
Abstract
Objectives:
Physical diseases are well-established risk factor for suicide, particularly among older adults. However, little is known about the underlying mechanism of the association. This study aimed to describe the prevalence of physical diseases and their influences on the elderly in rural China and to examine the underlying mechanisms of the relationship between physical diseases and suicide.
Methods:
This matched case–control psychological autopsy study was conducted from June 2014 to September 2015. Consecutive suicide cases (242) among people aged 60 years or above were identified in three Chinese provinces. The suicide cases were 1:1 matched with living comparisons based on age, gender and residential area. Two informants for each participant were interviewed to collect data on their demographic characteristics, the severity index of physical diseases, depressive symptoms, feelings of hopelessness, mental disorders and social support.
Results:
A significant difference was found between suicide cases and living comparisons regarding the prevalence of physical diseases (83.5% vs 66.5%, p < 0.001) and their severity (11.3 ± 6.2 vs 6.7 ± 5.3, p < 0.001). Independent risks of suicide included the following: not currently married (OR = 2.81, 95% CI = [1.04, 7.62]), mental disorders (OR = 7.18, 95% CI = [1.83, 28.13]), depressive symptoms (OR = 1.15, 95% CI = [1.05, 1.26]) and feelings of hopelessness (OR = 1.51, 95% CI = [1.20, 1.90]). The structural equation model indicated that the relationship between the severity index of physical diseases and suicide was mediated by depressive symptoms, feelings of hopelessness and mental disorders.
Conclusion:
The severity and number of physical diseases were found to be correlated with suicide among the elderly in rural China, after controlling for demographic characteristics. Physical diseases elevate one’s suicide risk by increasing depressive symptoms, feelings of hopelessness and mental disorders. Efforts for suicide prevention should be integrated with strategies to treat physical diseases along with psychological interventions.
Introduction
Suicide is a major public health problem. According to the World Health Organization (WHO, n.d.), 800,000 people die by suicide every year, with 79% of global suicides occurring in low- and middle-income countries. Suicide ranks as the fifth leading cause of death in China, which accounts for an estimated 25% of international suicides or approximately 200,000 deaths every year (Weiyuan, 2009). Suicide was among the top 10 causes of years of life lost in 12 out of 33 provinces in China (Zhou et al., 2016). The standardised suicide rate for Chinese people aged 5 years and above decreased from 15.61/100,000 in 2002 to 6.61/100,000 people in 2015 (Liu et al., 2017). However, the suicide rate among the elderly population was the highest. The average annual elderly suicide rate in China was 34.5 per 100,000 in 2013–2014 (Zhong et al., 2016).
China is becoming an ageing society as the average population age continues to increase, with 143.9 million older adults (aged 65 years and above) currently (National Bureau of Statistics of China, 2017). The prevalence of physical diseases is higher among the elderly compared to other age groups and has been continually increasing (Lai et al., 2018). Often, physical diseases among the elderly are not well treated because of a lack of medical resources in rural China. Chronic diseases do not only lead to disability and impaired functioning but also cause substantial individual and socioeconomic loss (Fouad et al., 2018).
Many previous studies have found that physical diseases are closely related to elderly suicide (Harwood et al., 2006; Jia et al., 2014; Juurlink et al., 2004; Quan et al., 2002; Waern et al., 2002; Yeh et al., 2020). A psychological autopsy case–control study conducted in Shandong province found that there was a higher prevalence of physical diseases in suicide cases than in paired controls (Jia et al., 2014). Individual-level register data on people aged 65 years and above living in Denmark between 1990 and 2009 showed that multiple physical diseases have been linked to increased risks of suicide in older adults (Erlangsen et al., 2015). A population-based case–control study in Ontario indicated that a wide range of physical diseases were associated with suicide among the elderly (Juurlink et al., 2004). However, there were methodological limitations in these studies. The severity of the same physical disease might vary greatly, with it being difficult to compare these severities. Therefore, measuring physical diseases as dichotomised variables may not accurately estimate their association with suicide.
Physical diseases have been associated with depression (Holahan et al., 2010; Poole and Steptoe, 2018) and various mental disorders (Scott et al., 2016). Hopelessness is a core component of depressive symptoms, with higher levels of depressive symptoms predicting increased feelings of hopelessness (Waszczuk et al., 2016). Studies have shown that depression (Zhou et al., 2019), hopelessness (De Leo et al., 2013; Kuo et al., 2004; Steeg et al., 2016) and mental disorders (Zhou et al., 2019) are all risk factors of suicide. However, few studies have examined the mediating role of depression, mental disorders and feelings of hopelessness on the relationship between physical diseases and suicide. Particularly, little is known regarding the underlying mechanisms of this relationship. Psychological autopsy has been widely used to explore the relevant factors of completed suicides (Cavanagh et al., 2003; De Leo et al., 2013; Phillips et al., 2002) and has a high reliability and validity in China (Mo et al., 2019; Niu et al., 2018a, 2018b; Zhang et al., 2003). To measure the severity index of physical diseases (SIPD), we conducted a psychological autopsy study with a 1:1 case–control design to explore the relationship between physical diseases, depression, hopelessness, mental disorders and completed suicides. We hypothesised that physical diseases elevate the risk of completed suicide and that depression, hopelessness and mental disorders mediate the relationship between physical diseases and completed suicide. To the best of our knowledge, this is the first national psychological autopsy study focusing on the effects of physical diseases on completed suicides among the elderly population in rural China, which is an increasingly vulnerable group.
