
Abstract
Objective:
This review, which was registered with PROSPERO (CRD42021237988), aimed to systematically extract common elements in the hikikomori definition or criteria applied by researchers and examine cultural differences and chronological changes in the demographic characteristics of hikikomori individuals such as age, gender and hikikomori duration.
Method:
For inclusion in the review, the hikikomori criteria, age and gender of the hikikomori individuals had to be specified, and the article had to be peer-reviewed and written in Japanese or English, focusing on hikikomori individuals or their families. Case studies, reviews and qualitative studies were excluded.
Results:
The total sample size for the 52 studies included in the review was 4744. Over 80% of the studies included the elements ‘not working or attending school’, ‘not socializing outside one’s home’ and ‘duration of hikikomori’ in their hikikomori criteria, and many studies included the element ‘staying at home on most days except solitary outings’. A cross-temporal meta-analysis showed the possibility that the age of hikikomori individuals increased chronologically (β = 0.44, B = 0.50, 95% confidence interval = [0.16, 0.84]). Comparisons weighted by sample size between Japan and other countries showed the possibility that the age of hikikomori individuals was higher (d = 0.32), the percentage of males was lower (d = 0.91) and the hikikomori duration was shorter (d = 2.06) in studies conducted in countries other than Japan. However, many of the included studies had a high risk of selection bias, and this bias may have influenced the results obtained. Thus, the results of this study may represent the researcher’s perception of hikikomori rather than accurately representing the actual condition of hikikomori.
Conclusion:
Researchers should specifically identify similarities and differences in the clinical picture of hikikomori and compare the studies to organize the findings derived from studies focusing on hikikomori.
Introduction
Hikikomori has attracted social attention in Japan since the 1990s and has recently been reported in many regions (Bowker et al., 2019; Teo et al., 2015). This phenomenon has serious consequences for the individual, including poor functioning (Kondo et al., 2013) and poor quality of life (Nonaka and Sakai, 2014), and has significant social consequences, as the individual is not independent and often requires support for their living, including financial assistance from family members and the local and central government. It is necessary to enhance the understanding of hikikomori to establish a fundamental support system.
Recently, there has been an increase in psychiatric, psychological and sociological research on hikikomori, but these studies have not been consistently based on the same demographic and clinical features, including hikikomori definition, age, gender and hikikomori duration. Some studies have used the definition provided in the Japanese Ministry of Health, Labour and Welfare’s guidelines for hikikomori (Japanese Ministry of Health, Labour and Welfare, 2010), while others have used the definition by Teo and Gaw (2010), Teo et al. (2015) or other definitions (Yuen et al., 2018), and recently, a new definition has been proposed (Kato et al., 2019, 2020). These definitions include elements that are common and elements that are not, and it is unclear how these differences influence the characteristics of hikikomori individuals. Given that hikikomori represents a variety of features that are influenced by comorbid psychiatric disorders (Kondo et al., 2013), culture (Bowker et al., 2019) and socioeconomic status (Nonaka and Sakai, 2021), a lack of clarity about how demographic and clinical features differ between studies has significant implications for comparing and integrating findings across studies. Thus, it is helpful to integrate previous studies and systematically clarify the features of hikikomori that have been identified by researchers.
Teo and Gaw (2010) and Li and Wong (2015) reviewed the literature and qualitatively examined several definitions of hikikomori but did not quantitatively examine or culturally compare them. Additionally, Teo and Gaw (2010) did not examine the division of hikikomori into elements, and Li and Wong (2015) did not include the Japanese literature, which accounts for the majority of the literature on hikikomori. This study quantitatively examined the ratio of studies that included each element when selecting hikikomori individuals. The operational definition of hikikomori used in previous studies can be categorized into the following elements: (a) not working or attending school, (b) not socializing outside one’s home, (c) staying at home on most days except solitary outings, (d) social isolation in one’s home, (e) significant functional impairment or distress associated with social isolation and (f) hikikomori duration (Japanese Ministry of Health, Labour and Welfare, 2010; Kato et al., 2019, 2020; Teo et al., 2015).
Although some previous reviews have systematically reviewed studies on hikikomori (Li and Wong, 2015; Nonaka et al., 2019; Pozza et al., 2019; Yung et al., 2021), none of these studies except Nonaka et al. (2019), which targeted family support, covered the Japanese literature. Using APA PsycInfo and MEDLINE, 265 articles (including duplicates) were identified that included ‘hikikomori’ in the title or abstract, and while using the Japanese database CiNii, 2334 articles were identified that included ‘ひきこもり’ OR ‘引きこもり’ (meaning ‘hikikomori’ in Japanese with or without Kanji) in the title (as of 6 September 2021). Although the English literature has expanded recently, the Japanese literature is still more than eight times larger than the English literature, and thus, a review including this literature would capture more findings (Figure 1).
