
Abstract
Objective:
The risk of suicide in contemporary serving and ex-serving Australian Defence Force personnel is an area of significant concern, driving government-directed inquiries, community campaigns and most recently, the establishment of a permanent National Commissioner for Defence and Veteran Suicide Prevention. This concern is mirrored in international militaries and despite investment in prevention programmes, suicide is a leading cause of death in military populations. This review seeks to summarise recent findings from Australian research regarding the magnitude and factors associated with suicide and suicidality in contemporary serving and ex-serving Australian Defence Force populations and discusses research findings, implications and future opportunities.
Methods:
Initial review of the prevalence of suicide and suicidality in the general community and military populations is presented, followed by review of recent research findings pertaining to suicides and suicidal thoughts, plans and attempts in contemporary serving and ex-serving Australian Defence Force personnel. Key findings are presented from the 2010 Australian Defence Force Mental Health and Wellbeing Prevalence Study and the 2015 Transition and Wellbeing Research Programme.
Results:
Differences between serving and ex-serving Australian Defence Force cohorts were observed, with rates of completed suicide in ex-serving Australian Defence Force males more than double that of serving Australian Defence Force males, and increased risk for suicidality observed among those who had recently transitioned out of full-time Australian Defence Force service. Risk for increased suicidality and completed suicide is particularly evident for younger males of lower ranks, and those who have been medically discharged.
Conclusions:
The findings provide insight into career phases and groups that should be followed-up and targeted for prevention and early intervention programmes, including prior to and several years following transition out of full-time military service. Further research to better understand the factors that influence those who develop suicidal ideation, and those who progress to plans and attempts, will inform a more sophisticated approach to suicide prevention programmes.
Completed suicides and suicidality are a significant concern across the entire community; however, there are several groups identified as being at particular risk. One group which has generated a great deal of research and public commentary both nationally and internationally is the military (McFarlane et al., 2011). In Australia, following years of government-directed inquiries (e.g. Foreign Affairs, Defence and Trade Reference Committee, 2017; National Mental Health Commission [NMHC], 2017), media commentary and community campaigns for action, a permanent National Commissioner for Defence and Veteran Suicide Prevention was announced in early 2020 (Prime Minister of Australia, 2020). Within the context of the prevalence rates of completed suicides and suicidality within the general community and other military populations, this review summarises the research findings regarding completed suicides and suicidality in the contemporary Australian Defence Force (ADF) serving and ex-serving populations and discusses implications as well as research gaps and future opportunities.
Prevalence of suicide and suicidality in the community
Prior to reviewing suicidality in military and veteran populations, it is useful to consider suicidality in the general community. Suicide is one of the leading causes of death around the world. The World Health Organization (WHO, 2019) estimates almost 800,000 people die by suicide each year and for every suicide there are over 20 suicide attempts. Research has supported the existence of a continuum of suicidal expression in the general community, whereby suicidality, including suicidal ideation and suicide plans and attempts, predominantly precede future completed suicides. Suicide attempts in particular are a risk factor for subsequent completed suicides (Nock et al., 2008; WHO, 2019). It has been estimated that about a third of those that report suicide ideation will go on to make a suicide attempt, and over 60% of these transitions from thoughts to attempts occur within 12 months of initial onset of suicidal ideation (Nock, 2016). Research focusing on suicidality has been undertaken as an opportunity to identify those factors that may prevent completed suicides. Suicidal thoughts, plans and attempts are also issues of concern in their own right, with the potential to cause significant distress to individuals, their families, friends and work colleagues; negatively affect functioning and productivity and even lead to permanent disability (Franklin et al., 2017; NMHC, 2017).
As in other nations, completed suicides and suicidality are issues of significant concern within the Australian population. Suicide is currently the leading cause of death among Australians aged between 15 and 44 years and is the second leading cause of death among those aged 45 to 54 years (Australian Bureau of Statistics [ABS], 2019). Suicide also accounts for the highest number of years of potential life lost, an average of 36.7 years. The standardised 2018 death rate was 12.1 deaths per 100,000, contrasting with rates over the past decade ranging from 10.5 (2011) to 12.9 (2015). Suicide was ranked the 14th leading cause of death in 2018, with males dying by suicide at a rate three times higher than females. In 2018, the standardised suicide death rate for males was 18.6 deaths per 100,000 and for females, it was 5.7 deaths per 100,000 people (ABS, 2019).
There is less recent data available on the rates of suicidality, such as suicidal thoughts, plans and attempts, in the Australian population. In the 2007 National Survey of Mental Health and Wellbeing of Australians aged 16 to 85 years, 0.4% of the community sample reported that they had attempted suicide in the preceding 12 month period (ABS, 2008). Further analysis of this dataset found that 13.3% of Australian adults reported suicidal ideation during their lifetime, 4.0% reported making a suicide plan and 3.3% reported a suicide attempt in their lifetime. Females were found to have higher prevalence of suicidal ideation, plans and attempts than males (Slade et al., 2009). More recent reports analysing rates of hospitalisation due to intentional self-harm highlight that females are significantly more likely to be hospitalised than males. Notably, these data did not distinguish between suicidal intent and intentional self-harm without suicidal intent (Australian Institute of Health and Welfare [AIHW], 2014).
Prevalence of completed suicides and suicidality in military populations
While there is variation in the rates of completed suicides and suicidal thoughts, plans and attempts across different militaries due to demographic factors, different recruitment protocols and methods of assessment and different health care systems (Sareen et al., 2016), there is substantial evidence that concern regarding the suicide risk for this population is warranted.
Most of Australia’s military allies report lower or comparable rates of completed suicide than in the age- and/or sex-matched general community, including in the United States (US; Tucker et al., 2019), United Kingdom (UK; Ministry of Defence, 2020), Canada (Rolland-Harris, 2019) and New Zealand (NZ; Stuart and Bennett, 2017). One notable exception is the suicide rate in US active service Army personnel which first exceeded the general community rate in 2008 (US Army Public Health and Center, 2017) and resulted in the initiation of the US Army Study to Assess Risk and Resilience in Servicemembers (or Army STARRS). This is the largest research study ever conducted on suicide, mental health risk and resilience in military personnel (Ursano et al., 2014, 2017; Ursano and Stein, 2017).
In contrast, rates of completed suicide in ex-serving military personnel in some countries are much higher than both current serving military personnel and civilians, including those from the United States (US Department of Veterans Affairs, 2019) and Canada (Simkus et al., 2017). This is particularly evident among younger males of lower ranks (Simkus et al., 2017; US Department of Veterans Affairs, 2019). Although there is less research available on suicidal ideation, plans and attempts, the available findings likewise indicate increased rates in veterans compared to both current serving and community samples in the United States (Nock et al., 2008), the United Kingdom (Jones et al., 2019) and Canada (Simkus et al., 2017).
Completed suicides in serving and ex-serving ADF personnel
Until recently, data on completed suicides in serving and ex-serving ADF personnel were somewhat limited. Drawn primarily from Defence records of suspected or completed suicides of serving ADF personnel (AIHW, 2018; Bounty et al., 2004; Gisler and Sadler, 2000), there was no comparable database of suspected or completed suicides in the ex-serving ADF population (NMHC, 2017). In addition, most research undertaken on ex-serving ADF members had examined those who had served in specific conflicts, such as Korea, Vietnam and the Gulf War and therefore was not necessarily applicable to ADF members serving in more recent conflicts nor to those who have recently transitioned from full-time military service (Dunt, 2009).
In 2017, a suicide data matching exercise was conducted for the Departments of Defence (Defence) and Veterans’ Affairs (DVA) by the AIHW to establish the number of serving and ex-serving ADF members who have served since 2001 and have died by suicide and to determine characteristics that may be associated with the risk of suicide. The study involved matching data between Defence personnel records and both the National Death Index and the State Coroners’ records. Since 2018, AIHW has released annual reports examining suicides in current serving (including Reservists) and ex-serving ADF personnel who had completed at least 1 day of ADF service since 2001, and 3-year rolling aggregations are used to report more detailed information. As each report only includes certified suicides, each annual release updates previously published numbers of suicides to incorporate any changes to the source data. Furthermore, as the ex-serving population increases each year as more people discharge from the ADF, changes in the number of suicides over time are interpreted in the context of the changing size of the population.
