
Abstract
Background:
Community reintegration from prison is typically stressful, with several health and social outcomes impacting psychiatric well-being during this time, often exacerbated among individuals with histories of drug use. Longitudinal data was used to assess change in psychiatric well-being over 2 years following release from prison among men who reported a recent history of injecting drug use.
Methods:
Data for this study come from the Prison and Transition Health cohort study of 400 men recruited in prison prior to release and followed up over three time points. Psychiatric well-being was assessed using the 12-item General Health Questionnaire. We calculated change in individual General Health Questionnaire scores between interviews and identified covariates associated with General Health Questionnaire score using linear mixed-effects regression.
Results:
Data from 690 follow-up interviews among 326 participants were included in analyses. There was considerable variation in individuals’ General Health Questionnaire scores. Moving accommodation frequently and frequent illicit drug injections were associated with an increase in General Health Questionnaire score (i.e. decline in psychiatric well-being). Two or more prior adult imprisonment episodes, social supports and past month primary healthcare attendance were associated with a decrease in General Health Questionnaire score.
Conclusion:
Our findings identify health, social and structural influences on psychiatric well-being after release from prison that can inform re-entry programmes to support community reintegration.
Keywords
Background and rationale
People with a history of illicit drug use are overrepresented in prison, with substance use disorders remaining an ongoing challenge for secure correctional settings internationally (Fazel et al., 2017). In Australia, almost two thirds of people in prison self-report using illicit substances in the 12 months before prison entry and almost half (46%) report a lifetime history of injecting drug use (Australian Institute of Health and Welfare [AIHW], 2019).
The prevalence of mental illness in prison populations globally is also elevated markedly (Baranyi et al., 2019; Fazel and Seewald, 2012), with Australian estimates ranging 40–80% of people in prison experiencing metal illness (AIHW, 2019; Butler et al., 2006). This compares to Australian general population estimates of 20% of people experiencing mental illness (AIHW, 2021). In addition, the link between substance use and poor mental health in this setting is well documented (Butler et al., 2011; Young et al., 2018), with the prevalence of co-occurring mental illness and substance use among people in prison ranging from 18% to 29% (Butler et al., 2011; Lukasiewicz et al., 2009). The high prevalence of mental health morbidity among people in prison typically occurs in the context of poor general health and social disadvantage (Aldridge et al., 2018; Degenhardt et al., 2016) and is also reflected in increased rates of self-harm (Stewart et al., 2018), with an Australian study reporting 1 in 15 people released from prison presented to hospital emergency departments for self-harm during a median follow-up period of 2½ years (Borschmann et al., 2017).
Community reintegration from prison is typically stressful, with several health and social outcomes impacting psychiatric well-being during this time. Such health and social outcomes vary between individuals and can change over time depending on peoples’ circumstances, and currently little is known about the factors and events that contribute to psychiatric well-being after release from prison among people with histories of drug use. Previous research into the psychiatric well-being of people with a history of imprisonment is cross-sectional and unable to analyse trends over time or identify factors associated with changes in psychiatric well-being (Cossar et al., 2018). Studies that have prospectively followed people after release from prison have typically recruited people from general prison populations with relatively short periods of follow-up (Thomas et al., 2016), further limiting the ability to measure key events that may trigger changes in well-being and the ability to identify possible points of intervention.
Understanding psychiatric well-being following release from prison and the factors that contribute to changes in psychiatric well-being is imperative to inform effective pre-release supports, better models of transitional care for successful community reintegration, improve health and social outcomes, and prevent reimprisonment. In this study, we used data from a cohort of men who reported a recent history of injecting drug use to assess change in self-reported psychiatric well-being over 2 years following release from prison and identify covariates associated with psychiatric well-being.