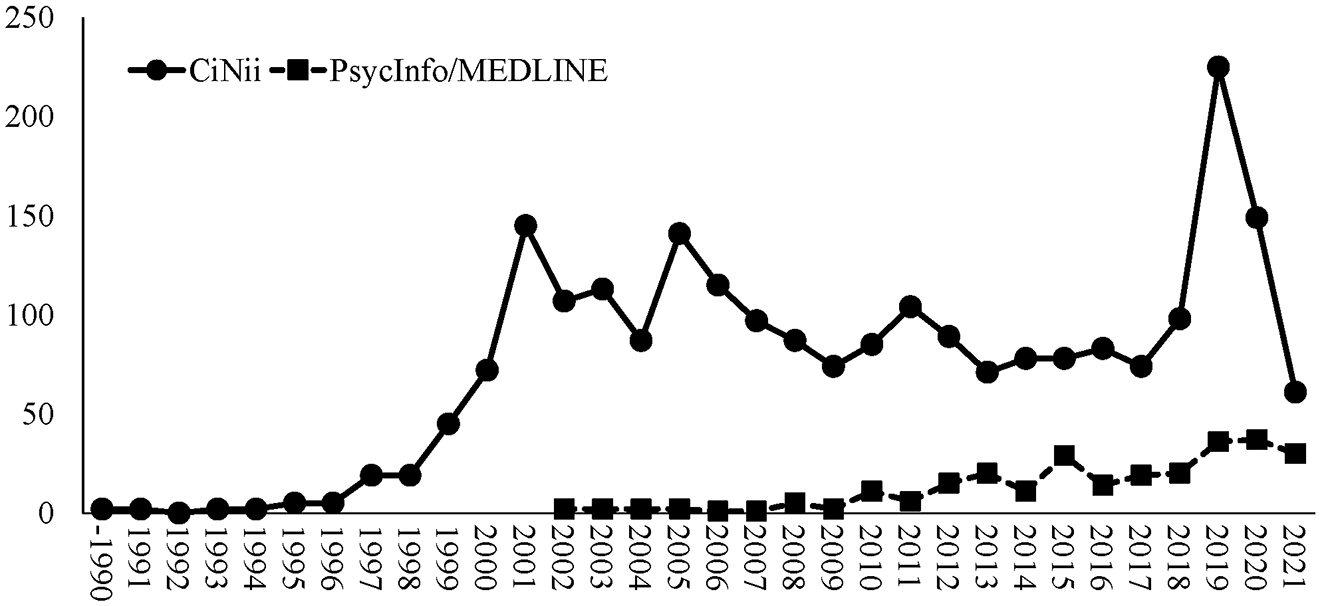
Trend in the number of studies related to hikikomori by electronic database.
This study reviewed the operational definitions of hikikomori used in previous studies on hikikomori written in Japanese or English. Furthermore, we examined the demographic characteristics of hikikomori individuals, including age, gender, hikikomori duration, cultural differences and chronological changes in these characteristics. One of the chronological changes is the problem of the aging of hikikomori. A generation of people in Japan called the ‘employment ice age’ looked for jobs in the 1990s and 2000s when the job market was severe, and the government started a program in 2019 to support this generation for work and life. The average age of hikikomori may be higher if hikikomori occurred more frequently in this generation. Thus, the trend toward higher age of hikikomori was also examined in this study.
Methods
Search strategy and inclusion and exclusion criteria
The systematic review was registered with PROSPERO (CRD42021237988) and is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement (Page et al., 2021). We searched the electronic databases MEDLINE, PsycINFO and the Japanese electronic database CiNii. The following terms were used: ‘hikikomori’ in MEDLINE, PsycINFO title or abstract search, ‘ひきこもり’ OR ‘引きこもり’ (meaning ‘hikikomori’ in Japanese with or without Kanji) in CiNii title search. This review was restricted to peer-reviewed, cross-sectional, case-control, cohort designs and intervention studies and excluded reviews, case series and qualitative studies. For inclusion in the review, the authors of a given study had to regard the study participants, or their families, as being in a hikikomori state or a state analogous to hikikomori. Moreover, the following information had to be specified: (1) operational definition of ‘hikikomori’ or inclusion criteria for ‘hikikomori’ and (2) age and gender ratio of hikikomori individuals. The literature was screened by two independent reviewers. The literature was first screened based on title, abstract and journal title and then those not excluded were screened based on full text. Studies that included only cases who had experienced hikikomori but were recovering from hikikomori at the time of the study were excluded. If a study included both people in a hikikomori state and otherwise (e.g. people in recovery), studies that exclusively presented data for people in a hikikomori state were included in the review, and data exclusively for people in hikikomori were included in the analysis.
Data extraction
Two reviewers (S.N. and T.T.) judged the study eligibility and extracted data by reviewing the full text of the eligible articles independently. Any disagreement was resolved through a third party (M.S.) in a systematic review. The extracted data included publication date, date when the research was conducted, the country where the study was conducted, inclusion and exclusion criteria used to define hikikomori, operational definition of hikikomori, the sample size in hikikomori cases, mean or range of age, percentage of males and females, research design and the type of scale used to assess hikikomori.
Outcome measures
This review examined the ratio of hikikomori targeted in each study that met the elements classified according to the definitions employed in previous studies (Japanese Ministry of Health, Labour and Welfare, 2010; Kato et al., 2020; Teo et al., 2015). Specifically, the definition or criteria specified in each study were coded as to whether they included the following elements: (a) not working or attending school, (b) not socializing outside one’s home, (c) staying at home on most days except solitary outings, (d) social isolation in one’s home, (e) significant functional impairment or distress associated with social isolation, (f) duration of hikikomori and (g) age criteria. Social participation was regarded as meeting with others, working or attending school, and socializing outside one’s home, according to the Japanese Ministry of Health, Labour and Welfare (2010). Avoidance of attending school, working and social participation was categorized as ‘not working or attending school’. Additionally, we examined the relationship between the mean age of hikikomori individuals, gender ratio, hikikomori duration, and the year and country in which the study was conducted.
Analysis
Statistical analyses were conducted using SPSS (IBM SPSS version 27) and Jamovi version 1.6 (The Jamovi Project, 2021). Chi-square tests were used to examine associations between the elements of the hikikomori definition or criteria and the study region or age of the participants. The study region was coded as Japan or countries outside Japan. Studies that included both Japan and countries outside Japan were coded as countries outside Japan. The participants’ ages were coded as high or low based on the weighted means by sample size. The type of scale used to assess hikikomori was coded 1 for studies that included proxies, such as parent-report questionnaires or proxy-reported interviews, and 0 for studies that did not include proxies (only hikikomori individuals). Sensitivity analyses were not performed.