Materials and methods
Sample and sampling
A stratified multi-stage cluster sampling strategy was used to select the study sites. In the first stage, based on the gross domestic product (GDP) per capita of 31 provinces in mainland China, Shandong, Hunan and Guangxi were chosen from the top 10, 11 to 20, and 21 to 31 provinces, respectively. In the second stage, the counties in these provinces were divided into three strata based on their average income; one county in each stratum in Shandong and Hunan provinces and two counties in each stratum in Guangxi province (as each county has a small population) were randomly selected. In the third stage, 12 rural districts of 12 counties were selected. Consequently, 12 rural districts from 3 provinces were randomly selected as the study sites.
We used the death certification system in each county to consecutively collect data on completed suicides in people aged 60 years or above. All village doctors and local public health professionals involved in the death certification process were briefly trained and asked to report on all the elderly deaths by suicide to their local Centers for Disease Control and Prevention (CDC). The manner of death was determined by trained investigators after all available and relevant information was collected. The two interviewers of each suicide case would make their independent judgement. Discrepancies were resolved through consensus meeting.
Living comparisons were 1:1 matched with the suicide cases by age (±3 years old), gender and residential area. When a suicide case was identified, the investigators would list and number the elderly who were matched in age and gender in the same village. Then, one living comparison was randomly selected from the list using a computer programme. If no appropriate living comparisons were available, the investigators expanded the search to include the nearest villages.
Procedures of interview
Face-to-face interviews to collect information were conducted from 1 June 2014 to 1 September 2015. All interviewers were intensively trained for 10 days on the methods of psychological autopsy, interview skills and the administration of study instruments.
Interviews with informants of suicide cases were scheduled 2–6 months after the death, while interviews with informants of living comparisons were conducted as soon as participants and their informants were identified. Two informants for each suicide case and living comparison were identified. Generally, the first informant was the family member who lived with the person who died or the living comparison, and they were selected in the order of spouse, children, parents, brothers, sisters and other family members; the second informant was a friend, a colleague, a neighbour, a remote relative or a person who was familiar with the situation of the person who died or the living comparison. In our study, only 3 informants of 242 suicide cases refused to participate, the response rate was 99.4% (484/487). For the randomly selected living comparisons, 10 have refused us or could not be reached, and the response rate was 96.0% (242/252). For the informants of living comparisons, the response rate was 99.4% (484/487). Each informant was interviewed separately by one trained interviewer in a quiet and enclosed place. The interview time was limited to 3 hours.
The study was approved by the ethics committees of the Central South University, Shandong University and Guangxi Medical University. The aim and procedure of the research were explained to all participants. Written informed consent was obtained from participants before each interview was conducted.
Measures
Demographic characteristics
We used a self-designed questionnaire to collect the participants’ demographic characteristics, including gender, age, education, marital status, employment, family annual income and residential information.
Physical diseases and severity index
Participants were asked to report their physical diseases, which were understood as any acute or chronic illness and/or condition causing significant impairment and that may lead to long-term impairment, disability and/or death (International Association for Hospice & Palliative Care, 2014). Diagnoses of physical diseases, as made by physicians, were recorded. When necessary, medical records were reviewed with consent. We further evaluated the severity of the illnesses using five items from the SIPD: two questions about the effect of the participant’s physical diseases on his or her daily life and mental condition, with each being scored on a scale of 0 to 4; two questions about financial burdens and the physical and mental burden on the family that were caused by the physical diseases, with each being scored from 0 to 4; and one question on whether the physical diseases were a threat to the participant’s life, which was scored from 0 to 4. The possible total scores of the SIPD ranged from 0 to 20, with a higher score indicating a more serious impact of physical diseases. The Cronbach’s alpha coefficient of the SIPD was 0.941 in our study.
