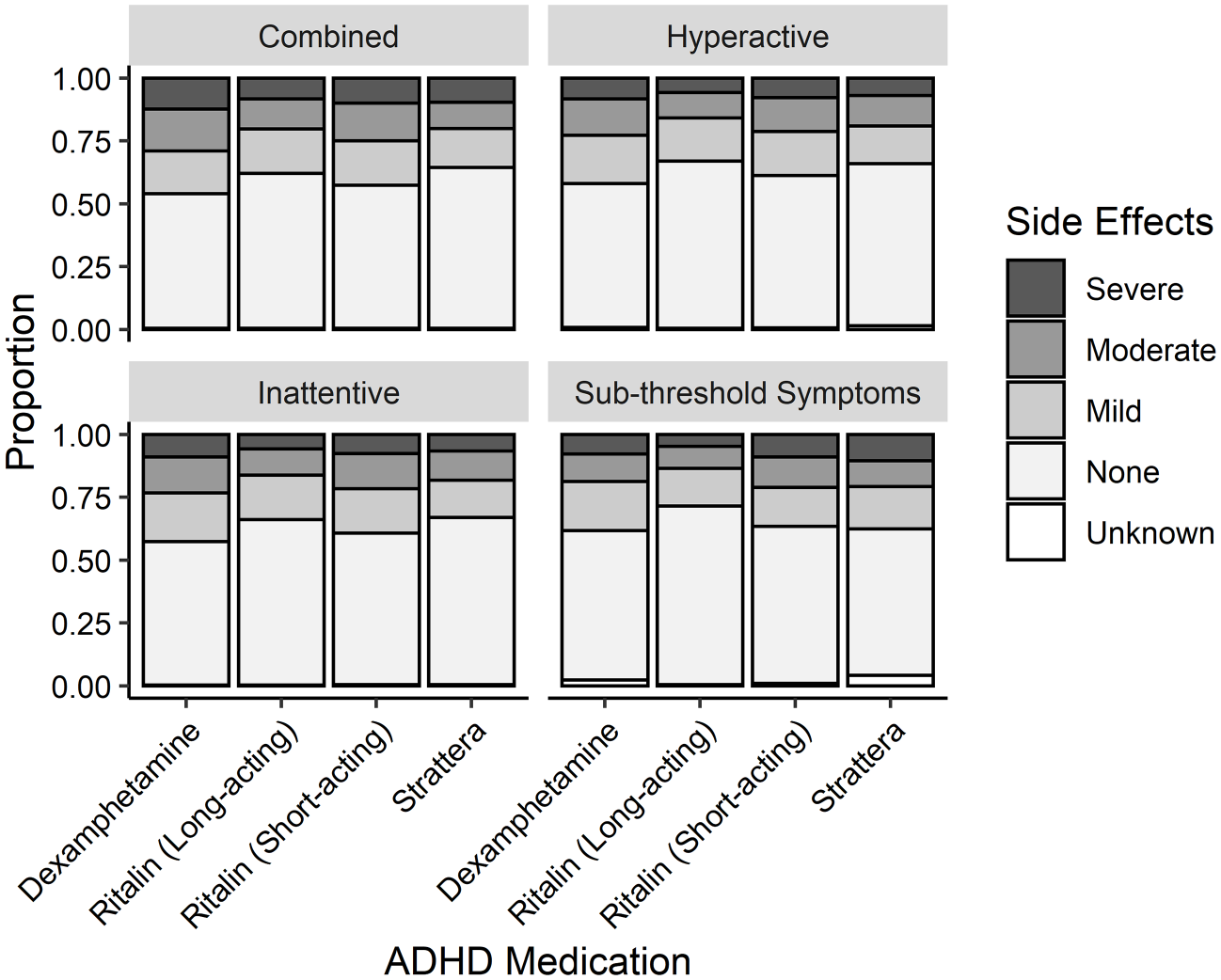
Severity of 16 side effects most commonly experienced for four different types of ADHD medications reported by ADHD subtype presentation.
PBS prescription records for the calendar year before and after ADHD diagnosis were explored to examine the impact of ADHD diagnosis on medication usage and health care costs. There were significant increases in both the average number of prescriptions supplied to the child (7.4 before vs 13.0 after), t(195) = −11.12, p = 1.5E-22, and different prescribing doctors seen (2.0 vs 2.3), t(195) = −2.822, p = 0.0052, in the calendar year following diagnosis. This resulted in a significant average increase of $78.44 in patient contributions (co-payments) made by each child’s family, $94.39 vs $172.83, t(195) = –6.481, p = 7.32E-10, and an average increase of $233.48 in cost to the PBS through prescription subsidies, $170.67 vs $404.17, t(195) = −7.650, p = 9.0E-13, in the calendar year following ADHD diagnosis.