A cross-temporal meta-analysis (Twenge, 2000) based on regression analysis, weighted by sample size, was used to examine chronological changes in the age, gender proportions and hikikomori duration of hikikomori individuals. The median age was included in the analysis instead of the mean for the studies in which only the median age was provided. For studies in which frequencies were described by age class but not mean values, approximate means were calculated using class values and frequencies and included in the analysis. Unknown samples in the frequency by age class were excluded, and an approximate mean was calculated (Watabe et al., 2010). In a study by Tsujimoto and Tsuji (2008), where the maximum value was described by an uncertain age class, the class of 40 years old and above was regarded as the class of 40–44 years old. Chronological changes were based on the year in which the study was performed. For studies in which the year of the study was provided, the median difference between the year the study was performed and the publication year was 3 years; thus, for studies in which the year of the study was not provided, 3 years before the year of publication was included as the year of implementation.
Risk of bias assessment
Selection bias was evaluated at the study level using the Joanna Briggs Institute (JBI) critical appraisal checklist (Moola et al., 2020). Two raters independently evaluated the risk of bias for each study.
Results
Study selection
After searching the databases, 2490 studies were identified (Figure 2). After screening, 52 studies were included in the analysis. Agreement between ratings by two independent reviewers showed κ = 0.57 (95% confidence interval [CI] = [0.50, 0.64]) for title, abstract and journal title screening and κ = 0.78 (95% CI = [0.69, 0.88]) for full-text screening.
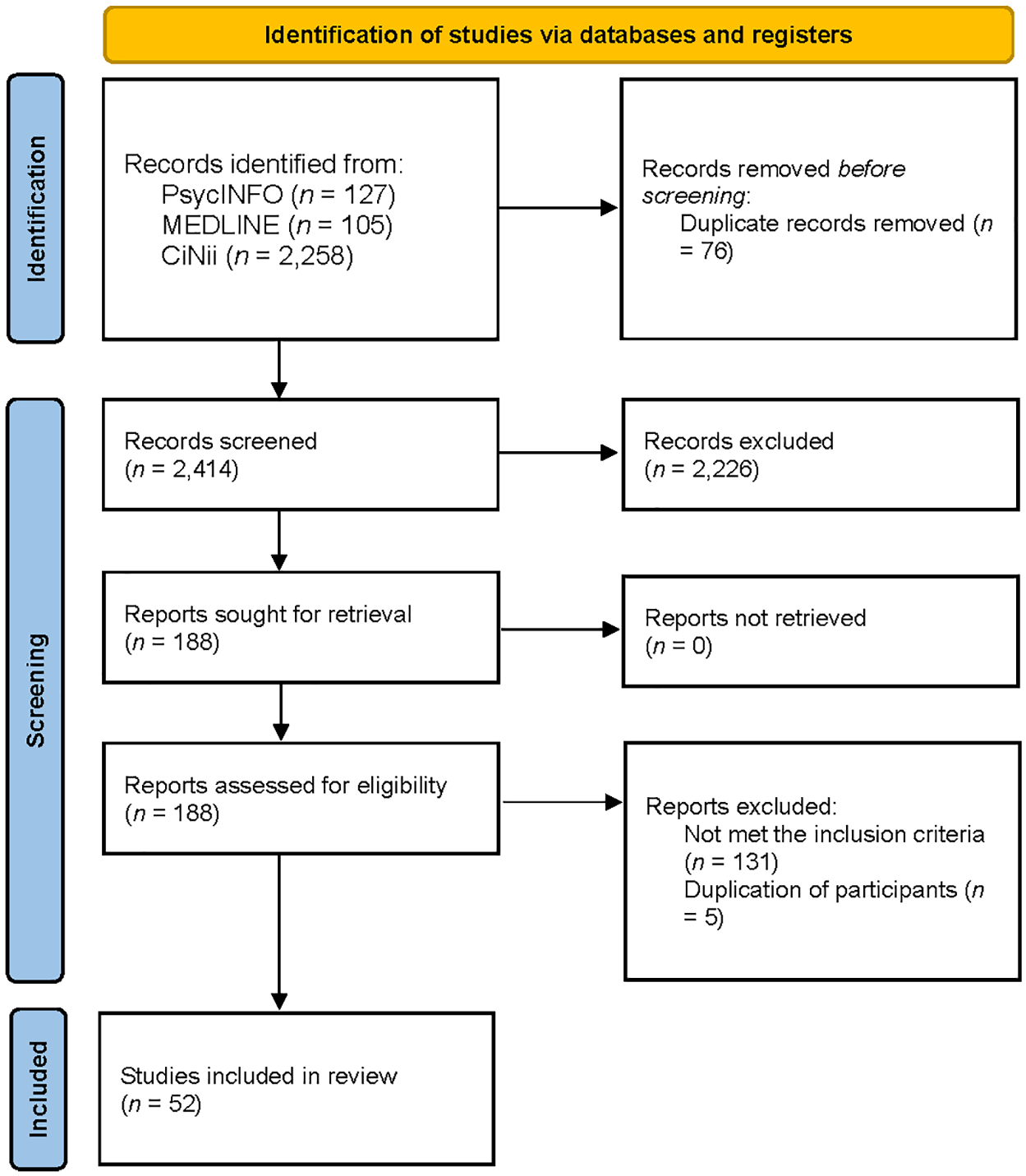
Flow diagram of the search process for this review.
Study characteristics
Of the studies included in the review, 84.6% were performed in Japan, 13.5% were performed outside Japan and 1.9% were performed in both Japan and outside Japan (Table 1). Of these studies, 46.2% were case–control studies, and 40.4% were cross-sectional studies. The total sample size of the 52 studies included in this review was 4744. Limited studies used gold standard diagnostic tools for the diagnosis of comorbid psychiatric disorders (Katsuki et al., 2019; Lee et al., 2013; Nagata et al., 2013; Teo et al., 2020; Yokose et al., 2014; Yuen et al., 2018).