The first reports were released in 2017 and 2018 and examined the incidence and risk factors associated with the completed suicide of ADF members with at least 1 day of ADF service between 2001 and 2015 (AIHW, 2017, 2018). Of the 325 certified suicide deaths that occurred during this period, 93% were male, and at the time of their death, 51% were no longer serving in the ADF. Results indicated that the suicide rates for males serving full-time in the ADF and the Reserves at the time of their death were significantly lower than similar aged males in the Australian community (AIHW, 2017). The crude suicide rate in ex-serving ADF males was more than twice as high as males serving full-time or in the Reserves (26 suicide deaths per 100,000 people, compared with 11 and 12 per 100,000 respectively). After adjusting for age, the suicide rate for all ex-serving ADF males was 14% higher than an age-matched community sample, however this difference was not statistically significant. This difference between ex-serving ADF members and similar aged males from the Australian community was particularly pronounced in the younger age groups, with ex-serving males aged 18 to 24 years being two times more likely (37 per 100,000 compared with 19 per 100,000) and ex-serving men aged 25 to 29 years old being 1.4 times more likely to die by suicide than Australian men of the same age (31 per 100,000 compared to 22 per 100,000). Due to the low number of females among the 325 certified deaths, detailed analysis of this group was not undertaken.
Military service-related risk factors associated with an increased risk of completed suicide among ex-serving ADF males included type of discharge and rank. The odds of suicide for those who had medically discharged were 1.9 times the odds for those who discharged voluntarily. The odds of suicide for those who had discharged at any rank level other than commissioned officers (all ranks from Private through to Warrant Officer) were 2.2 times the odds of those who had discharged as commissioned officers (all ranks from Lieutenant and higher). While the length of service was not a significant predictor of death by suicide, there were indications that those with less than 1 year of military service were at greater risk than those who had served 10 years or more. Service branch (Navy, Army or Air Force) and whether or not the ADF member had been on operational service did not predict death by suicide (AIHW, 2018).
In the 2019 update (AIHW, 2019), it was reported that between 2001 and 2017 there were 419 suicides in current serving, Reserve and ex-serving ADF personnel (a further 94 certified deaths since the last data extraction 2 years prior in 2015). In this study, the age-adjusted suicide rate was 48% lower among current serving ADF males and 18% higher in ex-serving males than Australian men. This represents an increase of 4% (since the first reporting of the rate in 2017) among ex-serving men compared to their civilian counterparts. The suicide rate remained particularly high for ex-serving men aged under 30 years old. In 2014-2016, ex-serving men aged under 30 had a suicide rate 2.2 times higher than Australian men the same age. For the first time there were sufficient data to analyse suicide rates in the female ex-serving cohort. There were 21 suicide deaths among ex-serving females and the age-adjusted rate of suicide was 115% (or 2.15 times) higher than that of Australian women. All of these findings were statistically significant.
In the most recent analysis (AIHW, 2020), it was reported there had been 465 certified deaths by suicide between 2001 and 2018 among males and females with at least one day of ADF service since 1 January 2001, and of these, 267 (57%) were ex-serving personnel. In 2016–2018, the age-adjusted rate of suicide in serving males and Reserve males was 37% and 47%, respectively, lower than in Australian males, and these findings were significantly different. For the same 3-year period, the age-adjusted rate of suicide in ex-serving males was 19% higher than in Australian males, but this difference was not significant. The suicide rates for 2016–2018 in ex-serving males aged under 30 and over 30 years were not significantly different from each other. However, they remained higher than the rates for serving and Reserve males for both age groups (under and over 30 years). The report also included analysis of suicide rates in ex-serving males by discharge reason (voluntary, medical or other involuntary) between 2007 and 2018. Although ex-serving males who discharged voluntarily had similar rates of suicide to Australian males, ex-serving males who had discharged on medical grounds had significantly higher rates of suicide than Australian males.
Suicidal thoughts, suicide plans and attempts in current serving and recently transitioned ADF members
The most comprehensive assessment of the prevalence of suicidal thoughts, plans and attempts (suicidality) among current serving ADF personnel was conducted as part of the 2010 ADF Mental Health and Wellbeing Prevalence Study (McFarlane et al., 2011). In this study, 12-month suicidality was examined using the following four items in a self-report survey: ‘in the last 12 months, have you ever felt that your life was not worth living?’ (ideation); ‘in the last 12 months, have you ever felt so low that you thought about committing suicide?’ (ideation); ‘in the last 12 months, have you made a suicide plan?’ (planning); ‘in the last 12 months, have you attempted suicide?’ (attempt). Responses were restricted to ‘yes’ or ‘no’, and data were analysed either as separate items or dichotomised into whether the participant endorsed any suicidality item (‘any suicidality’) or whether they endorsed none of the suicidality items. The first three items were adapted from the National Survey of Mental Health and Wellbeing (ABS, 2008), and the final item was devised by researchers for use in the study. As part of this research, all Regular ADF personnel serving in 2010 (n = 50,049) were invited to complete a self-report survey, and it was completed by n = 25,566. As the ADF population characteristics are known (e.g. sex, Service branch, medical status), it was possible to compare personnel who had responded to the survey with personnel who had not. This enabled weighting of the data to provide estimates of the prevalence that were representative of the entire serving Regular ADF in 2010 (McFarlane et al., 2011).
The estimated prevalence of 12-month suicidality (ideation, plans or attempts) in current serving Regular ADF personnel in 2010 was 4.0%. The estimated prevalence of 12-month suicidal ideation was 3.9%, 1.1% reported making a suicide plan and 0.4% reported attempted suicide in the last 12 months. These data were compared to a sociodemographically matched sample (based on employment status, that is, employed/not employed, sex and age) from the Australian community (Table 1), and it was estimated that the 12-month rates of ideation and planning were higher in the ADF sample than in the community sample, but there was not a significant difference between rates of suicide attempts. Suicidal ideation was 39% more likely to be reported by females, but there were no significant differences between females and males in plans or attempts. There was a significant interaction with 12-month mental disorder (defined as an International Classification of Disease Version 10.0 [ICD-10]: WHO, 2011) affective, anxiety or alcohol disorder], with 2.8% of ADF personnel who met the criteria for an ICD-10 mental disorder, estimated to have attempted suicide in the preceding 12 months, compared to an estimated 0.1% of those with no mental disorder.
Estimated prevalence of suicidality by sex in the ADF compared to the Australian community (standardised by age, sex and employment status).
