
Abstract

To the Editor
A 55-year-old right-handed, unemployed, single Caucasian male, Mr J, was referred for diagnostic assessment of a 6-year history of cognitive impairment, on a background of polysubstance use (40+ years, especially methamphetamine peaking with over $100,000 inheritance spent in a 12-month period, 40 cigarette pack years, 8–10 alcohol units/day), head injuries in adolescence, but nil other psychiatric/medical history. The only family history was of a brother with schizophrenia and substance use who died aged 52 years from a myocardial infarction. Collateral history suggested initial memory problems and complaints of paraesthesiae and numbness, at the time attributed to heavy substance use, followed by progressive decline in memory, personality change (apathetic and ‘softer’, compared to being previously angry and xenophobic) and functional impairment, despite reduced substance use after moving in with his sister 2 years prior.
Mr J appeared significantly older than 55 and apathetic. Cognitive bedside testing demonstrated reasonable attention, but significantly impaired orientation, rapid forgetting, anomia, paraphasias, apraxia and impaired Luria. Neurological examination revealed utilisation behaviour, abnormally brisk lower limb reflexes and bilateral grasp reflexes. Sensation could not be assessed reliably.
Mr J tolerated a lumbar puncture, but his confusion and agitation prevented further assessments. Figure 1 demonstrates magnetic resonance imaging (MRI) and cerebrospinal fluid (CSF) findings that were consistent with multiple sclerosis (MS), neurodegeneration, and possibly Alzheimer’s disease (AD).
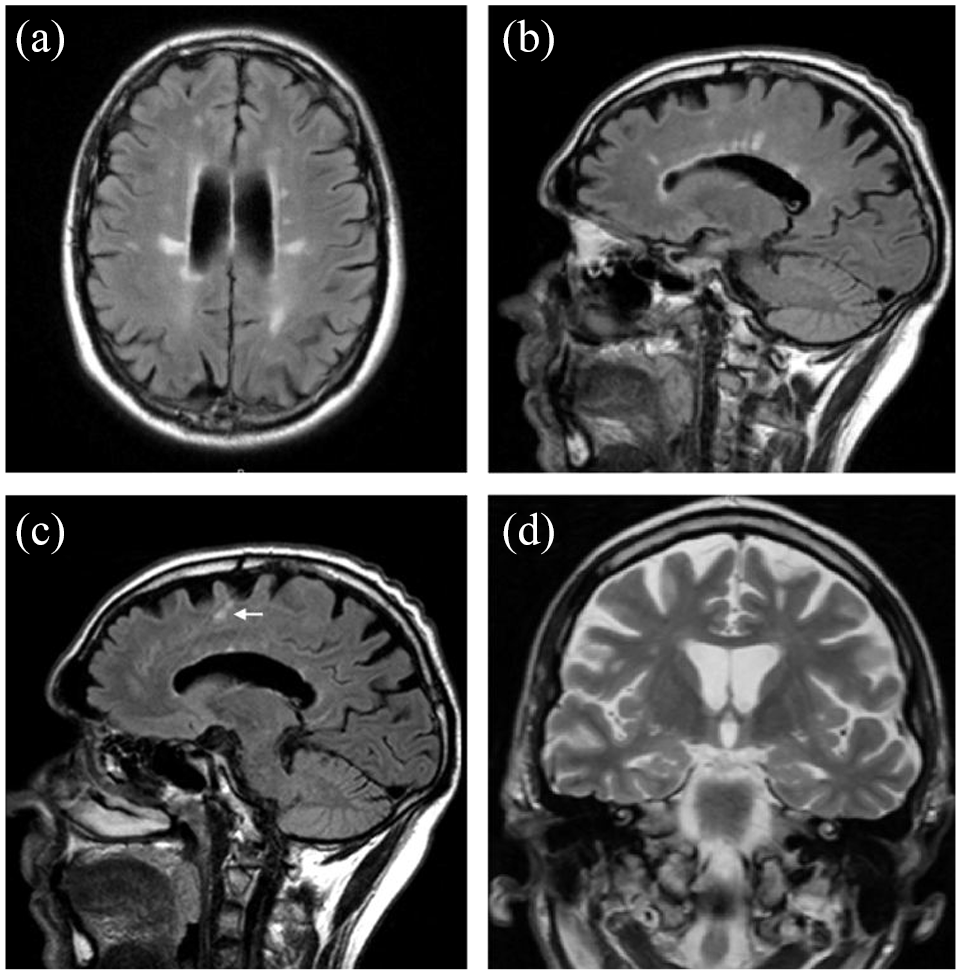
MRI brain imaging from 2 years prior and other investigation results. A and B: Excess white matter hyperintensities, some likely related to methamphetamine use but also ‘Dawson’s fingers’ pattern of periventricular white matter lesions, relatively specific to multiple sclerosis. C: Cortical lesions involving U-fibres (white arrow). Findings in A, B and C, and CSF findings (elevated CSF protein at 0.6 g/L and oligoclonal bands in CSF but not serum), suggested multiple sclerosis, fulfilling criteria for dissemination in space, although not yet for dissemination in time (there was no evidence to suggest new lesions). B and C: Dulcal widening and generalised cortical atrophy greater than expected for age. D: Bilateral hippocampal atrophy (medial temporal score 1), disproportionate to degree of generalised atrophy, along with elevated marker of neurodegeneration (neurofilament light, NfL: 805 pg/mL, normal <582 pg/mL), abnormal CSF Alzheimer’s disease proteins, low amyloid-beta 1–42: 402 pg/mL (normal >656 pg/mL), borderline total tau: 285 pg/mL (normal <304 pg/mL), borderline phosphorylated tau: 55 pg/mL (normal <59 pg/mL) and abnormal tau:amyloid-beta ratios, possibly consistent with Alzheimer’s disease pathology.
The final diagnosis was severe dementia (multifactorial aetiology: methamphetamine and alcohol use, head trauma, cerebrovascular disease, MS, possible AD). The patient was discharged home with maximised psychosocial supports, psychiatry and neurology follow-up.
To our knowledge, this is the first case of multiple pathophysiological processes related to methamphetamines, MS and AD, culminating in severe cognitive and functional decline, without prominent ‘hard’ neurological signs. Methamphetamines are associated with psychosis, anxiety, depression, memory and executive function deficits, choreoathetoid movements, increased white matter hyperintensities and demyelination (Rusyniak, 2013). Cognitive dysfunction affects 50–70% of patients with MS; dementia is present in 22%, although rare as a presenting feature, and usually occurs late in severely neurologically affected patients (Staff et al., 2015). Methamphetamine may increase the risk of AD via direct impact on hippocampi, amyloidogenic and non-amyloidogenic pathways (Shukla and Vincent, 2020).
This case highlights the utility of MRI and CSF investigations, and the challenges of diagnosing multiple neurological and neurocognitive disorders when complicated by severe substance use. Given the increasing rates of methamphetamine use, the long-term neuropsychiatric and cognitive effects of chronic methamphetamine neurotoxicity will most likely become more frequent clinical issues for clinical psychiatrists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article. The patient and family provided permission to publish this deidentified case.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.