Summary of the studies included in the review.
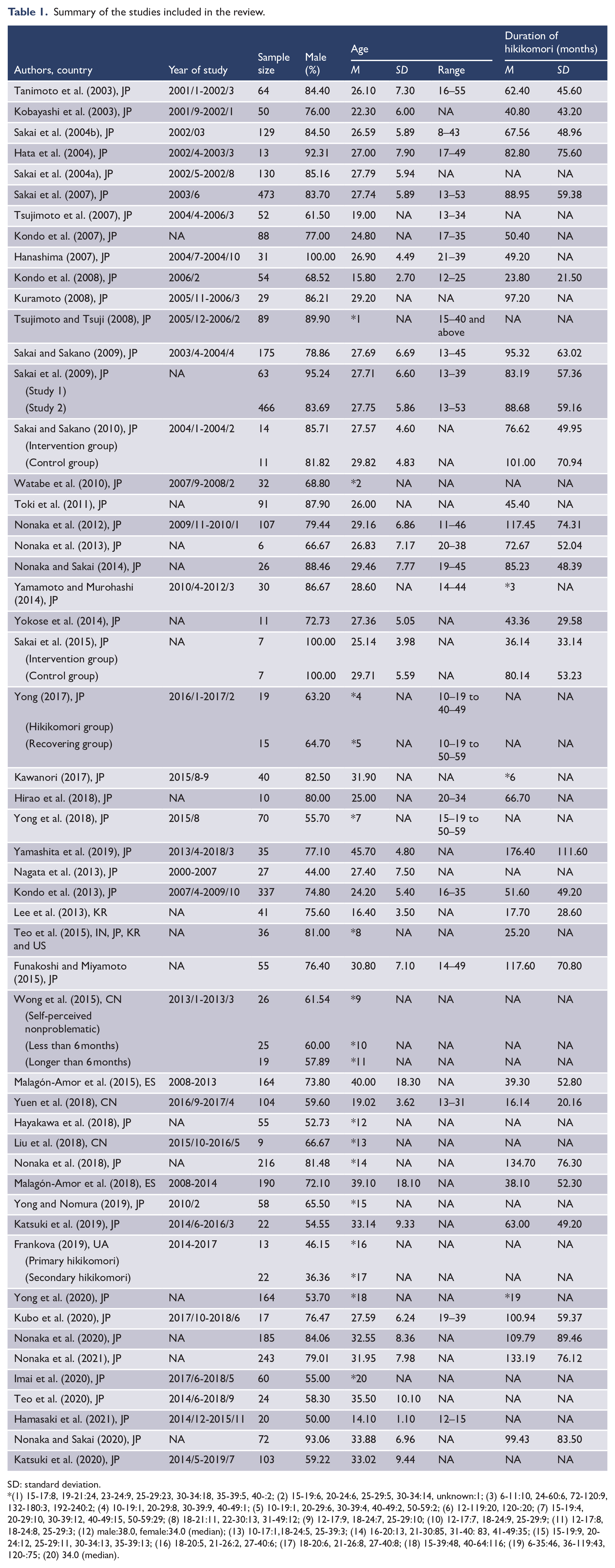
SD: standard deviation.
(1) 15-17:8, 19-21:24, 23-24:9, 25-29:23, 30-34:18, 35-39:5, 40-:2; (2) 15-19:6, 20-24:6, 25-29:5, 30-34:14, unknown:1; (3) 6-11:10, 24-60:6, 72-120:9, 132-180:3, 192-240:2; (4) 10-19:1, 20-29:8, 30-39:9, 40-49:1; (5) 10-19:1, 20-29:6, 30-39:4, 40-49:2, 50-59:2; (6) 12-119:20, 120-:20; (7) 15-19:4, 20-29:10, 30-39:12, 40-49:15, 50-59:29; (8) 18-21:11, 22-30:13, 31-49:12; (9) 12-17:9, 18-24:7, 25-29:10; (10) 12-17:7, 18-24:9, 25-29:9; (11) 12-17:8, 18-24:8, 25-29:3; (12) male:38.0, female:34.0 (median); (13) 10-17:1,18-24:5, 25-39:3; (14) 16-20:13, 21-30:85, 31-40: 83, 41-49:35; (15) 15-19:9, 20-24:12, 25-29:11, 30-34:13, 35-39:13; (16) 18-20:5, 21-26:2, 27-40:6; (17) 18-20:6, 21-26:8, 27-40:8; (18) 15-39:48, 40-64:116; (19) 6-35:46, 36-119:43, 120-:75; (20) 34.0 (median).
Definition or criteria for hikikomori
Of these, 96.2% met at least one element, 94.2% met two or more elements, 84.6% met three or more elements, 61.5% met four or more elements and 19.2% met five or more elements. Only two studies did not meet any of the elements (Funakoshi and Miyamoto, 2015; Sakai et al., 2004b). Funakoshi and Miyamoto (2015) noted that they had to use a definition that did not match that of the Japanese Ministry of Health, Labour and Welfare (2010) as an important limitation. They recognized the definition by the Japanese Ministry of Health, Labour and Welfare (2010) as hikikomori. Sakai et al. (2004b), whose study was performed before most of the definitions were proposed, operationally defined ‘People who perceive themselves or their families to be hikikomori’, based on the subjective ratings of the participants.
More than 80% of the studies included elements A (not working or attending school), B (not socializing outside one’s home) or F (duration of hikikomori), and many studies included element C (staying at home on most days except solitary outings) (Table 2; Supplemental material). In contrast, only a few studies included elements D (social isolation in one’s home), E (significant functional impairment or distress associated with social isolation) and G (age criteria). Of the studies that included hikikomori duration as a criterion, 85.7% used 6 months as the criterion.