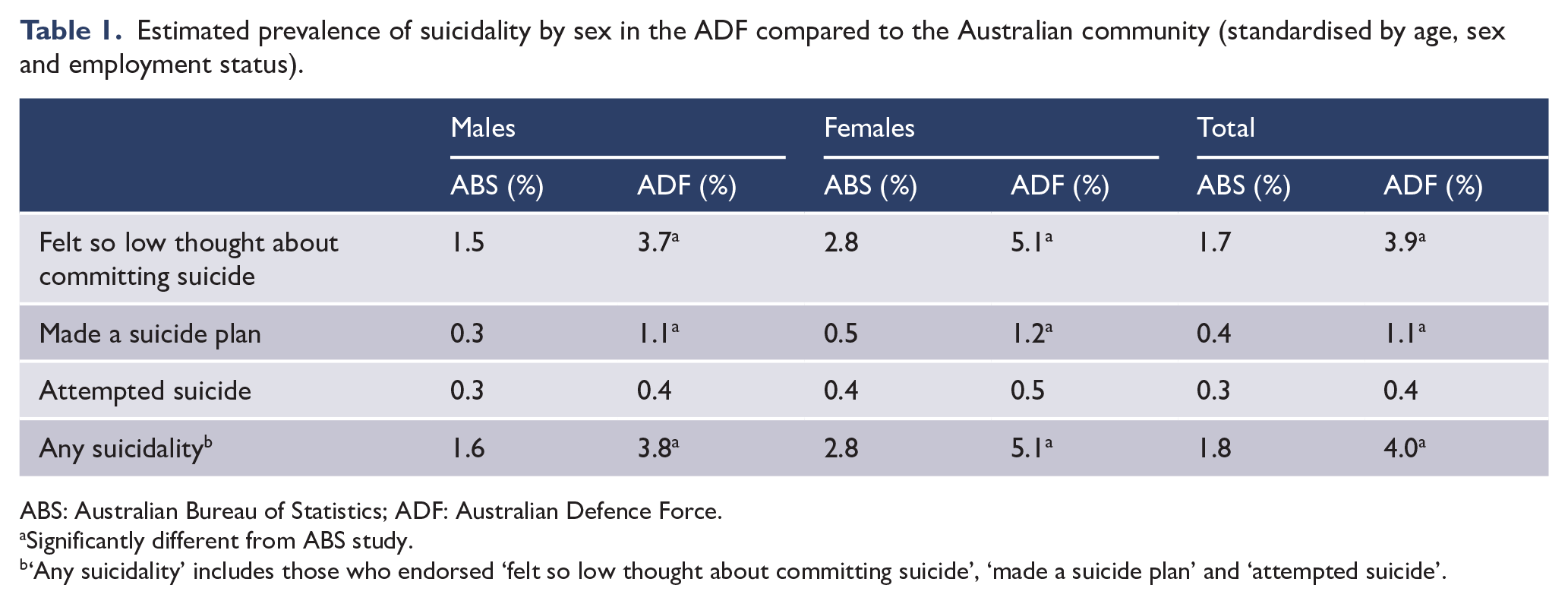
ABS: Australian Bureau of Statistics; ADF: Australian Defence Force.
Significantly different from ABS study.
‘Any suicidality’ includes those who endorsed ‘felt so low thought about committing suicide’, ‘made a suicide plan’ and ‘attempted suicide’.
Further analysis of this suicidality data (Van Hooff et al., 2013) indicated that suicidality was significantly more likely to occur among ADF personnel who had experienced interpersonal (e.g. direct combat, rape) and environmental (e.g. life threatening accident) trauma in their lifetime, and there was a trend of increasing severity in suicidality as the number of traumas accumulated. Stigmas and barriers relating to help-seeking, perceived poor support from peers and supervisors and experiencing workplace bullying also significantly increased the risk of self-reported suicidal thoughts, plans and attempts. The majority of ADF personnel who met criteria for an ICD-10 affective, anxiety or alcohol disorder had an increased risk of suicidality, with this risk increasing with multiple disorder types. Suicidality risk was significantly increased if there was concurrent mental disorder as well as a lifetime history of interpersonal trauma (Van Hooff et al., 2013).
The Transition and Wellbeing Research Programme, funded by DVA and Defence, was initiated by a consortium of Australian researchers in 2014 to address key research gaps relating to the impact of contemporary military service on the mental, physical and social health of serving and ex-serving ADF personnel and their families. Of particular interest was determining the health and wellbeing of those who had recently transitioned out of full-time military service in the 5 years between 2010 and 2014. The period of transition, and the impact on the health and wellbeing of military personnel and their families, is a growing field of international research, with evidence of deterioration in reported physical and mental health and general wellbeing in some individuals after they have left full-time (e.g. Shields et al., 2016; Van Hooff et al., 2018) or part-time military service (Wang et al., 2020). The Transition and Wellbeing Research Programme built upon the ADF research undertaken as part of the Military Health Outcomes Programme (MilHOP), which included the 2010 ADF Mental Health Prevalence and Wellbeing Study (McFarlane et al., 2011), the 2012 Middle East Area of Operations (MEAO) Prospective Study (Davey et al., 2012) and the 2012 MEAO Census Study (Dobson et al., 2013).
Suicidality and mental health data were collected for the Transition and Wellbeing Research Programme in 2015 via an online self-report survey and telephone administration of the WHO Composite International Diagnostic Interview – Version 3.0 (CIDI; Kessler and Üstün, 2004) to examine lifetime and 12-month mental disorder according to the ICD-10 (WHO, 2011). Twelve-month self-reported suicidality was assessed using the same four items used in the MilHOP studies. Notably, the Transition and Wellbeing Research Programme included the follow-up of individuals who participated in the MilHOP, providing the opportunity to match data in this population across two time points and examine changes over time.
Three reports published within the Transition and Wellbeing Research Programme included analysis of the suicidality data items: Mental Health Prevalence Report (Van Hooff et al., 2018), Mental Health Changes Over Time: A Longitudinal Perspective Report (Bryant et al., 2019) and Impact of Combat Study Report (Lawrence-Wood et al., 2019). The Mental Health Prevalence Report (Van Hooff et al., 2018) highlights the significant level of ICD-10 mental disorders and significantly poorer self-reported mental health (psychological distress, depression, alcohol, suicidality and Posttraumatic Stress Disorder [PTSD] symptoms) in those who had transitioned out of full-time service between 2010 and 2014 versus those who were still serving in the full-time ADF in 2015 (referred to as the 2015 Regular ADF).
Consistent with the methodology used for the 2010 ADF Mental Health and Wellbeing Prevalence Study, the survey data analysed for the Mental Health Prevalence Report (Van Hooff et al., 2018) were weighted using distinct strata for sex, Service branch, rank and medical fitness. In relation to suicidality (Table 2), an estimated 21.7% of the Transitioned ADF reported suicidal ideation or behaviour in the last 12 months; 28.9% had felt their life was not worth living; 21.2% felt so low they had thought about taking their own life (both indications of suicidal ideation); 7.9% had made a suicide plan; and 2.0% had attempted suicide in the preceding 12 months (Van Hooff et al., 2018). Further analysis indicated an increased risk for any suicidality (where ideation, planning and attempts were collapsed into one variable) for those who had served in the ADF for less than 4 years, had been medically discharged, were registered as a client of DVA, were in the Army and were of lower rank. Furthermore, the Transitioned ADF were significantly more likely to report suicidal ideation, plans and attempts than the 2015 current serving Regular ADF. Notably, there was also an upwards trend in suicidality in the current serving in 2015 (8.8%) as compared to the current serving in 2010 (4.0%; Van Hooff et al., 2018).
Estimated prevalence of suicidality in Transitioned ADF and the entire current serving Regular ADF in 2010 and 2015.