Mental disorders
The Chinese version of the Structured Clinical Interview for DSM-IV (SCID) was used to define current diagnoses of mental disorders. The diagnoses were made by psychiatrists in consensus meetings in which all information, including the SCID interviews from both the informants and previous medical records, were presented. Four categories of diagnoses were included: mood disorders, schizophrenia and other psychotic disorders, alcohol dependence and anxiety disorders. The diagnoses of personality disorders or uncommon disorders among the elderly in rural China (i.e. onset of mental disorders in childhood and adolescence, eating disorders and illicit drug abuse) were not included.
Duke Social Support Index
Social support in the last week before the death/investigation was measured by the 23-item Duke Social Support Index (DSSI), with scores ranging from 11 to 45 (a higher score indicates a higher level of social support). The DSSI has been used in a previous psychological autopsy study in China and showed satisfactory reliability and validity (Zhang et al., 2003).
Geriatric Depression Scale
We used the 30-item Chinese revision of the Geriatric Depression Scale (GDS) to assess the participants’ level of depression (Yesavage et al., 1982). This instrument is frequently used to screen depression among the elderly, with scores ranging from 0 to 30; a higher score indicates more severe depressive symptoms (Chan, 1996). The GDS was validated among the elderly in rural China in this study, with its intraclass correlation coefficient (ICC) value being 0.590 (Niu et al., 2018b).
Beck Hopelessness Scale
The four-item Beck Hopelessness Scale (BHS-4) was used to assess the levels of hopelessness among the participants. This instrument has since been revised (Aish et al., 2001), with participants being asked about their views on the future in the last week before the death/investigation. Two of the four items were reverse-scored (a negative answer indicated hopelessness). Each item had four options: strongly agree, agree, undecided, disagree or strongly disagree, which were scored from 1 to 5, respectively. The total scores of the BHS-4 ranged from 4 to 20, with a higher score indicating a higher sense of hopelessness.
Integration of information from different sources
As the answers from the two informants could differ, they needed to be integrated. For the demographic characteristics, we relied on the information that was provided by the first informant. For information on physical diseases, mental disorders, DSSI, GDS and BHS-4, the answers that hypothetically correlated to an elevated suicide risk were used. The rationale behind this was that a targeting behaviour may exist if one of the two informants had observed it. For instance, a positive answer for an item on the GDS was used when one of the two informants reported it as positive; similarly, a higher prevalence of physical diseases and mental disorders, higher scores on the BHS-4 and lower scores on the DSSI were used.
Statistical methods
Descriptive analyses, χ2 tests, t-tests and rank-order tests were used to describe and compare the demographic characteristics, physical diseases, mental disorders, social support, depressive symptoms and hopelessness in both the suicide cases and the living comparisons. Marital status was dichotomised into currently married and not currently married, with the former including currently married and living together and the latter including never married, divorced, widowed and separated. Family annual income was categorised into three groups based on the 33rd and 66th percentiles: <3600, 3600–10,000 and >10,000 yuan. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs), as derived from the conditioned multivariable logistic regression, indicated the associations between risk factors and suicide; the scores of the SIPD, DSSI, GDS and BHS were used as continuous variables to indicate the severity of physical diseases, higher social support, severity of depressive symptoms and a higher sense of hopelessness, respectively. The backward stepwise (likelihood ratio) method was used for the logistic regression. All analyses were conducted using SPSS 24.0 for Windows (IBM Corporation, Armonk, NY, USA). All the reported p-values were two-sided, with p-values less than 0.05 being considered statistically significant.
The theoretical model was estimated with a structural equation model. We speculated that physical diseases do not directly cause suicide but that they do elevate its risk through their effects on depressive symptoms, hopelessness and mental disorders. Depressive symptoms not only had a direct effect on suicide but also had an indirect effect by increasing hopelessness. Hopelessness and mental disorders had direct effects on suicide, with the latter being correlated with depressive symptom. The χ2 test, goodness-of-fit index (GFI), adjusted goodness-of-fit (AGFI), Tucker–Lewis index (TLI) and root mean square error of approximation (RMSEA) were used to estimate the GFI of the theoretical model. These analyses were performed using AMOS 21.0 for Windows.