Elements of the hikikomori definition/criteria for the studies included in the review.
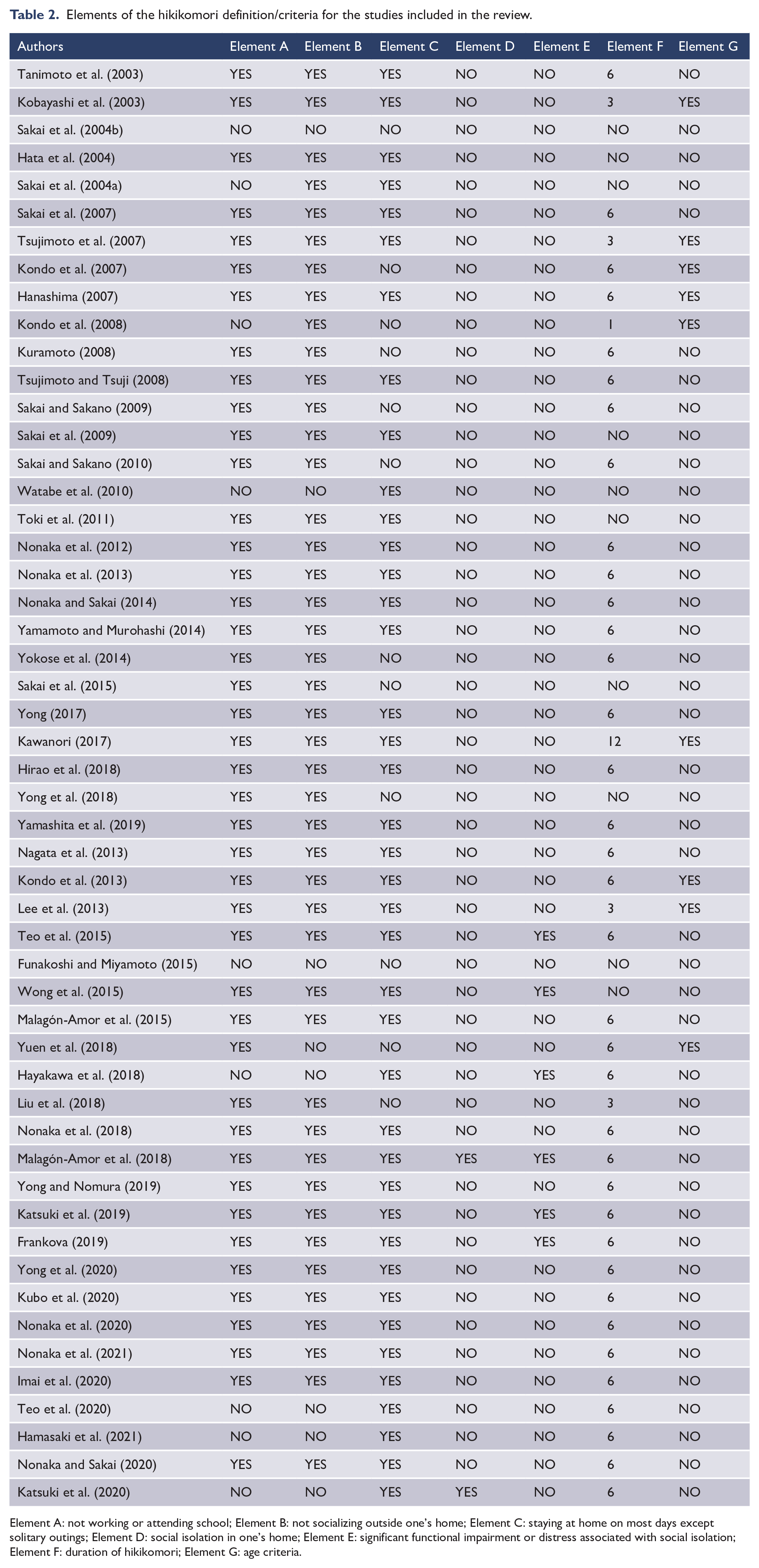
Element A: not working or attending school; Element B: not socializing outside one’s home; Element C: staying at home on most days except solitary outings; Element D: social isolation in one’s home; Element E: significant functional impairment or distress associated with social isolation; Element F: duration of hikikomori; Element G: age criteria.
A larger proportion of studies outside Japan included element E compared to studies in Japan (χ2 = 13.70, p = 0.003). There were no significant rate differences in the other elements (Table 3). Additionally, there was no significant rate difference between studies with older and younger hikikomori individuals for any of the elements.
Association between the study region and the elements of the hikikomori definition/criteria.