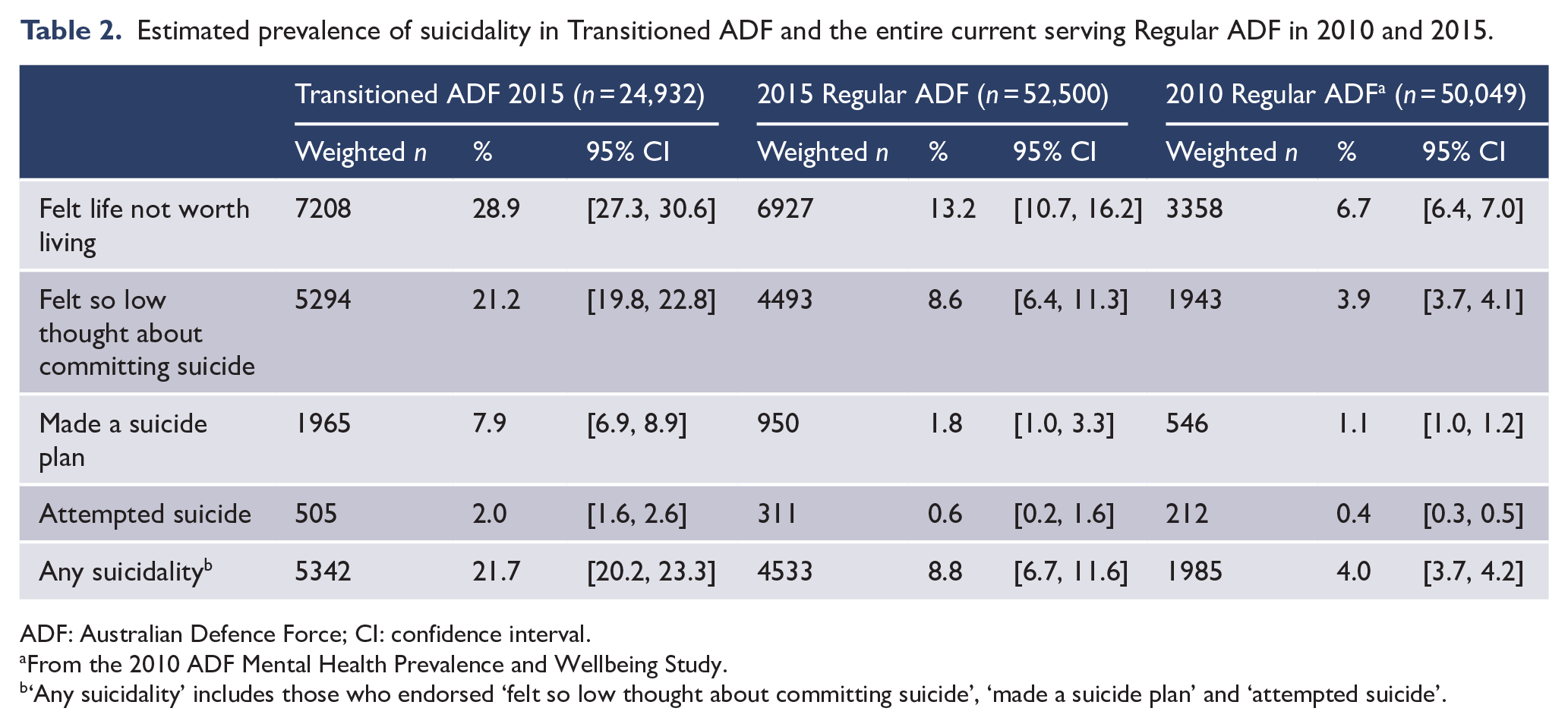
ADF: Australian Defence Force; CI: confidence interval.
From the 2010 ADF Mental Health Prevalence and Wellbeing Study.
‘Any suicidality’ includes those who endorsed ‘felt so low thought about committing suicide’, ‘made a suicide plan’ and ‘attempted suicide’.
Time elapsed since transition was also reported to be a determinant of risk of suicidality, with any suicidality significantly increasing 1 year after transitioning. The estimated prevalence of all forms of 12 month suicidality was lowest in those who had transitioned in the past year (13.9%), compared to rates of over 20% for those who had transitioned 1, 2, 4 or 5 years prior. The highest estimated prevalence of suicidality was observed at 3 years post-transition out of full-time ADF service. Furthermore, suicidality risk increased as ‘distance’ from full-time ADF service increased. Those who had completely transitioned out of ADF service (e.g. medically discharged) were 3.2 times more likely to report any suicidality within the past year than those who had transitioned to the Active Reserves (still completing at least 20 days of military service per year) and 2.4 times more likely than those who had transitioned to the Inactive Reserves (not consistently providing Reserve service; Van Hooff et al., 2018).
Additional analysis examined the relationship between probable 30-day mental disorder and suicidality in the Transitioned ADF and 2015 Regular ADF. For the purpose of this analysis, and due to the fact that CIDI interviews were not conducted on a representative proportion of current serving Regular ADF members in 2015, a composite measure of 30-day probable mental disorder was derived from validated screening and epidemiological scores (Searle et al., 2015) on the Kessler Psychological Distress 10-item scale (K10; Kessler et al., 2002) and the Posttraumatic Stress Disorder Checklist – civilian version (PCL-C; Weathers et al., 1994). Based on these validated cut-offs on the K10 and PCL-C, three groups were defined: No probable 30-day disorder: below screening cut-off on K10 (17) and PCL-C (29); 30-day Subsyndromal probable disorder: above the optimal screening cut-off on either the K10 (17) or PCL-C (29), but below the optimal epidemiological cut-off on both the K10 (25) and PCL-C (53); Probable 30-day disorder: above the epidemiological cut-off on either the K10 (25) or PCL-C (53) (Van Hooff et al., 2018).
As illustrated in Table 3, as the severity of self-reported mental health issues increased, so did the proportion of individuals reporting suicidality in the previous 12 months. While the majority of people reporting 12-month suicidality also reported a probable 30-day disorder at the time of data collection, it is important to note there is a small proportion of both transitioned and current serving members who were reporting no probable 30-day disorder or subsyndromal probable disorder at the time of data collection, but who had indicated 12-month suicidality. This highlights that individuals without a probable mental disorder can also be at risk of suicidality.
Probable 30-day mental disorder and 12-month any suicidality in the Transitioned ADF and 2015 Regular ADF.
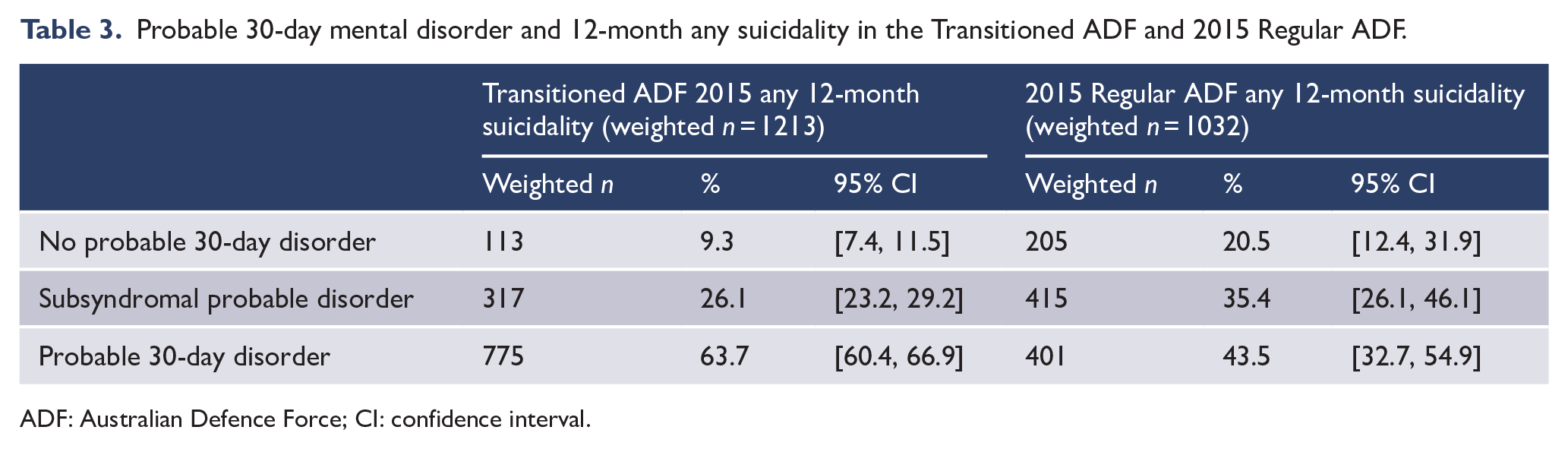
ADF: Australian Defence Force; CI: confidence interval.