Results
Demographic characteristics, social support, depressive symptoms and hopelessness in the suicide cases and living comparisons
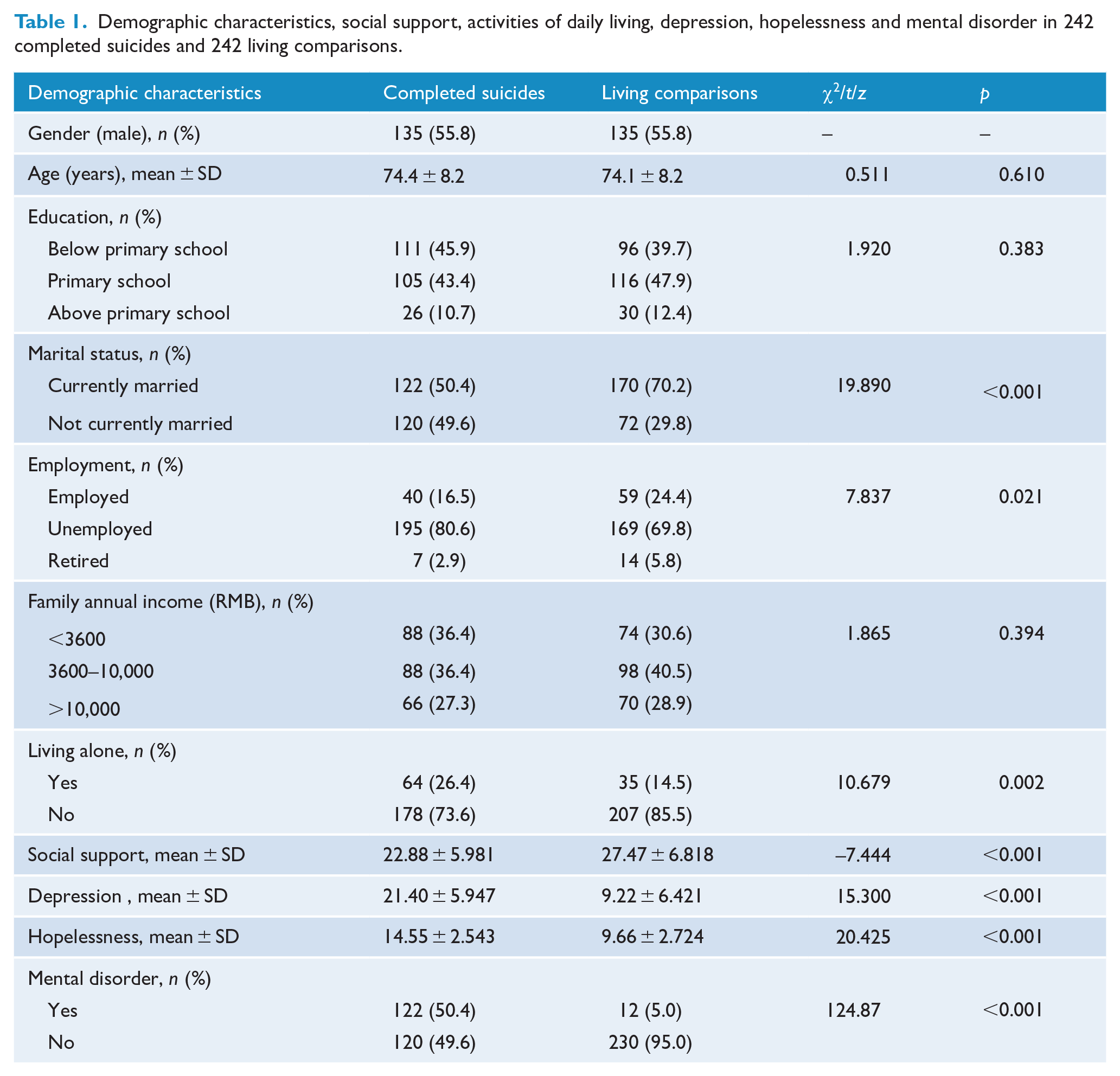
A total of 242 suicide cases and 242 living comparisons were assessed in this study. As shown in Table 1, 125 (55.8%) of the participants were male, with their mean (SD) age being 74 (8) years. Compared with the living comparisons group, suicide cases were more likely to be not currently married, unemployed and living alone. No statistically significant difference was found in the education or family annual income between the suicide cases and living comparisons (all p-values > 0.05). However, the suicide cases had significantly lower social support, as well as more severe depressive symptoms and feelings of hopelessness (all p-values < 0.001).
Demographic characteristics, social support, activities of daily living, depression, hopelessness and mental disorder in 242 completed suicides and 242 living comparisons.
Physical diseases and severity index of suicides and comparisons
Table 2 shows that 202 (83.5%) suicide cases and 161 (66.5%) living comparisons had at least one diagnosis of physical diseases. Physical diseases increased the suicide risk, with a crude OR of 2.84 (95% CI = [1.67, 4.84]) for individuals with one physical disease and 2.51 (95% CI = [1.53, 4.11]) for those with two or more physical diseases. The adjusted ORs for one and two physical diseases were 3.10 (95% CI = [1.76, 5.45]) and 2.95 ([1.72, 5.07]), respectively, after controlling for marital status, employment and living alone.
Prevalence of physical diagnoses and associated risk for suicide among the rural elderly in China.