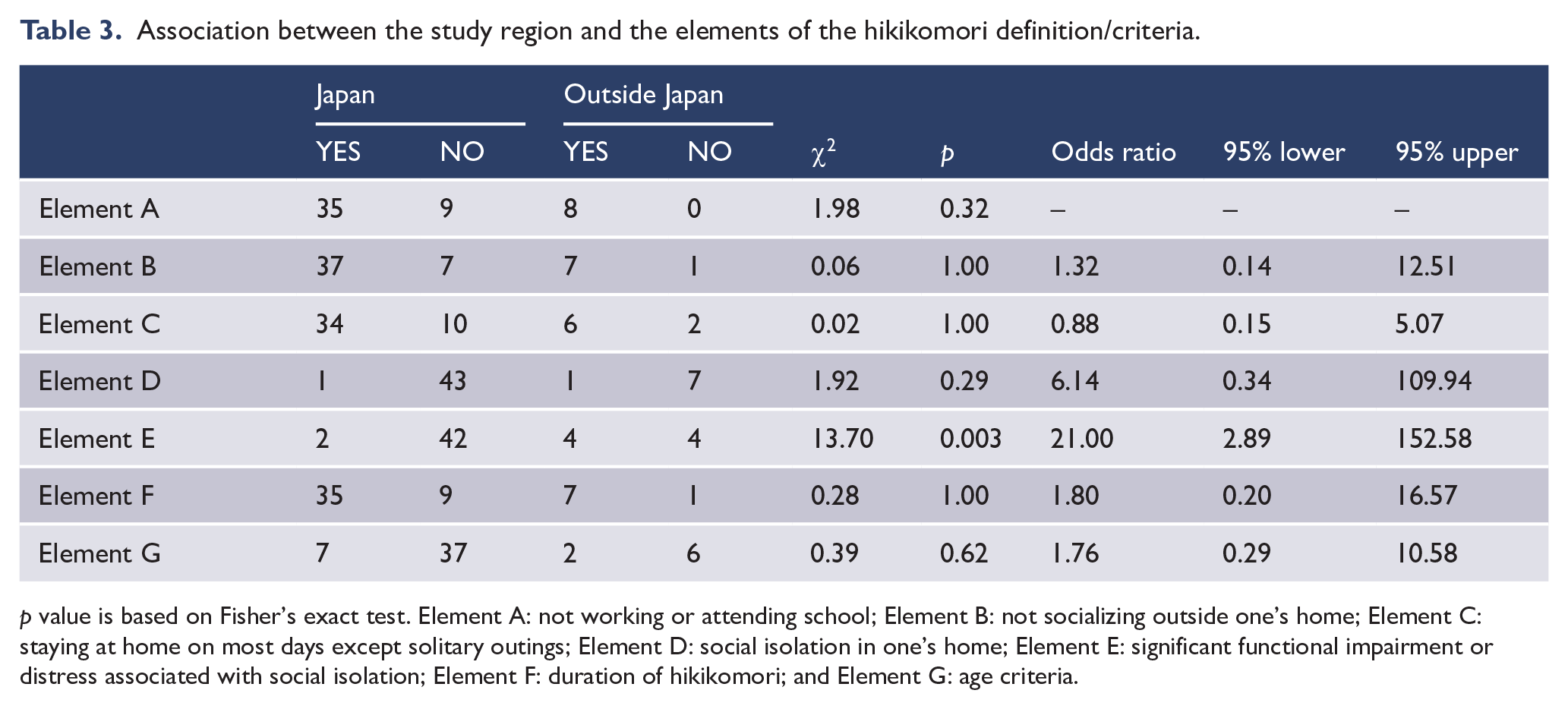
p value is based on Fisher’s exact test. Element A: not working or attending school; Element B: not socializing outside one’s home; Element C: staying at home on most days except solitary outings; Element D: social isolation in one’s home; Element E: significant functional impairment or distress associated with social isolation; Element F: duration of hikikomori; and Element G: age criteria.
Demographic features
The mean values weighted by sample size were 29.55 (95% CI = [29.37, 29.72]) for the age of hikikomori individuals, 76.49 (95% CI = [76.17, 76.81]) for the percentage of males and 80.66 (95% CI = [79.54, 81.78]) months for the hikikomori duration.
A cross-temporal meta-analysis for age weighted by sample size showed that the regression model was significant (Table 4; R2 = 0.24, R2 adj = 0.18, p = 0.01). The year of study showed a positive regression coefficient (β = 0.44, p = 0.005), whereas the percentage of males, country and assessment type did not show significant coefficients. Figure 3 is a scatter plot showing the relationship between the age of hikikomori individuals and the year of study.
Linear regression results of a cross-temporal meta-analysis.
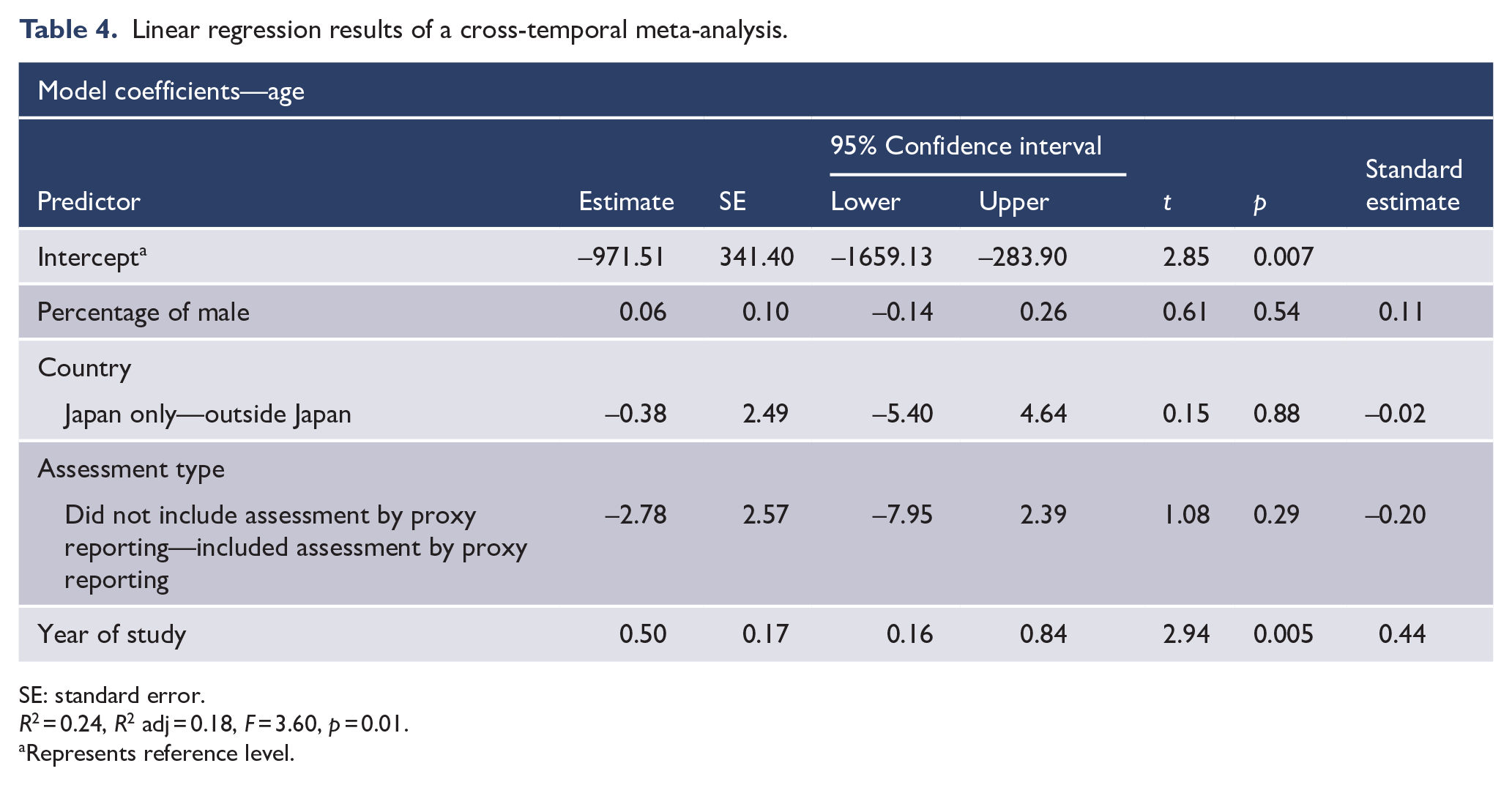
SE: standard error.