Methods
Study design and setting
Data come from baseline and follow-up behavioural surveys from the Prison and Transition Health (PATH) Cohort Study, a prospective cohort study of 400 men recruited in the weeks preceding release from one minimum, one medium and one maximum security prison in the state of Victoria, Australia (referred as participants ‘index’ imprisonment). The median index sentence length was 207 days (interquartile range [IQR] = 110–369). The PATH study protocol and participants’ characteristics have been published previously (Kirwan et al., 2019). In brief, study eligibility involved self-reporting approximately monthly injecting drug use in the 6 months prior to their index imprisonment, being aged at least 18 years at baseline, being sentenced (i.e. not on remand and awaiting trial or sentencing) and willing to consent to participate in the baseline and up to three interviews following release from prison. Participants were also asked to provide informed consent to data linkage with administrative databases. Recruitment occurred between September 2014 and May 2016, with baseline interviews occurring a median of 39 days (IQR = 15–69) prior to release. Post-release follow-up interviews were scheduled for 3, 12 and 24 months post-release. Follow-up interviews were completed in the community, or in prison for participants reimprisoned at the time a follow-up interview was due. At each interview, participants reviewed and updated detailed contact tracing information collected during baseline interview, including primary residential addresses and phone numbers. The same information was detailed for a secondary contact, such as a family member or friend, who may be contacted in the event of participants’ primary contact information changing. Additionally, the names of participants who were unable to be located via primary or secondary contacts or participants who were reported by a secondary contact as potentially being reimprisoned were provided to the Department of Justice and Community Safety (DJCS). Researchers were notified if any of these participants were reimprisoned in Victorian prisons and follow-up interviews were scheduled. Final follow-up interviews were completed in February 2019 and data linkage to administrative health and criminal justice datasets occurred following release from index imprisonment.
Ethics approval for the PATH study was granted by the Alfred Hospital Ethics Committee (79/12) and the Victorian Government DJCS Human Research Ethics Committee (CF/14/10169). All participants completed informed written consent to participant in the study.
Outcome measure
We used the 12-item General Health Questionnaire (GHQ) to measure subjective psychiatric well-being. The 12-item GHQ is a validated short screening instrument used to identify current psychiatric well-being (Goldberg, 1992) and has previously been used in studies of mental health screening during pregnancy (Iheanacho et al., 2015), among people with cancer (Gao et al., 2012), and within low- and middle-income settings (Endsley et al., 2017). Participants answered questions relating to a range of symptoms experienced within the previous 4 weeks on a 4-point Likert-type scale ranging from 0 to 3, with higher scores representing poorer psychiatric well-being (Goldberg, 1992; Goldberg et al., 1997). Responses are summed to give a final GHQ score ranging from 0 to 36. The GHQ has previously been validated for use in community-based (Donath, 2001) and low-resource settings (Endsley et al., 2017).
Covariates
Fixed and time-varying covariates were included based on previous studies of criminal justice-involved populations (Cossar et al., 2018; Stewart et al., 2018) and people who inject drugs (Scott et al., 2016, 2017) and taken from primary and administrative data across the domains of socio-demographics, social supports, physical and mental health, substance use, alcohol and other drugs (AODs) treatment and criminal justice involvement. We included imprisonment at the time of follow-up as a time-varying covariate to assess if reimprisonment is a risk factor for psychiatric well-being. Linked data from the Medicare Benefits Schedule (MBS), a database of primary care services subsidised by the Australian government, were used to identify primary healthcare contacts in the month prior to follow-up interview. Past month attendances were included to match the time scale of the GHQ, which is based on symptoms experienced within the previous 4 weeks.
Fixed covariates from the baseline interview included GHQ score (0–36), age (years), index prison security level (minimum, medium, maximum) and number of prior adult imprisonment episodes (0–1, 2, 3+). Time-varying covariates were concurrently measured alongside the primary outcome at each follow-up interview, and included imprisonment at the time of interview (no, yes); being in a stable relationship, including married, de facto or a regular partner (no, yes); available social supports, including family, partner, friends or children (no, yes); times moved accommodation since last interview (0, 1–2, 3+); employment status at the time of interview including being employed full-time, part-time, casual or self-employed versus unemployed (employed, unemployed); number of past-week drug injections (0, 1–6, 7–13, 14+); sharing injecting equipment, including needle and syringe, tourniquet, spoon, filter and water since last interview (no, yes); non-fatal opioid overdose since last interview (no, yes); currently receiving opioid agonist treatment (OAT; no, yes); non-pharmacological AOD treatment based on treatment start date preceding follow-up interview, determined using linked administrative data from the Victorian Alcohol and Drug Collections (a state-wide database of all Victorian government-funded AOD treatment episodes; no, yes); current self-reported physical health status measured on a five-item scale was dichotomised, poor health represents responses of poor and fair health, and good health represents responses of good, very good and excellent health (good, poor); past month MBS record of primary care contact (no, yes); arrested since last interview (no, yes); and victim of violent crime since last interview (no, yes).