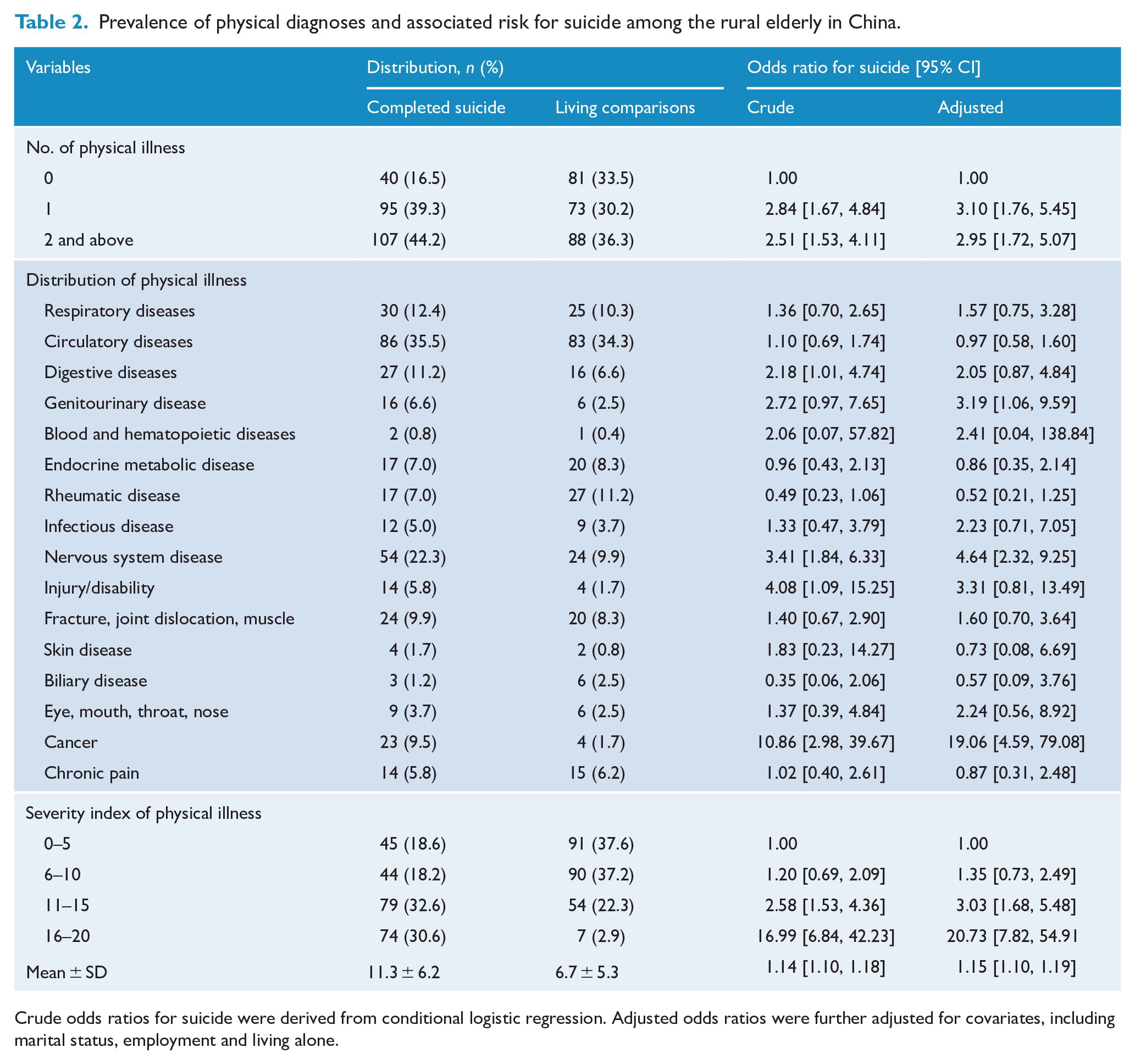
Crude odds ratios for suicide were derived from conditional logistic regression. Adjusted odds ratios were further adjusted for covariates, including marital status, employment and living alone.
Circulatory disease was the most common illness in both the suicide cases and the living comparisons (Table 2). Using an individual with no physical diseases as a reference showed that digestive diseases, nervous system diseases, injury or disability, and cancer were associated with a higher risk of suicide among the elderly in rural China. However, genitourinary diseases, nervous system diseases and cancer were associated with a high risk of suicide among the elderly in rural China after controlling for marital status, employment and living alone.
The mean scores for the SIPD were significantly higher in the completed suicides than in the living comparisons (p < 0.001). A high SIPD increased the suicide risk, with a crude OR of 1.14 (95% CI = [1.10, 1.18]). The adjusted OR was 1.15 (95% CI = [1.10, 1.19]) after controlling for marital status, employment and living alone.