R2 = 0.24, R2 adj = 0.18, F = 3.60, p = 0.01.
Represents reference level.
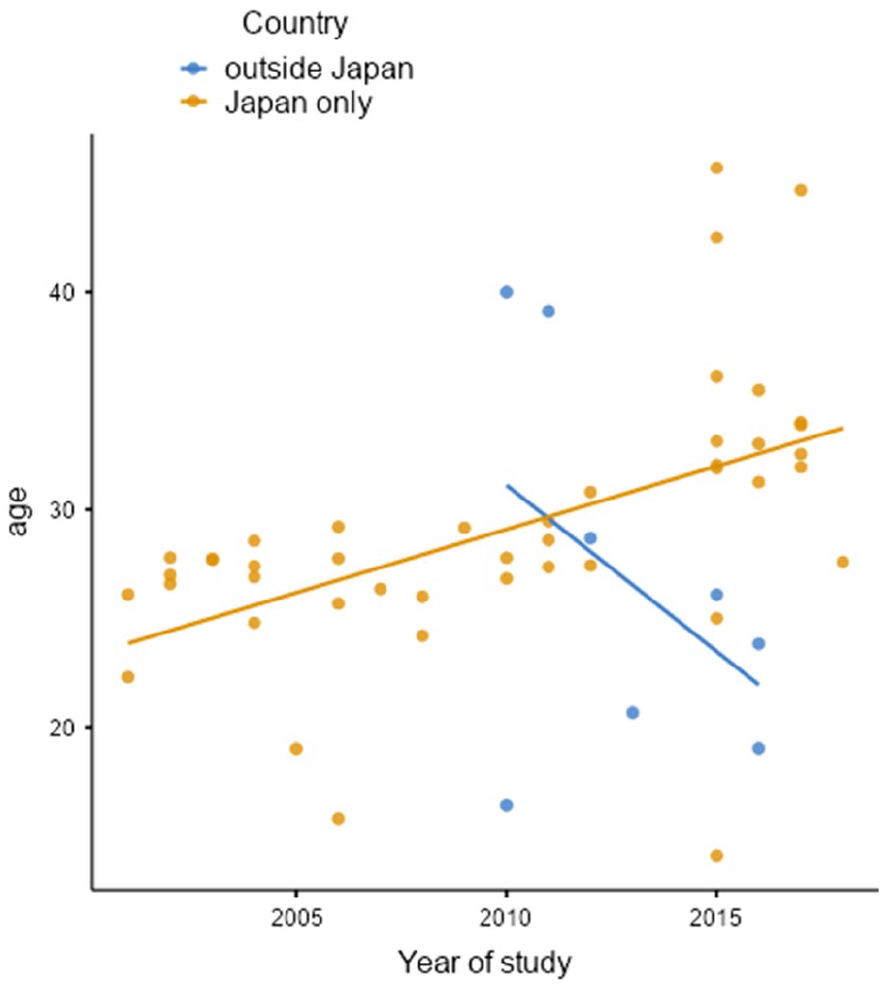
Scatter plot showing the relationship between age of hikikomori individuals and the year of study.
The results of group differences weighted by sample size showed that studies outside Japan had older participants (t (713.49) = 5.00, p < 0.001, d = 0.32), lower percentages of males (t (949.34) = 23.99, p < 0.001, d = 0.91), and a shorter hikikomori duration (t (2477.55) = 83.80, p < 0.001, d = 2.06), than studies in Japan.
Risk of bias assessment
For the two-item critical appraisal checklist for selection bias, two independent reviewers assessed that 73.1% overall, 69.2% and 76.9% of each item did not meet the element.
Discussion
The following elements of the definition of hikikomori seemed approximately consistent among researchers: ‘not working or attending school’, ‘not socializing outside one’s home’, ‘staying at home on most days except solitary outings’ and ‘Hikikomori duration over six months’. One reason for this result may be that the definitions (Japanese Ministry of Health, Labour and Welfare, 2010; Teo and Gaw, 2010) used (entirely or partially) by many studies originate from a common definition (Japanese Ministry of Health, Labour and Welfare, 2003), which includes these elements.