Data analysis
Of the 400 men recruited into the PATH study, five died prior to their 3-month follow-up interview (date of death determined by data linkage from Australia’s National Death Index [NDI]). Of the remaining 395 men, 336 (85%) completed at least one follow-up interview, such that it was possible to compare GHQ scores between baseline and at least one follow-up interview (i.e. 59 participants were lost to follow-up after baseline interview). During a median of 24 months (IQR = 6–27 months) study observation, a further 18 participants died (identified via NDI records). Follow-up rates at each time point (i.e. participants interviewed) were as follows: 85% (n = 336/395) for first follow-up, 64% (n = 250/389) for second follow-up and 42% (162/382) for third follow-up. A complete case approach was taken for analysis; therefore, an additional 10 participants who had missing behavioural data (i.e. missing observations within covariates included in analysis) were excluded from the analysis. From the study sample, the final analysis sample was 326 participants who contributed 690 interview records.
To assess attrition bias, we compared baseline GHQ score and a range of baseline characteristics of participants retained (i.e. those who completed at least one follow-up interview and had no missing observations within covariates included in analysis) and not retained in the analysis using an independent sample t-test for continuous variables and chi-square test for categorical variables.
We described psychiatric well-being in the sample by calculating mean GHQ scores at baseline and each follow-up interview and compared these using paired-samples t-tests. To assess the prevalence of psychiatric caseness, poor psychiatric well-being was determined using a GHQ score cut-off threshold, with more than or equal to 12 regarded as experiencing current poor psychiatric well-being (Goldberg et al., 1997).
To assess the extent that individual GHQ scores vary between follow-up interviews, histograms of the change in individual GHQ scores between interviews were plotted for each transition. Participants were not required to complete immediately successive interviews, and to retain participants with missing interview wave/s, interview transitions were determined by interview number: baseline to follow-up 1, n = 336 transitions; follow-up 1 to follow-up 2, n = 288 transitions; and follow-up 2 to follow-up 3, n = 136 transitions. GHQ score difference was calculated as GHQ score minus GHQ score at the previous follow-up interview. For example, if GHQ score at baseline was 20 and GHQ score at first follow-up was 16, then the change score at first follow-up would be −4. Therefore, at a minimum, people contributed one change score (first follow-up minus baseline) and at most three change scores (first follow-up minus baseline, second follow-up minus first follow-up, third follow-up minus second follow-up).
We generated descriptive statistics for fixed and time-varying covariates included in analysis. GHQ score recorded at first, second and third follow-up interviews were included in the regression analysis. The primary outcome was GHQ score treated as a continuous variable with repeated measures across individuals (distribution of the outcome shown in Supplementary Figure 1). Bivariable and multivariable associations between GHQ score and fixed or time-varying covariates were estimated using a linear mixed-effects regression model with clustering on the subject to account for within subject correlation. Mixed-effects models allow the inclusion of fixed and time-varying exposure variables, repeated measures, unequally spaced time points within and between participants, and differing number of time points between participants (Scott et al., 2017). Time in the model is indicated by follow-up interview with a minimum of one and a maximum of three time points. Results are presented as linear regression coefficients and 95% confidence intervals (95% CIs). All covariates were retained in the final model. All analyses were conducted in Stata 15.1 for Windows (StataCorp, 2017).
Results
Analysis involved 690 follow-up interviews from 326 participants: 326 first follow-up (median = 6.0 months post-release, IQR = 4.2–9.6), 228 second follow-up (median = 15.6 months post-release, IQR = 13.7–21.5) and 136 third follow-up (median = 27.6 months post-release, IQR = 25.5–30.9).
There was no difference in mean baseline GHQ score for participants included (n = 326; mean GHQ = 12.6, SD = 6.3) and excluded from analysis (n = 74; mean GHQ = 13.2, SD = 7.0). There were no differences in the baseline characteristics of participants included and excluded from analysis with respect to educational attainment, employment status, relationship status, times moved accommodation in the past year and prior adult imprisonment history. However, participants excluded from analysis were on average older (t-test, p = 0.002) and had poorer self-reported health status (χ2, p = 0.007) (see Supplementary Table 1).
Days since baseline interview, mean GHQ score at each interview and prevalence of poor psychiatric well-being among PATH participants, Victoria, Australia (N = 326 participants).
