
Abstract

To the Editor
A 28-year-old man (based on a true case – details altered to preserve confidentiality) was taken to the emergency department by his brother with suicidal ideation. He had no significant psychiatric, medical or family history and took no regular medication; there was no problematic substance use.
On psychiatric review, the patient was unable to provide a coherent account of himself or the series of events leading to his presentation. He was seemingly unable to comprehend his brother’s concerns, denied having been suicidal and repeatedly requested discharge. His history was vague, inconsistent and factually incorrect (e.g. reported being the oldest sibling of three when he is the youngest of two; said he worked ‘60+ hours in a medical practice’, when he worked part-time as a labourer; described being in a relationship with ‘Jenny’, when he had been single for 8 months). Collateral described out-of-character, disorganised behaviours the day prior. Mental state examination revealed a fatuous affect with degrees of perplexity. He was mildly thought disordered, his narrative rife with contradictions and inconsistencies. Cognitive assessment revealed a clear sensorium, but confusion, inattention and he was disoriented to time and place. His short-term recall was poor (1 from 3 words) and he was unable to complete serial-7’s. He omitted 4 months on months-of-year-backwards. A provisional diagnosis of delirium was made and recommendations for full organic workup and referral to medicine provided.
Vital signs, physical examinations, blood, urinalysis, urine drug screen (UDS), CT brain, and neurological opinion were all unremarkable. He was admitted to the psychiatric unit for further observation. Over the following 24 - 48 hours, his cognitive symptoms fully resolved. Further investigations were unremarkable (MRI-B, electroencephalogram [EEG], autoimmune-encephalitic screen). He subsequently disclosed an 8-month history of preceding psychotic symptoms including auditory hallucinations, paranoid and referential delusions, thought interference and, consequently, suicidal ideation. He was diagnosed with first-episode psychosis, responded quickly to treatment and was referred to the early intervention team before discharge home to his family.
‘Pseudodelirium’ was first coined by Goldney in 1979 to describe ‘acute functional psychoses’ that simulate delirium (Goldney and Lander, 1979). Where psychosis presents with prominent disorganisation of thought and behaviour, perplexity and/or inattention, it may be very difficult to differentiate from delirium (see Table 1). Other psychiatric syndromes that may resemble, or indeed co-occur with, delirium include ‘delirious mania’, catatonia and Ganser syndrome (Wilson et al., 2021). Efforts to delineate delirium from pseudodelirium are crucial to ensure provision of appropriate, timely clinical care and to minimise the risk of unnecessary investigations and/or iatrogenic harms (see Table 2). It nonetheless remains psychiatry’s core business to ensure that any such presentation always receives an appropriate and proportionate medical assessment prior to the provision of any definitive psychiatric diagnosis and treatment.
Potential differentiating features of delirium and ‘pseudodelirium’ (using disorganised psychosis as one such example).

Source: Adapted from Wilson (2021).
EEG: electroencephalogram.
Risks of misdiagnosis of disorganised psychosis as delirium and vice versa.
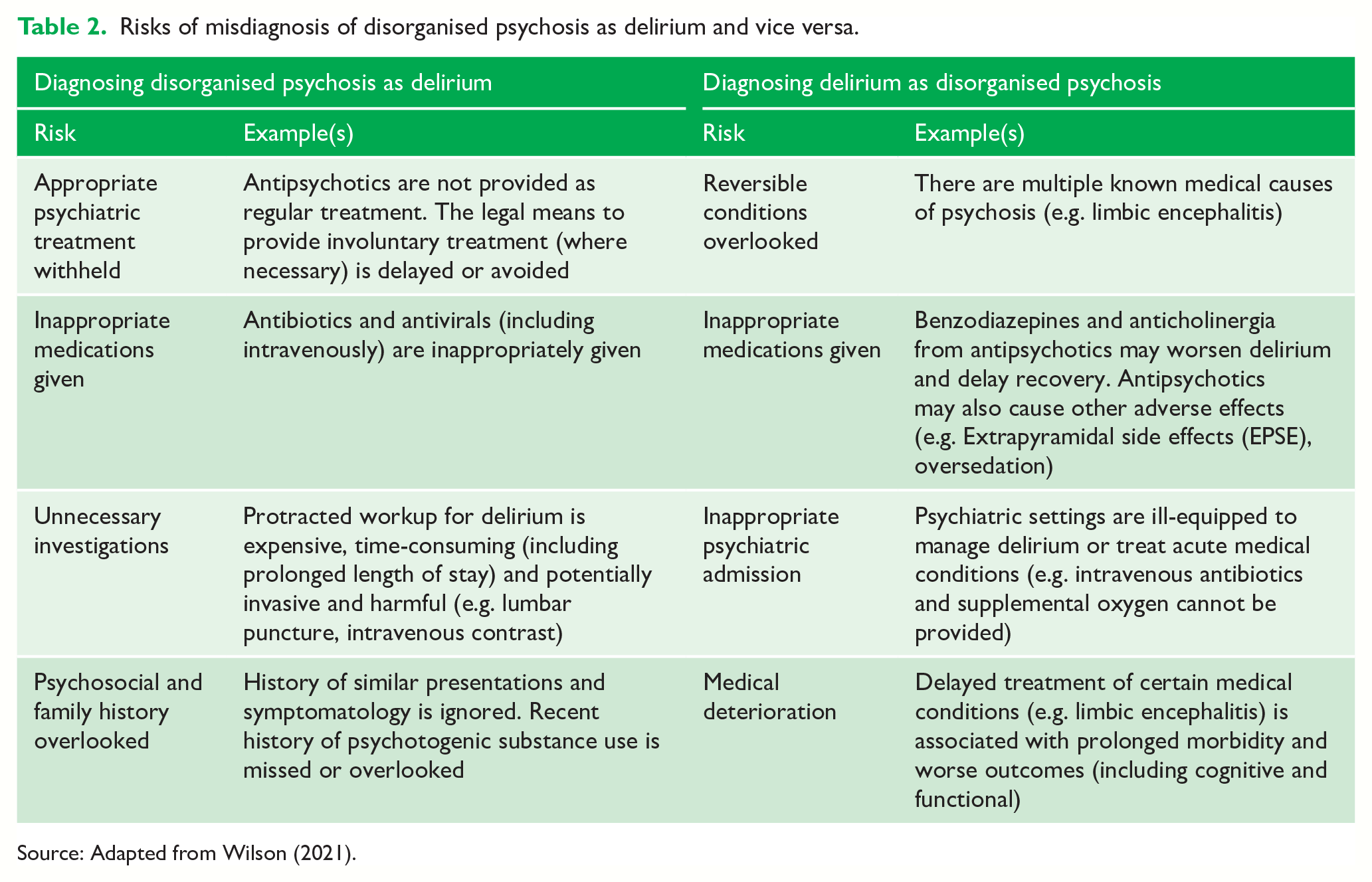
Source: Adapted from Wilson (2021).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.