Risk of elderly suicide in China: conditional multivariable regression
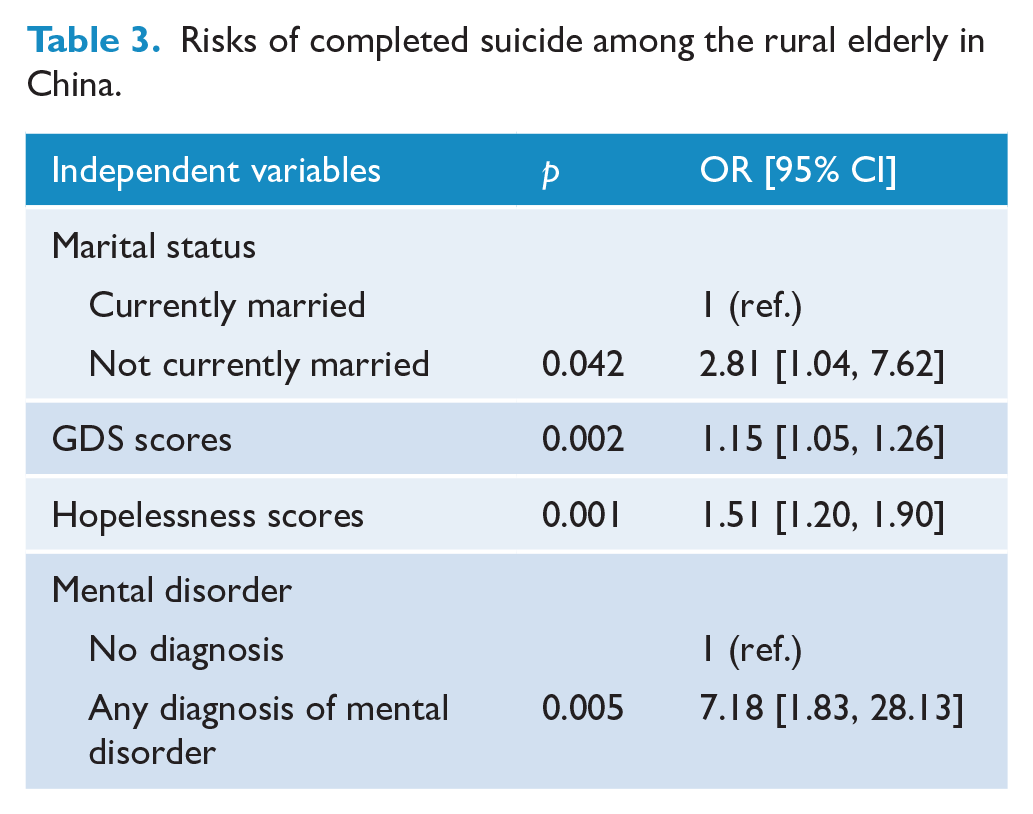
A conditioned multivariable logistic regression was used to determine the risk factors of suicide. The independent variables included in this model were as follows: marital status, employment, living alone, diagnosis of mental disorders (yes or no), SIPD, social support, hopelessness and depressive symptoms (the SIPD, DSSI, BHS-4 and GDS scores were used as continuous variables). The four variables in the final model were as follows: marital status (OR = 2.81, 95% CI = [1.04, 7.62]), depressive symptoms (OR = 1.15, 95% CI = [1.05, 1.26]), hopelessness (OR = 1.51, 95% CI = [1.20, 1.90]) and mental disorders (OR = 7.18, 95% CI = [1.83, 28.13]) (Table 3).
Risks of completed suicide among the rural elderly in China.
Testing the structural equation model
Based on the results of the conditional multivariable regressive model, we established two path analysis models to explore the relationships between SIPD, depressive symptoms, hopelessness, mental disorders and suicide. The theoretical model was not well validated (Model 1). The χ2 test showed a significant probability of >0.05, χ2(1) = 3.528, p = 0.060. The GFI analysis showed that the model fit was high: GFI = 0.997, AGFI = 0.956, TLI = 0.977 and RMSEA = 0.072. The SIPD had no direct effects on suicide.
We then removed the path between SIPD and created Model 2. The verification analysis of the structural equation model proved that the modified model was well validated (Model 2). The χ2 test showed a significant probability of >0.05, χ2(1) = 2.272, p = 0.103. The GFI analysis showed that the model fit was high: GFI = 0.996, AGFI = 0.972, TLI = 0.988 and RMSEA = 0.051. The standardised total effects of the predictors on suicide were as follows: SIPD = 0.350, depressive symptoms = 0.604, hopelessness = 0.329 and mental disorder = 0.156 (see Figure 1).