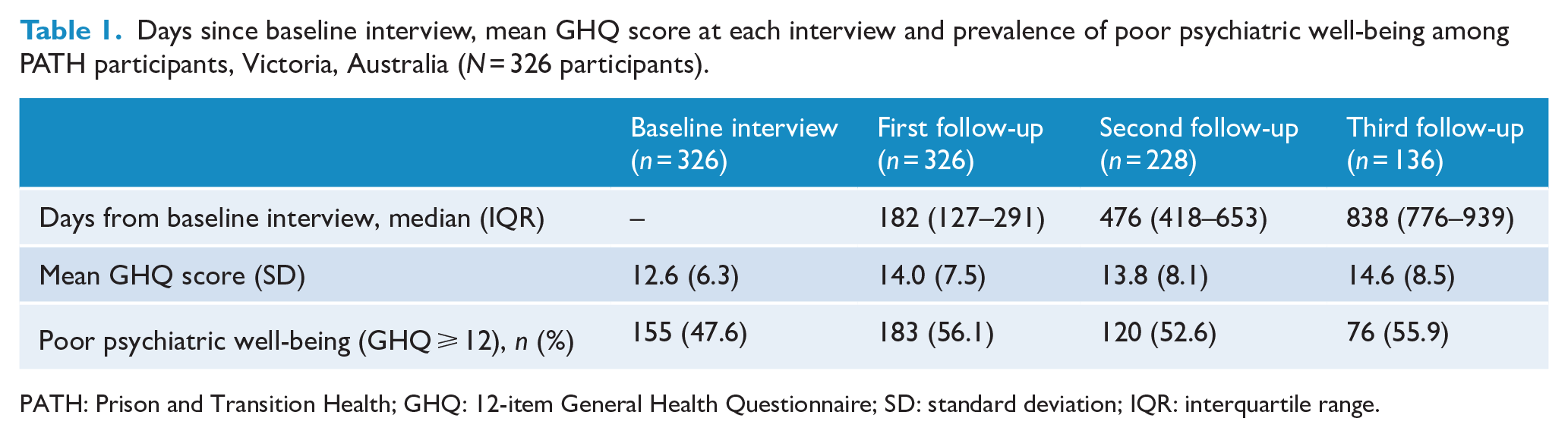
PATH: Prison and Transition Health; GHQ: 12-item General Health Questionnaire; SD: standard deviation; IQR: interquartile range.
At baseline, the mean age of participants was 35 years (SD = 8.15), 41% (n = 133/326) had completed less than 10 years of education, 83% (n = 270/326) were unemployed prior to imprisonment, 64% (n = 208/326) were not in a stable relationship and the median number of prior imprisonment episodes was 5 (IQR = 3–9), with 75% (n = 245/326) of participants reporting three or more prior imprisonment episodes at baseline interview. Mean GHQ score at baseline (mean GHQ = 12.6; SD = 6.3) was lower than mean GHQ score at first (mean GHQ = 14.0, SD = 7.5; t-test, p = 0.010), second (mean GHQ = 13.8, SD = 8.1, p = 0.05) and third (mean GHQ = 14.6, SD = 8.5; t-test, p = 0.005) follow-up interviews, only reaching statistical significance at first and third follow-up. This reflects poorer psychiatric well-being recorded during follow-up interviews compared to baseline interview. There were no statistically significant differences in mean GHQ scores between follow-up interviews (Table 1). At baseline, 48% (n = 155) of participants met the criteria for poor psychiatric well-being (i.e. GHQ score ⩾ 12), which increased to more than 50% of participants at each follow-up interview (first follow-up, n = 183, 56%; second follow-up, n = 120, 53%; third follow-up, n = 76, 56%).
Change in GHQ scores across interview waves
While the mean GHQ scores were relatively stable, there was considerable variation in individuals’ GHQ scores over time (Figure 1). Figure 1 displays a normal distribution of change in GHQ score (ranges of change, transition 1, −26 to 27; transition 2, −29 to 26; transition 3, −21 to 26; distribution with single unit on x-axis is shown in Supplementary Figure 2). Thirty-eight per cent, 29% and 10% of the sample recorded a change in GHQ score that was between 5 and 10 points of their previous score, while 21%, 29% and 28% of the sample recorded a change in GHQ score that varied by 10 or more points from their previous interview at transition 1, 2 and 3, respectively.