The Mental Health Changes Over Time Report (Bryant et al., 2019) linked self-report data from the 2010 ADF Mental Health Prevalence and Wellbeing Study and the 2015 Transition and Wellbeing Research Programme to examine changes in mental disorder (defined as either ICD-10 affective, alcohol or anxiety disorders) and self-reported mental health symptoms over a five-year period (2010-2015). This was referred to as the longitudinal cohort, and the data were not weighted. Overall, the rates of mental disorder were higher in both 2010 and 2015 in those members of the longitudinal cohort who had transitioned by 2015, compared to those who remained in the Regular ADF in 2015 (2010: 48.3% vs 39.0%; 2015: 51.7% vs 43.3%). The most common mental disorder experienced by both groups were anxiety disorders, and this was the only disorder category that showed a significant change over the 5-year period between 2010 (32.6%) and 2015 (37.8%).
In relation to self-reported suicidality in the longitudinal cohort (Table 4), the most frequently endorsed suicide item was that they ‘felt that their life was not worth living’, with the percentage of respondents endorsing the item almost doubling between 2010 (8.2%) and 2015 (15.8%). There was a greater increase in those who had transitioned out of full-time ADF service in comparison to those who had remained in full-time ADF service at both time points (in 2010, 11.3% for the transitioned cohort versus 7.0% for the 2015 Regular ADF cohort; in 2015, 26.2% for the transitioned cohort versus 11.9% for the 2015 Regular ADF cohort). The second most highly endorsed item was also related to ideation, ‘have you felt so low you have thought about committing suicide’, with 4.7% endorsing this item in 2010 and 10.6% endorsing it in 2015. There was a higher increase in those who had transitioned than those who had remained in full-time service (2010: 6.9% vs 3.9%, 2015: 18.6% vs 7.6%).
Suicidal ideation, plans and attempts in Transitioned ADF and 2015 Regular ADF in the longitudinal cohort.
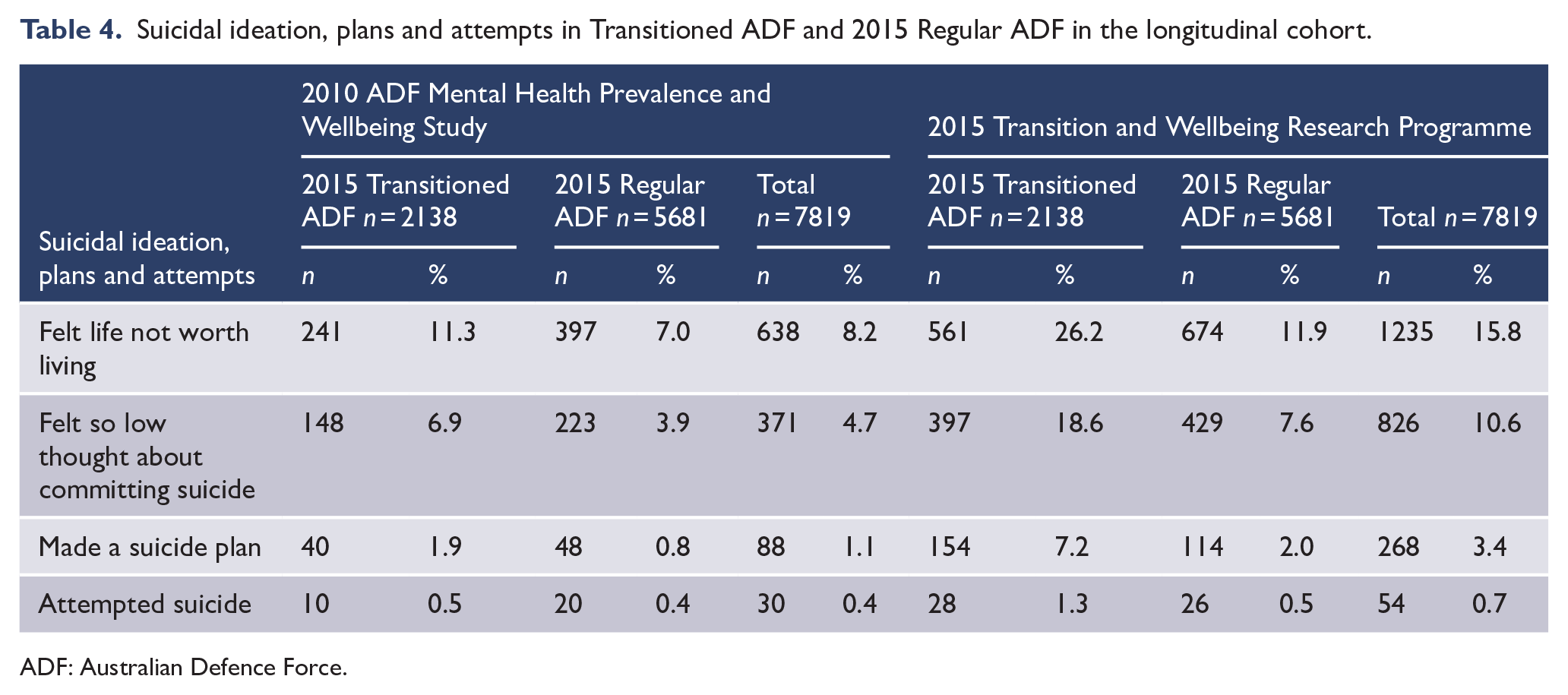
ADF: Australian Defence Force.
Although a substantially smaller number endorsed the item relating to making a suicide plan (1.1% in 2010, 3.4% in 2015), the numbers endorsing these items, as well as the increase in rates between the two time points were higher in those who had transitioned (1.9% in 2010, 7.2% in 2015) in comparison to those who had remained in full-time ADF service at both time points (0.8% in 2010, 2.0% in 2015). Similarly, the number endorsing the suicide attempt item was small across both time points (0.4% in 2010, 0.7% in 2015), with the greatest increases reported in those who had transitioned (0.5% in 2010, 1.3% in 2015) compared to those who had remained in full-time service across both time points (0.4% in 2010, 0.5% in 2015).
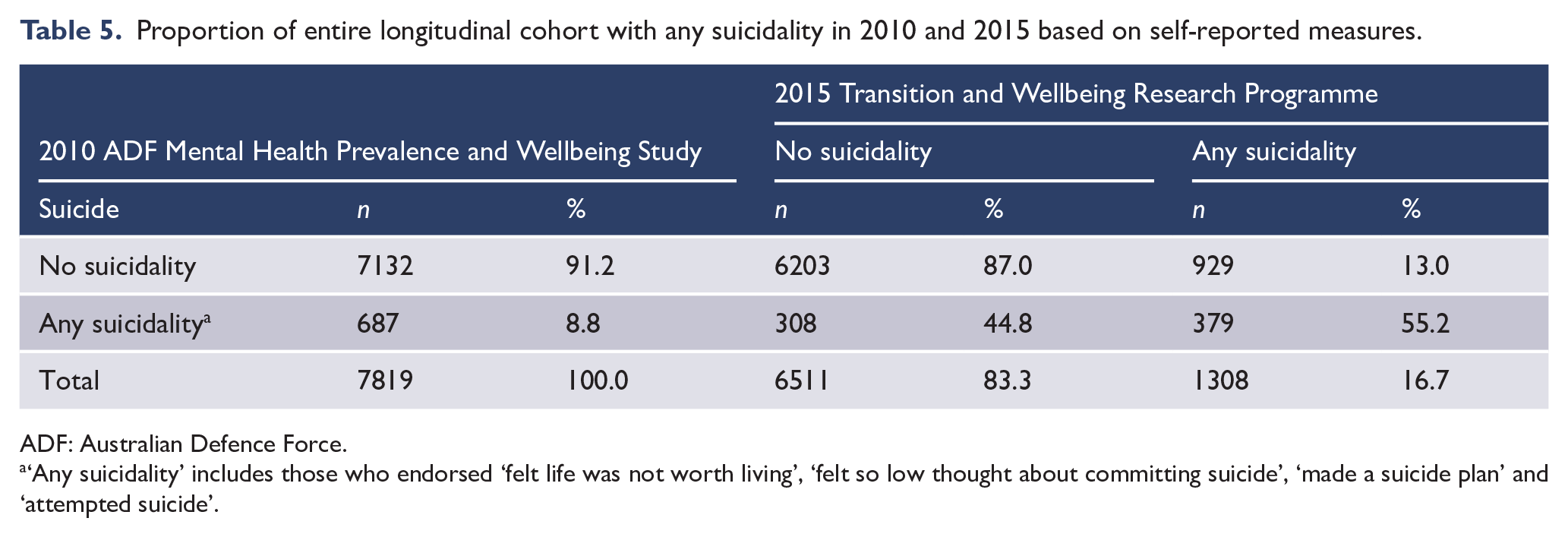
The report also analysed the proportion of those endorsing any suicidality item in 2010 cross-tabulated by the same grouping of scores in 2015, among the entire longitudinal cohort, and according to whether they had transitioned or remained in full-time ADF service in 2015. In the longitudinal cohort, 8.8% reported any suicidality in 2010 and this increased to 16.7% in 2015 (Table 5). Of those who had reported no suicidality in 2010, 13.0% were new cases of suicidality in 2015, and of those who had reported any suicidality in 2010, over half of them (55.2%) still endorsed at least one suicidality item in 2015.