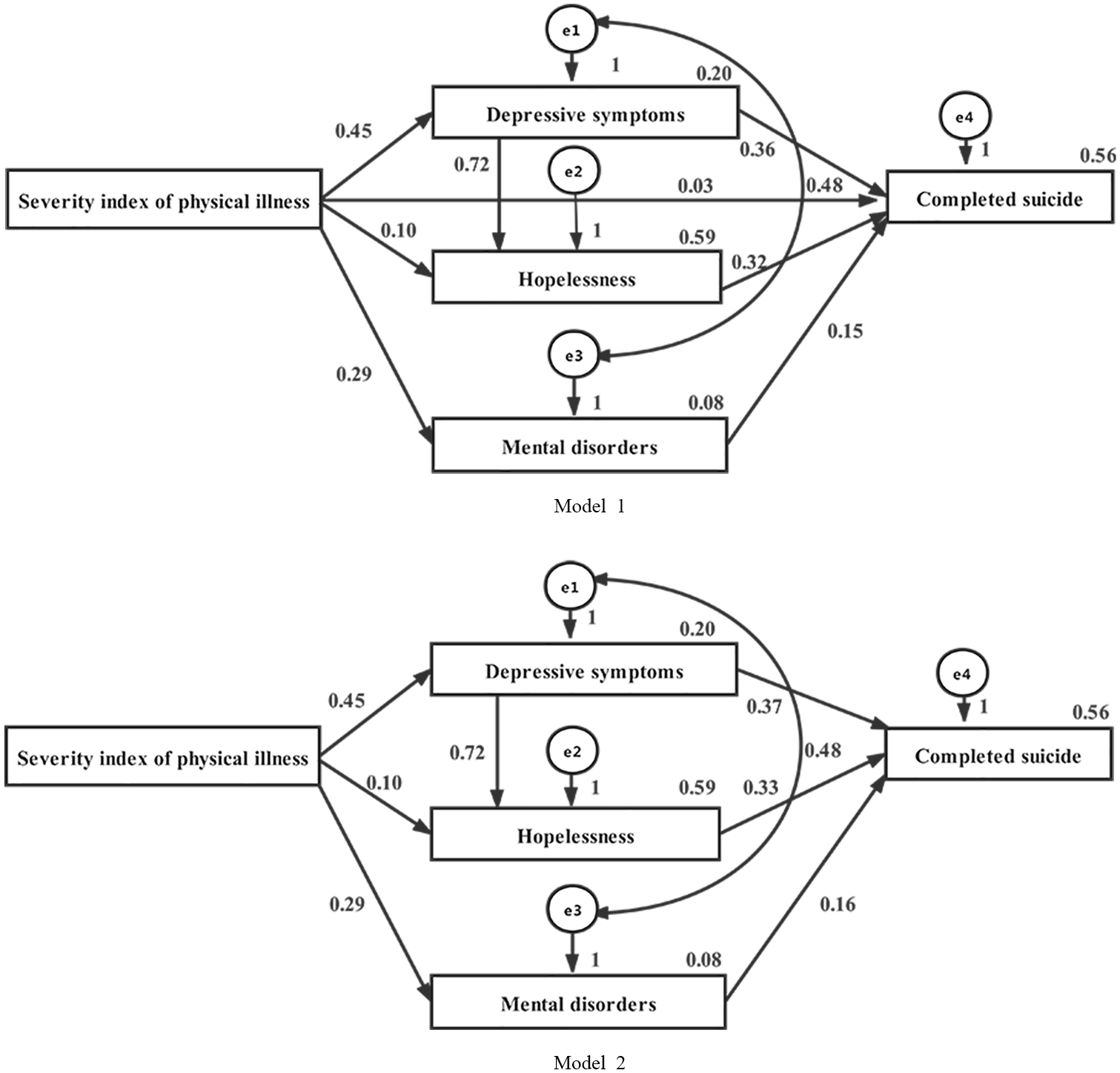
Model 1: Physical diseases not only have a direct effect on suicide but also have an indirect effect by increasing the risk of completed suicide. Moreover, depression, hopelessness and mental disorders mediate the relationship between physical diseases and completed suicide. The mediating effects of these factors on the relationship between the severity index of physical diseases and suicide were examined using a structural equation model: CMIN = 3.528, CMIN/DF = 3.528, p = 0.060, GFI = 0.997, AGFI = 0.956, TLI = 0.977 and RMSEA = 0.072. Model 2: The relationship between the severity index of physical diseases and suicide is mediated by depressive symptoms, hopelessness and mental disorders. The mediating effects of these factors on the relationship between the severity index of physical diseases and suicide were examined using a structural equation model: CMIN = 4.544, CMIN/DF = 2.272, p = 0.103, GFI = 0.996, AGFI = 0.972, TLI = 0.988 and RMSEA = 0.051.
Discussion
We found that physical diseases were significantly more prevalent in suicides than in living comparisons (83.5% vs 66.5%, p < 0.05). The structural equation model showed that physical diseases elevated suicide risk by increasing depressive symptoms, hopelessness and mental disorders. This may explain our finding that physical diseases were no longer associated with suicide after controlling for these mediating factors with conditional multivariable regression.