Psychiatric comorbidity
Index children were screened for four psychiatric disorders (ODD, CD, ASD and anxiety and depression) commonly observed in children with ADHD. The majority of children (91.4%) screened positive for one or more of these disorders – almost one in three children (31.3%) screened positive for one disorder, 36.4% for two disorders and 22.6% for three or more disorders. Of note, gender had no impact on the frequency of these psychiatric comorbidities (p > 0.05). However, the number of psychiatric comorbidities experienced by children differed by ADHD subtype (p = 5.3E-39). Briefly, children presenting with the combined subtype screened positive on average for 1.9 disorders compared with 1.7 disorders in predominantly hyperactive children, 1.3 disorders in predominantly inattentive children and 1.0 disorder in children with sub-threshold ADHD symptoms.
Compared to children with sub-threshold ADHD symptoms, children presenting as the combined subtype were at highest risk of ODD (odds ratio [OR] = 20.2, 95% confidence interval [CI] = 12.0–34.0, p = 1.8E-29), CD (OR = 35.9, 95% CI = [5.0, 258.8], p = 3.8E-04) and symptoms of anxiety and depression (OR = 4.6, 95% CI = [2.8, 7.6], p = 1.4E-09), while at lowest risk of ASD (OR = 0.30, 95% CI = [0.20, 0.46], p = 3.0E-08). A consistent pattern of risk, but with smaller sizes of effect, was also found with children presenting as predominantly hyperactive and inattentive subtype. Similarly, the severity of obsessive-compulsive disorder (OCD) symptoms, as indexed by the Short OCD Screener (SOCS; Uher et al., 2007) score, did not differ by gender but was higher (p = 2.3E-13) among children presenting as a combined subtype (score = 3.0 ± 2.9) compared with predominantly inattentive and predominantly hyperactive (both 1.9 ± 1.9) children.
Education and learning difficulties
Primary caregivers provided data on learning support provided by schools and the prevalence of adverse school-related events such as suspension and expulsion (see Supplemental Table S4). Almost 1 in 10 (9.2%) children had repeated a school year. More than half of the children (51.4%) had been provided with a personalised intervention plan at school and 27.4% had been enrolled in special education at least part-time. While approximately one in five children had experienced a suspension, only 6% had been expelled from school (however, 19% of children who had a history of being suspended had also experienced an expulsion). Overall, 31% of caregivers responded that they were unsatisfied with the level of support the index child received at school. Being male increased the child’s odds of being provided with a personalised intervention plan (OR = 1.7, 95% CI = [1.3, 2.2], p = 1.9E-04) and experiencing suspension (OR = 2.7, 95% CI = [1.9, 3.9], p = 1.6E-07) or expulsion (OR = 1.9, 95% CI = [1.02, 3.5], p = 0.043). In addition, compared with children presenting as predominantly inattentive or with sub-threshold symptoms, children with combined or predominantly hyperactive subtypes were at a 2-fold or higher risk of experiencing suspension or expulsion. The likelihood of a child living with ADHD being suspended or expelled from school was significantly higher if they also screened positive for CD and ODD. With respect to school suspension, the OR for CD (ORCD) was 2.4 (95% CI = [1.8, 3.3], p = 4.0E-09) while ORODD = 2.3 (95% CI = [1.6, 3.3], p = 6.0E-06). For school expulsion, the ORCD = 2.8 (95% CI = [1.9, 4.5], p = 1.5E-0) and ORODD = 2.6 (95% CI = [1.21, 5.38], p = 0.013). After adjusting for ODD and CD, boys maintained a similar magnitude of risk for school suspension and expulsion compared with girls.
Discussion
The censusADHD study was established to recruit a nationwide cohort of Australian children aged 6–11 years living with ADHD. As expected from previous reports (Chow et al., 2014), almost two-thirds of the index children were first diagnosed with ADHD by paediatricians. Consistent with other population-based studies (Bianchini et al., 2013; Rowland et al., 2015), the proportion of index children of each ADHD subtype was as expected, indicating that the sample is representative of the DSM-IV diagnostic criteria for ADHD cases in the population. In our study, the combined subtype of ADHD was the most common subtype in both boys and girls, with significant differences in subtype presentation by gender observed. We also found the age of first ADHD diagnosis was significantly younger in boys, and boys were consistently diagnosed earlier across all ADHD subtypes. Similar to the finding of Applegate et al. (1997) that children with the predominantly inattentive subtype exhibit a later onset, we observed that the average age of diagnosis for children with this subtype presentation (6.5 ± 1.5 years) was older than for the combined (5.8 ± 1.6 years) and predominantly hyperactive (5.7 ± 1.5 years) subtypes.
Overall, approximately two-thirds of the children had taken two or more of the five most prescribed medications in Australia to treat their ADHD. Efficacy and side effects were variable. While most caregivers reported that the index child’s current medication was effective, medication side effects were common and resulted in medication cessation in some children.
Preliminary analysis of the data collected also offers information about the epidemiology of ADHD in an Australian context. A strong family history of childhood ADHD or attention problems was observed among the parents of the index children. This is consistent with the previously reported high heritability of ADHD in twin studies, where genetic effects explain ~75% of the variance (Faraone et al., 2005), and similar to the estimated 41–55% observed in smaller studies (Smalley et al., 2000; Starck et al., 2016; Takeda et al., 2010). Similar to Takeda et al. (2010), children who had one or more parents with a history of ADHD exhibited more severe ADHD symptoms. Consistent with previous studies (Erskine et al., 2016; Gillberg et al., 2004; Quinn, 2008), high levels of comorbid ODD (~70%) and CD (~20%) were also observed among the children.