Proportion of entire longitudinal cohort with any suicidality in 2010 and 2015 based on self-reported measures.
ADF: Australian Defence Force.
‘Any suicidality’ includes those who endorsed ‘felt life was not worth living’, ‘felt so low thought about committing suicide’, ‘made a suicide plan’ and ‘attempted suicide’.
Among those members of the longitudinal cohort who had transitioned out of full-time ADF service between 2010 and 2014 (n = 2138), the rates reporting any suicidality doubled between 2010 (12.3%, n = 263) and 2015 (27.4%, n = 586). Of this group (Figure 1), 78.3% (n = 1468) did not report any suicidality in 2010 or in 2015, but 21.7% (n = 407) reported suicidality in 2015, who did not in 2010. Of those who had reported any suicidality in 2010, 68.1% (n = 179) still reported any suicidality in 2015 and 31.9% (n = 84) no longer reported suicidality.
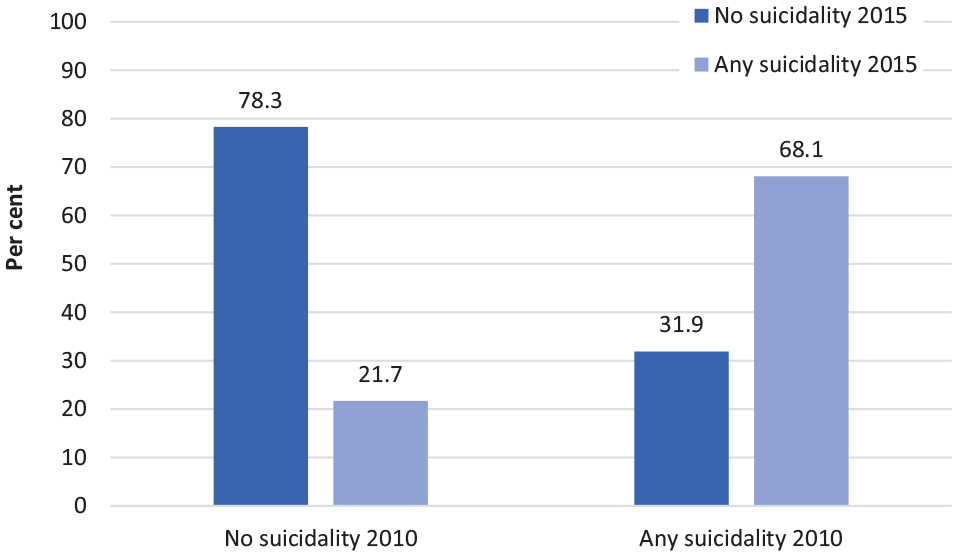
Proportion of Transitioned ADF in the longitudinal cohort with any suicidality in 2010 and 2015 based on self-reported measures.
Among those members of the longitudinal cohort who remained in the full-time ADF at both time points (in 2010 and 2015, n = 5681), 7.5% (n = 424) reported suicidality in 2010 and 12.7% (n = 722) in 2015. Of this group (Figure 2), among those reporting no suicidality in 2010 (92.5%, n = 5257), the majority (90.1%, n = 4735) still did not report suicidality in 2015. Of those who did endorse at least one suicide item in 2010 (7.5%, n = 424), almost half (47.2%, n = 200) also reported suicidality in 2015.
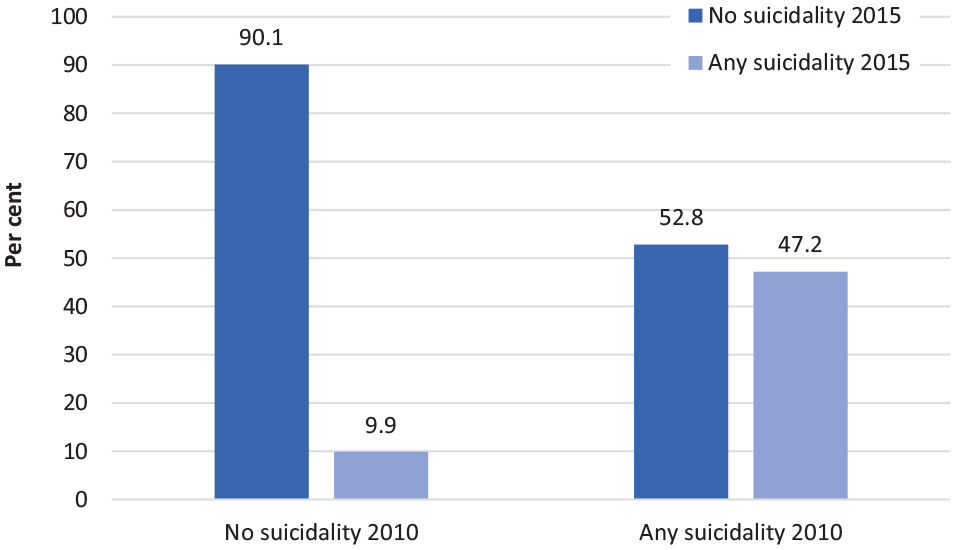
Proportion of 2015 Regular ADF in the longitudinal cohort with any suicidality in 2010 and 2015 based on self-reported measures.
Proportionally more new cases of suicidality (no suicidality in 2010, but at least one suicidality item endorsed in 2015) were reported in those who had transitioned compared to those still serving (21.7% vs 9.9%). Of those who had reported any suicidality in 2010, a greater proportion of the transitioned group (68.1%) again reported any suicidality in 2015 compared to those still serving (47.2%). Therefore, one in four of the transitioned cohort reported any suicidality in 2015, and almost one-third of this group had reported any suicidality in 2010.
Reported 12-month any suicidality in 2010 also predicted a shift from no disorder (defined as below screening cut-off on the K-10 and the PCL-C in 2010) to 30-day probable mental disorder (above the epidemiological cut-off on either the K-10 or PCL-C) in 2015. Those reporting 12-month any suicidality in 2010 were more likely to shift from having no disorder in 2010 to current probable disorder in 2015, compared to those who did not report any suicidality (OR = 3.11; 95% CI = [1.65, 5.86]). The findings from the longitudinal cohort highlight how suicidality can develop over time, including in those who have previously reported no suicidality, with a more pronounced increase in new cases in those who had transitioned out of full-time ADF service. Notably, in those who had previously reported any suicidality, approximately half continued to report suicidality years later, and they also had an increased risk of reporting a current probable mental disorder. This has important implications for early intervention.