We found that having one or more physical diseases were significantly more prevalent among suicides than in living comparisons (39.3% vs 30.2%, 44.2% vs 36.3%, all p < 0.05). This finding is consistent with previous studies on rural residents of modern China (Jia et al., 2014). Cancer, injury/disability, nervous system diseases and digestive diseases were also significantly more prevalent in suicides than in living comparisons (85.2% vs 14.8%, 77.8% vs 22.2%, 69.2% vs 30.8%, 62.8% vs 37.2%, all p < 0.05), with the difference remaining significant after controlling for sociodemographic characteristics. This finding is consistent with previous studies that people with cancer, nervous system diseases, prostate disorders and male genital disorders had a significantly increased risk of suicide (Erlangsen et al., 2015; Fassberg et al., 2016; Quan et al., 2002).
Psychological autopsy is considered an effective method to explore the relevant factors of completed suicide (Cavanagh et al., 2003; De Leo et al., 2013; Niu et al., 2018a, 2018b; Phillips et al., 2002; Zhang et al., 2003). However, a measurement of severity of physical diseases among psychological autopsies was not available. Our study used SIPD to measure the severity of physical diseases. The internal consistency was 0.941, which indicates that the SIPD was both reliable and valid. The SIPD was also significantly higher in suicides (11.3 ± 6.2 vs 6.7 ± 5.3, p < 0.05) and a dose–response relationship between severity index and suicide was observed after controlling for sociodemographic characteristics.
The prevalence of mental disorders, the GDS scores and the BHS-4 scores among people who completed suicide were significantly higher than those in the living comparisons. Mental disorders, depression and hopelessness were independent risk factors for elderly suicide after controlling for other relevant factors. This finding is consistent with previous studies (De Leo et al., 2013; Hu et al., 2005; Liu et al., 2018; Ngamini Ngui et al., 2015; Phillips et al., 2002; Ribeiro et al., 2018; Zhang et al., 2010; Zhang and Li, 2013). However, little is known about the factors affecting the relationship between physical diseases and suicide. Our study found that physical diseases elevated the risk of completed suicide and that depression, hopelessness and mental disorders mediated the relationship between physical diseases and completed suicide. The structural equation model showed that the SIPD, depressive symptoms, hopelessness and mental health explained 56% of the variance in complete suicide among the elderly in rural China. This finding suggests that suicide prevention strategies for people with physical diseases should focus on the treatment of these diseases, psychological intervention for any depression and desperation, and the treatment of mental disorders. The accessibility of health care in rural China is low, and more importantly, the quality of health care is even lower. The cost of health care is relatively high considering the very low income of older adults in rural China. All these real-world issues may have shaped the response to physical illness of older adults and should be taken into consideration when developing suicide prevention strategy through the management and treatment of physical illness.
However, several limitations should be considered when interpreting our results. First, the rate of physical diseases reported by the informants may be lower than the actual prevalence. The presence of physical diseases in this study was verified by a medical institution before suicide or investigation. The number of physical diseases might be underreported due to a lack of regular health check-ups accessible to the elderly in rural China. Second, psychological autopsy studies have methodological limitations. Using proxy informants, the impact of bereavement on informants of suicide decedents and the retrospective information collection might have an impact on the quality of data. The different types of informants between suicides and living comparisons could also have impaired the comparability of data. Third, our strategy of selecting the higher scores by the two informants might have elevated the scores of scales. Fourth, we did not assess cognitive impairment of suicides or living comparisons, so we were not able to explore the relationship between dementia and suicide. Finally, the interviews of the informants of the suicide cases were conducted 2–6 months after death, which may have affected the reliability of the data.
Conclusion
Physical diseases can elevate the risk of suicide by increasing depressive symptoms, hopelessness and mental disorders. Efforts for suicide prevention should be integrated with strategies to treat any physical diseases along with psychological interventions.
Footnotes
Acknowledgements
The authors would like to thank village cadres for guiding them to visit each household in the rural regions of Hunan, Shandong and Guangxi provinces, China.
Author Contributions
C.J., Z.M. and L.Z. conceived and designed the study. G.W., C.J. and Z.M. collected the data. G.W. and L.Z. analysed and interpreted the data. G.W. drafted the article, while L.Z., C.J. and Z.M. critically revised it for intellectual consent. All authors gave final approval to the version submitted for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the American Foundation of Suicide Prevention to Dr Liang Zhou (Grant No. SRG-0-169-12), the Fundamental Research Funds for Shenzhen Science and Technology Innovation Commission (Grant No. JCYJ20170413101017457) and the Natural Science Foundation of Guangxi Province to Dr Zhenyu Ma (Grant No. 2014GXNSFBA11816).
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.