There was a difference between studies conducted only in Japan and those conducted in other countries in whether or not the element of functional impairment was included in the definition or criteria of hikikomori. This difference is because the definition of the Japanese Ministry of Health, Labour and Welfare (2010) does not include functional impairment, while the definitions of Teo and Gaw (2010) and Kato et al. (2020) include that criterion. Additionally, this difference is accounted for by the observation that the Japanese Ministry of Health, Labour and Welfare (2010) argues that hikikomori is a concept rather than a symptom of a disease or disorder and that not all hikikomori necessarily need some support or treatment (Japanese Ministry of Health, Labour and Welfare, 2010), while the definition provided by Kato et al. (2020) is primarily intended as a criterion for diagnosis. Certainly, hikikomori individuals do not engage in social participation, and in most cases, their social functioning is likely to be impaired; however, researchers should still clarify whether the hikikomori definition/criterion in their studies includes impairment in social functioning.
Social isolation was also not included as a hikikomori criterion in many studies, which could be because it was only recently proposed to use social isolation as a criterion (Kato et al., 2019). Kato et al. (2019) and Kato et al. (2020) suggested a criterion of marked and continuous ‘social isolation’, which is mainly defined by the frequency of going out (3 days a week or less) than a criterion of avoidance of social participation or social interaction, or staying mainly at home. However, further psychiatric, psychological and sociological evidence will be needed to examine how this change in the criteria influences the interpretation of the existing evidence and whether it adequately represents the actual conditions. Although social isolation studies have mainly been conducted in the elderly and do not necessarily have a consensus definition (Fakoya et al., 2020), clarifying the similarities and differences between the hikikomori and social isolation states may have a synergistic effect on the accumulation of findings. Additionally, fewer than 20% of the studies included the participants’ age in the definition/criteria of hikikomori, and many of them were limited to teenagers and young adults in their twenties with a focus on young people.
Many of the studies included an element of avoidance of social participation, whereas some of them included cases in which people were working (Frankova, 2019; Liu et al., 2018; Wong et al., 2015; Yong et al., 2020). This implies that in some cases, people ‘avoid’ social participation, but actually engage in it. Given these cases, researchers should also clearly report whether their studies include actual social participation in their definition of hikikomori.
The results of the cross-temporal meta-analysis showed that hikikomori individuals are getting older. Although this aging phenomenon has attracted social attention, there is little scientific evidence to support it. This systematic finding will help improve the understanding of hikikomori and provide significant evidence for the establishment of a support system. Future studies will be needed to clarify the background to the older age of hikikomori individuals, such as whether this phenomenon reflects a change in the triggers of hikikomori, a longer duration of hikikomori or a change in the social perception of hikikomori.
This study had several limitations. In this regard, some studies included some psychiatric disorders as exclusion criteria, and it is unclear how the comorbidity of psychiatric disorders influenced the findings obtained. Indeed, while the inclusion or exclusion of psychiatric disorders is inconsistent across studies (Li and Wong, 2015), it seems that psychiatric disorders are often not included in the exclusion criteria more recently (e.g. Kato et al., 2019). Clarification of the hikikomori type by comorbid psychiatric disorders is also vital for understanding the pathology and establishing treatment. Suwa and Suzuki (2013) classified hikikomori into primary hikikomori without comorbid psychiatric disorders and secondary hikikomori with comorbid psychiatric disorders for discussion of psychopathology, and many studies focused on the differences between them (Frankova, 2019; Martinotti et al., 2021; Suwa and Suzuki, 2013). Additionally, there is a suggestion that cases in which psychiatric disorders appear during prolonged hikikomori should be distinguished from secondary hikikomori as zeroth-order hikikomori (Sakai, 2012). In contrast, findings are insufficient to clarify psychopathological differences between these types, with one report showing that primary hikikomori showed higher physical hostility than secondary hikikomori while showing no differences in other psychological characteristics, including alexithymia, traumatic events and quality of life (Frankova, 2019). There are few high-quality studies that have differentiated the presence of psychiatric disorders, and further research is needed to summarize the psychopathologic features of the comorbidity of hikikomori and psychiatric disorders precisely. Additionally, while the focus has been on the topology of hikikomori, including the severity, there should be a focus on the functions of why hikikomori continues. For example, identifying functional types based on operant conditioning theory may help develop individualized interventions. Furthermore, the risk of selection bias was high in much of the literature included in this review. The findings of this study may not accurately represent the actual condition of hikikomori but rather the perception of hikikomori held by the researchers. However, this was the purpose of this study. This review was limited to studies written in English and Japanese and thus may yield different results in countries where other languages are predominant.
Supplemental Material
sj-docx-1-anp-10.1177_00048674221085917 – Supplemental material for Who are hikikomori? Demographic and clinical features of hikikomori (prolonged social withdrawal): A systematic review
Supplemental material, sj-docx-1-anp-10.1177_00048674221085917 for Who are hikikomori? Demographic and clinical features of hikikomori (prolonged social withdrawal): A systematic review by Shunsuke Nonaka, Tomoya Takeda and Motohiro Sakai in Australian & New Zealand Journal of Psychiatry
Footnotes
Author contributions
S.N. contributed to conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; visualization; writing – original draft; and writing – review and editing. T.T. contributed to data curation; formal analysis; investigation; resources; and writing – review and editing. M.S. contributed to funding acquisition; investigation; resources; supervision; and writing – review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by JSPS KAKENHI (grant numbers 20K14199 and 20H01769). The funding source had no role in the study design; the collection, analysis and interpretation of data; the writing of the report; or the decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.