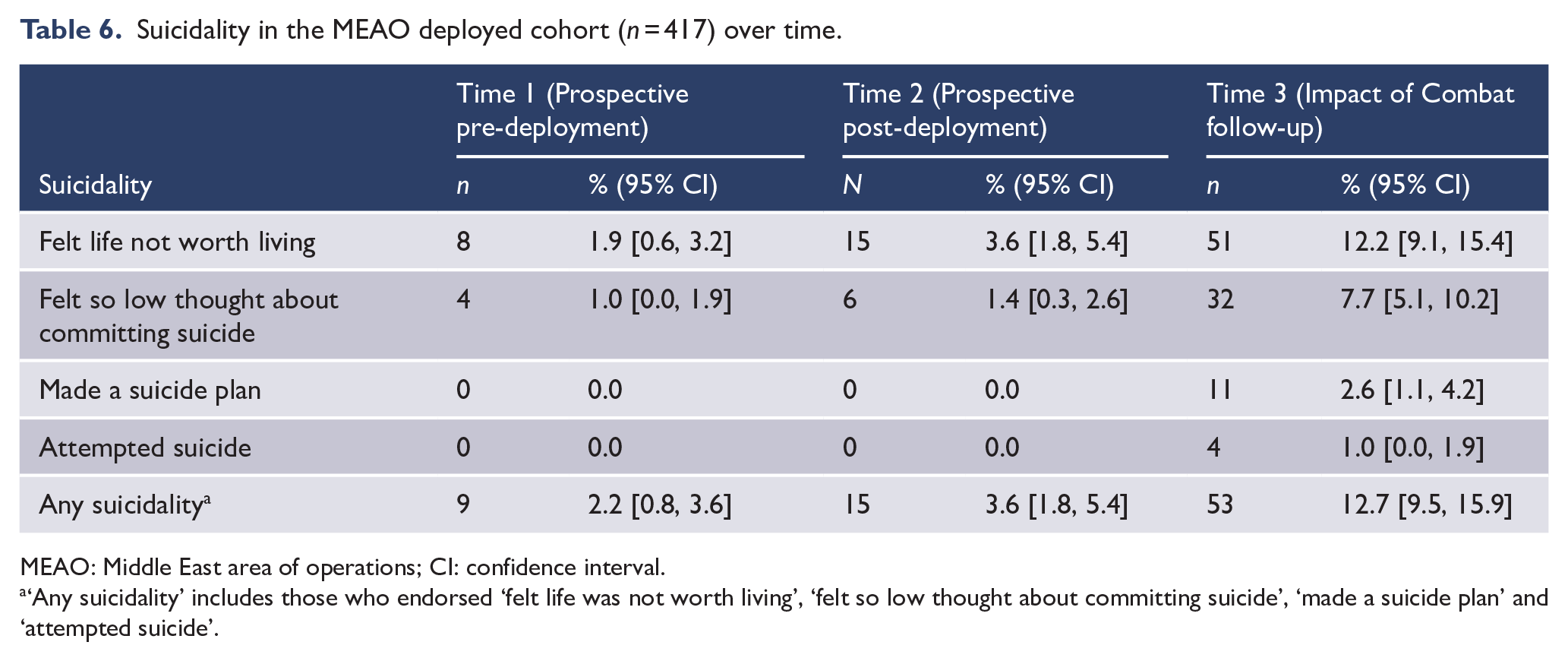
The Impact of Combat Study (Lawrence-Wood et al., 2019) documented changes over time in the mental, physical and neurocognitive health and wellbeing of a healthy, deploying cohort of ADF members (MEAO deployed cohort). This small but significant cohort (129 Transitioned ADF, 431 Regular ADF) participated in the MEAO Prospective Health Study and had deployed to the MEAO between 2010 and 2012, completing both a pre-deployment survey (Time 1) and a survey approximately 4 months post-deployment (Time 2). The Transition and Wellbeing Research Programme represented the third wave of data collection (Time 3). Although the majority of the cohort remained well, rates of psychological and physical symptoms and disorder increased over time, particularly in those who had transitioned from full-time ADF service. The proportion of the entire deployed cohort who reported any suicidality (Table 6) only increased slightly from Time 1 (2.2%) to Time 2 (3.6%), but it increased dramatically at Time 3 (12.7%). At Time 1 and Time 2, no members of the cohort reported having made a suicide plan or attempt; however, by Time 3, 2.6% of the cohort reported having made a plan and 1.0% had made a suicide attempt.
Suicidality in the MEAO deployed cohort (n = 417) over time.
MEAO: Middle East area of operations; CI: confidence interval.
‘Any suicidality’ includes those who endorsed ‘felt life was not worth living’, ‘felt so low thought about committing suicide’, ‘made a suicide plan’ and ‘attempted suicide’.
Summary of findings and implications
The research on contemporary ADF personnel highlights that for many there are protective factors associated with military service, with lower rates of suicide attempts and completed suicides in both the full-time and Reserve components than the sociodemographically matched Australian community. In part, this may reflect the rigorous ADF recruitment system, which would exclude some individuals at higher risk of suicidality. However, there are still areas of concern relating to completed suicides and suicidality in the serving ADF population, and these intensify following transition from full-time ADF service.
The detailed analysis undertaken on completed suicides has established that the suicide risk for males in the full-time and Reserve components of the ADF is significantly less than the aged-match Australian community. The rate of completed suicides in ex-serving ADF males, however, is more than double the rate for serving ADF males. The rate of completed suicides in ex-serving ADF men is higher than Australian men of the same age, and this rate is significantly higher in ex-serving ADF men aged below 30 years. Due to the smaller population, meaningful analysis has not been possible on rates of completed suicides in current serving ADF females, but the age-adjusted rate of suicide for ex-serving ADF women is more than double the rate for Australian women.
When age and gender were controlled for, the ADF Service-related characteristics associated with completed suicides were having been medically discharged and being any rank other than a commissioned officer. Although not statistically significant, there were indications that those with less than 1 year of military service were at increased risk compared to those who had served 10 years or more. There was no significant difference in the suicide rates between those with or without operational service or between the different Service branches.
Key factors associated with completed suicides in the Australian military are consistent with the findings from other militaries, including gender, younger age and lower rank (e.g. Ministry of Defence, 2020; Ursano et al., 2017). Studies in other countries have also not identified a clear link between operational service and risk for completed suicides or suicidality, with many other military and personal factors contributing to risk (Ejdesgaard et al., 2015; Ursano et al., 2016), including psychiatric disorder (Ursano et al., 2016) and the type of combat exposures experienced during deployment (Bryan et al., 2015).
The analysis of suicidality in 2010 revealed that while the rate of suicide ideation in the current serving ADF was higher than the matched community rate, there was a lower progression to behaviours (attempts and completed suicides) than in the general community. Analysis of the data collected in 2015 has established that the risk for suicidality significantly increases in ADF personnel who have recently transitioned out of full-time military service, and consistent with the findings for completed suicides, the risk is particularly evident for younger males of lower ranks, and those who have been medically discharged. The risk increases 1-year post-transition and peaks approximately 3 years following transition out of full-time ADF service and is significantly higher for those who have completely transitioned out of any ADF involvement compared to those who remain in the Reserves (Van Hooff et al., 2018).
Furthermore, there is a trend of increasing suicidality within the serving and ex-serving ADF population over time. Self-reported rates increased across the domains of ideation, plans and attempts between 2010 and 2015 in those still serving in the ADF, but particularly increased in those who had transitioned out of full-time ADF service by 2015. Interestingly, this trend of increasing risk over time was also found in a healthy, deploying cohort, again particularly once they had transitioned out of full-time ADF service. The levels of suicide ideation reported in the serving and ex-serving populations is notable, with ideation being a major predictor of completed suicides (Cavanagh et al., 2003), and suicidal ideation while still serving was identified as an important precursor to suicidality following transition. Over two-thirds of those who had reported suicidality while serving in the ADF still reported suicidality following discharge. It is possible that these increasing suicidality rates over time in the serving and ex-serving population are mirrored in a rise in general community rates. However, this is unclear as the most recent comparable Australian data on suicide ideation, plans and attempts were collected in 2007 (ABS, 2008).