Children living with ADHD have been found to be 3–6 times more likely to experience adverse academic and educational outcomes, including repeating grades, qualifying for special education services or being suspended or expelled from school compared to children without ADHD (LeFever et al., 2002). In our study, caregivers reported that their children experienced many learning and behavioural difficulties at school. Approximately 1 in 5 children had a history of suspension and almost 6% had been expelled previously; boys, children with hyperactivity symptoms (combined and predominantly hyperactive subtypes) and children who screened positive for the externalising disorders CD and ODD were at greater risk of both adverse schooling outcomes. While the rate of grade repetition (9.2%) was higher than the 4% reported in an Australian study of 136 high school–aged children with ADHD (Martin, 2014), international studies report that 9–40% of children with ADHD have repeated a year at school (Flood et al., 2016). Our finding that 49.1% and 25.4% of children had accessed school-based learning support and special education, respectively, is higher than the rates of 17% and 5% observed among 398 Australian children and adolescents with ADHD in 1998 (Sawyer et al., 2004). However, Zendarski et al. (2020) reported that 60% of 130 Australian adolescents with ADHD had accessed school-based education support, including Individualised Educational Plans (22%), in 2014.
While this study did not focus on the healthcare utilisation data in the linked MBS records, we have shown ADHD diagnosis is associated with significant increases in healthcare costs both to the index child’s family and to the PBS. Given that the Deloitte Access Economics (2019) report estimated non-healthcare costs to be $24,071 per person with ADHD, we also expect to observe an increase in indirect (for example, time spent out of role) costs to families following their child’s ADHD diagnosis.
The major strength of the study is its sample size, as it is one of the largest population-based studies of children living with ADHD in Australia. Importantly, 81% of caregivers consented to link the online survey data with the index child’s electronic PBS and MBS records – these pharmaceutical and health utilisation records have now been obtained for over 65% of the children. Validation of self-report data can be achieved using PBS prescription records and these records will also allow measures to be derived, such as medication cessation or switching due to adverse side effects. Prescribing cascades would also be identifiable.
Moreover, the study also demonstrates that in countries with strictly regulated prescribing of ADHD medications, prescription-based recruitment is a feasible and cost-effective method of recruiting a relatively large cohort of children with ADHD. Ethnicity data for the 1574 children indicate that our study is representative of the Australian population and that we were able to recruit children from diverse populations.
Despite these strengths, this study has some limitations. First, our medication-based recruitment strategy meant that only caregivers of children with three or more dispensed ADHD prescriptions were within our sampling frame. Given that many children with ADHD in Australia are undiagnosed (Efron et al., 2014) or not prescribed medication (Charles et al., 2011; Efron et al., 2014; Lawrence et al., 2015; Stephenson et al., 2013), it is unclear whether our strategy has caused bias towards the recruitment of children with more severe forms of ADHD and whether our findings will generalise to the majority of Australian families of children living with ADHD. Second, selection bias cannot be excluded since there was a relatively low participation rate (6.2%) from the 25,920 caregivers sent study invitation letters by Services Australia and we do not know whether there are systematic differences between caregivers who chose to participate and those who did not. However, ADHD subtype presentation in the index children was similar to that observed in other population-based samples. Finally, we do not have data from a large cohort of children who had not been diagnosed with ADHD, so we cannot compare our PBS findings with children in the general population.
Conclusion
Our medication-based recruitment strategy successfully resulted in the recruitment of a cohort of 1574 caregivers of children living with ADHD. While gender did not differentially affect psychiatric comorbidity among the children, gender influenced age of ADHD diagnosis across all subtype presentations. Overall, the majority of children screened positive for at least one other psychiatric disorder, with children presenting with the combined subtype most at risk for psychiatric comorbidities. Future analyses of the PBS and MBS data will allow us to clarify the relationship between ADHD symptom severity and subtype presentation, pharmacotherapy treatment response, cost of illness and health service usage within an Australian context, but which is likely to be generalisable to other Western countries.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221089234 – Supplemental material for censusADHD Study: An Australian-wide medication-based recruitment study for Attention-Deficit/Hyperactivity Disorder
Supplemental material, sj-docx-1-anp-10.1177_00048674221089234 for censusADHD Study: An Australian-wide medication-based recruitment study for Attention-Deficit/Hyperactivity Disorder by Penelope A Lind and Sarah E Medland in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We thank the participants for giving their time and support for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Data collection was funded by a Seed Grant from the QIMR Berghofer Medical Research Institute to S.E.M. Data analysis was supported by the National Health and Medical Research Council (Grant No. APP1158125). S.E.M. is supported by a National Health and Medical Research Council Investigator Grant (No. APP1172917).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.