Arguably, the most studied (O’Connor and Nock, 2014) and strongest established risk factor for completed suicides and suicidality is the presence of a mental disorder (Joiner et al., 2005), and this is consistent across genders and age groups (Cavanagh et al., 2003), as well as military populations (Nock et al., 2014). Analysis of the ADF data collected in 2010 revealed a link between 12-month mental disorder and suicidal thoughts, plans and attempts, and this risk increased if there were co-morbid mental conditions, particularly in those also reporting a lifetime history of interpersonal trauma.
The analysis of the data collected in 2015 similarly indicated that as the severity of self-reported mental health symptoms increased, so did the level of risk for suicidality in both the current serving and transitioned ADF populations. Of critical importance, the longitudinal analysis revealed that self-reported suicidality also appears to be a predictor of self-reported current probable mental disorder following transition. This highlights an opportunity to not only identify suicidality in those who present for assistance with mental disorders but to also target suicidal ideation as a way of identifying those who may require additional assistance and support to reduce the risk of broader mental health issues (Bryant et al., 2019). A recent Australian study which analysed the 2015 data revealed that 12-month suicidality was associated with childhood anxiety and childhood interpersonal trauma (Sheriff et al., 2019), highlighting the need to take a whole of life approach to understanding suicidality in military populations.
Despite the strong association between mental disorder and suicidality, the majority of individuals with a mental disorder do not report suicidal thoughts, plans or attempts, and conversely, individuals without a mental disorder can be at risk of suicide or suicidality (O’Connor and Nock, 2014). In the ADF serving and transitioned populations, there was a small but significant group who reported any suicidality in the past 12 months without any probable 30-day mental disorder. A recent US study (Ursano et al., 2018) similarly reported that more than one-third of soldiers with a documented suicide attempt did not have a previous mental health diagnosis, highlighting that suicide assessment and early intervention opportunities for military populations should extend beyond primary health and mental health care systems (Reger et al., 2018; Ursano et al., 2018). For example, training staff working within legal and family support systems to be alert for indications of suicidality.
Overall, the findings suggest that while a range of programmes have been implemented by Defence and DVA over recent years to reduce suicide risk and improve mental health and wellbeing (Veteran Mental Health and Wellbeing Strategy and National Action Plan 2020-2023, Department of Veterans’ Affairs, 2020; Defence Mental Health and Wellbeing Strategy 2018-2023, Department of Defence, 2017; 2011 ADF Mental Health and Wellbeing Strategy, Department of Defence, 2011), they may not meet the needs of all sub-groups. Although the impact of the most recent Departmental initiatives to address suicide and suicidality is unclear from the available data, there are additional risk factors associated with transition which still need to be better understood and addressed, particularly for those who transition completely out of ADF service and for those who have transitioned over 12 months ago.
The findings also highlight the importance of investing in research which considers all stages of a military career, including the period of transition and beyond, regardless of the length or nature of ADF service. There are distinct differences between the serving and transitioned cohorts (including differences between those who have transitioned and are now ex-serving and those who have transitioned but are still in the Active or Inactive Reserves) and this has implications for the development of targeted prevention and early intervention programmes. For example, the findings illustrate there would be significant value in identifying those who are experiencing suicidality while still serving, as well as actively following-up individuals post-transition from full-time ADF service, including those who did not report any suicidality during their military career. The ADF research supports the need for this follow-up to continue several years following transition and to include those transitioning from both the ADF full-time and Reserve components.
The period of transition out of full-time (Shields et al., 2016; Van Hooff et al., 2018) and part-time (Wang et al., 2020) military service is increasingly being recognised as a time of significance and potential vulnerability, with increased rates of mental disorders and suicidality in comparison to those currently serving. In part this can be attributed to those who are transitioning due to medical reasons or because of emerging psychological distress (Van Hooff et al., 2019), with the currently serving representing the working well. This is commonly referred to as the ‘healthy soldier’ or ‘healthy warrior’ effect. However, there is evidence of a complex array of other potential stressors associated with the transition process including difficulties securing employment, interpersonal conflicts and legal difficulties (Morin, 2011). Other potential explanations include different cultures and values between military and civilian employment, loss of identity, loss of routine and purpose, loss of social connections, socialised masculinity and stoicism, subsequent trauma exposures and differences in health care systems (Mobbs and Bonanno, 2018; Sadler, 2019; Sadler et al., 2020; Van Hooff et al., 2019), as well as an under engagement in appropriate evidence-based care for mental disorders (Forbes et al., 2018). However, further empirical evidence research is required to identify the factors of transition that are associated with increased risk for mental health problems and suicidality, and how they may differ for those transitioning from the full-time versus Reserve components.
There are also other unanswered questions, including a clear understanding of the factors that contribute to the increased risk for completed suicides and suicidality, especially following transition. Research indicates there are complex and often interconnected factors associated with the risk of completed suicides or suicidality in serving and ex-serving military members; however, just as in the broader community, the causes of suicidal thoughts and behaviours are still not fully understood (Franklin et al., 2017). The reliance on cross-sectional data has been a common limitation in research related to suicide (Franklin et al., 2017), and the establishment of the ADF longitudinal cohort in particular has enabled additional investigation of how suicidality changes over time for this population. However, it is still not clear which factors lead to the progression from suicide ideation to a suicide attempt, noting that although ideation is an important precursor to attempts, most suicide ideators never attempt suicide (Franklin et al., 2017; O’Connor and Nock, 2014). The link between mental disorder and suicidality is one area that warrants further investigation as a risk factor, but also of interest is ascertaining the risk factors influencing the small but significant group of serving and ex-serving ADF personnel who report any suicidality over the previous 12 months without any probable 30-day mental disorder.
Finally, the limitations of the available research data must be acknowledged, particularly in relation to understanding suicidality in those who have transitioned out of full-time ADF service. While the Transition and Wellbeing Research Programme is the most comprehensive examination undertaken of the mental, physical and social health of contemporary ex-serving ADF personnel, and data were weighted to be representative of the entire transitioned and Regular ADF populations, the response rate in the transitioned cohort was less than 20% (Van Hooff et al., 2018). Findings should therefore be interpreted with caution, especially for the relatively low numbers who reported suicide plans and attempts. This includes the interpretation of probable current disorder and suicidality. As probable current disorder was self-reported over the previous 4-week period and suicidality was self-reported over the previous 12-month period, it is possible that individuals did not experience mental health symptoms and suicidality concurrently. This makes it difficult to know if suicidality is linked to a progression to disorder or relapse of disorder, or perhaps both. Furthermore, while a longitudinal cohort was established, this only included a subset of those who participated in the 2010 ADF prevalence research (McFarlane et al., 2011). A clearer understanding of how suicide risk changes over time for the serving and ex-serving ADF populations could be achieved through longitudinal surveillance of this entire 2010 cohort, along with the collection of data on a matched civilian cohort. Researchers must also investigate novel ways to improve participation in data collection, particularly following transition from full-time military service.
Conclusion
The Australian research conducted over recent years has significantly increased our understanding of the magnitude of suicidal thoughts and behaviours in contemporary serving and ex-serving ADF personnel. The findings provide insight into career phases and groups that should be followed-up and targeted for prevention and early intervention programmes, including prior to and several years following the transition out of full-time military service. Further research to better understand the factors that influence those who develop suicidal ideation and then the factors that influence progression to plans and then attempts, will inform a more sophisticated approach to suicide prevention programmes for serving and ex-serving ADF personnel. This has direct implications for training, policy development and service delivery within Defence and DVA, as well as the broader health services and other support agencies for these populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Nicole Sadler is employed by the Army Reserves, Department of Defence. The views expressed herein are those of the author and do not reflect the official position or views of the Department of Defence.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This Work has been produced with the assistance of funding provided by the Department of Veterans’ Affairs and the Department of Defence. However, the views expressed in this version of the Work do not necessarily represent the views of the Minister for Defence or the Minister for Veterans’ Affairs or the Department of Defence or the Department of Veterans’ Affairs. The Commonwealth does not give any warranty nor accept any liability in relation to the contents of this Work.