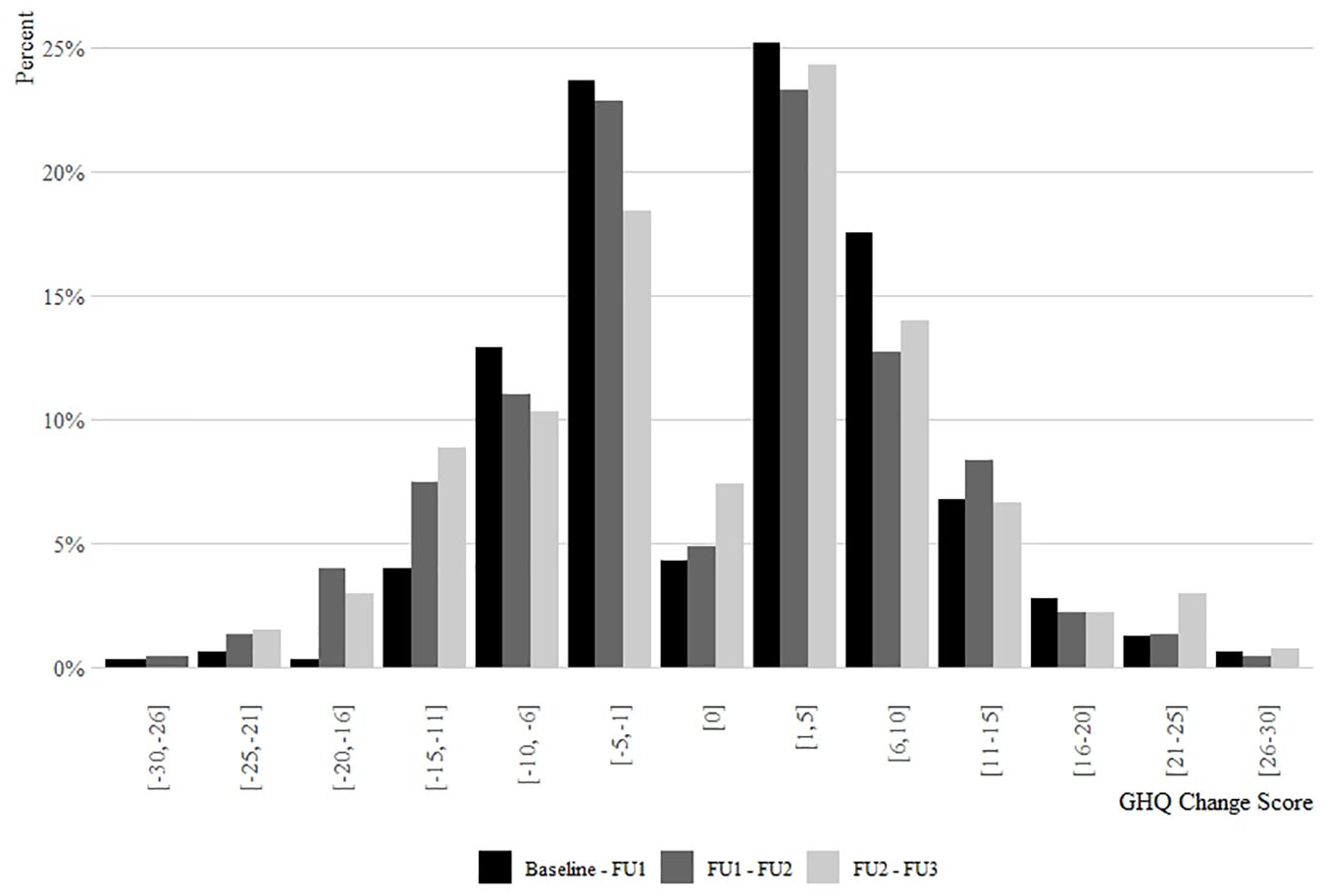
Change in individual GHQ scores among PATH participants. The distribution displays the difference recorded between interview transitions from baseline to third follow-up interview (transitions include: baseline to follow-up 1, n =326; follow-up 1 to follow-up 2, n = 228; follow-up 2 to follow-up 3, n = 136).
Mixed-effects regression model
Table 2 shows associations between covariates and GHQ score from the mixed-effects regression model. After adjustment for covariates, variables associated with an increase in GHQ score included a higher baseline GHQ score (adj. coef. = 0.28, 95% CI = [0.2, 0.37]), moving accommodation more than three times since last interview (adj. coef. = 1.48, 95% CI = [0.2, 2.77]), reporting seven or more illicit drug injections in the past week (7–13 injections, adj. coef. = 3.39, 95% CI = [1.46, 5.31]; 14+ injections, adj. coef. = 3.47, 95% CI = [2.07, 4.86]), and self-reporting poor health status (adj. coef. = 5.78, 95% CI = [4.65, 6.9]). Variables associated with a decrease in GHQ score were reporting two (adj. coef. = −2.82, 95% CI = [−5.11, −0.53]) or three or more (adj. coef. = −3.07, 95% CI = [−5.09, −1.04]) prior adult imprisonment episodes at baseline interview, having available social supports (adj. coef. = −2.54, 95% CI = [−3.79, −1.29]), and a primary healthcare contact in the past month (adj. coef. = −1.43, 95% CI = [−2.63, −0.23]; Table 2).
Participant characteristics, bivariate and multivariable linear mixed-effects regression results (N = 690 records, 326 participants).
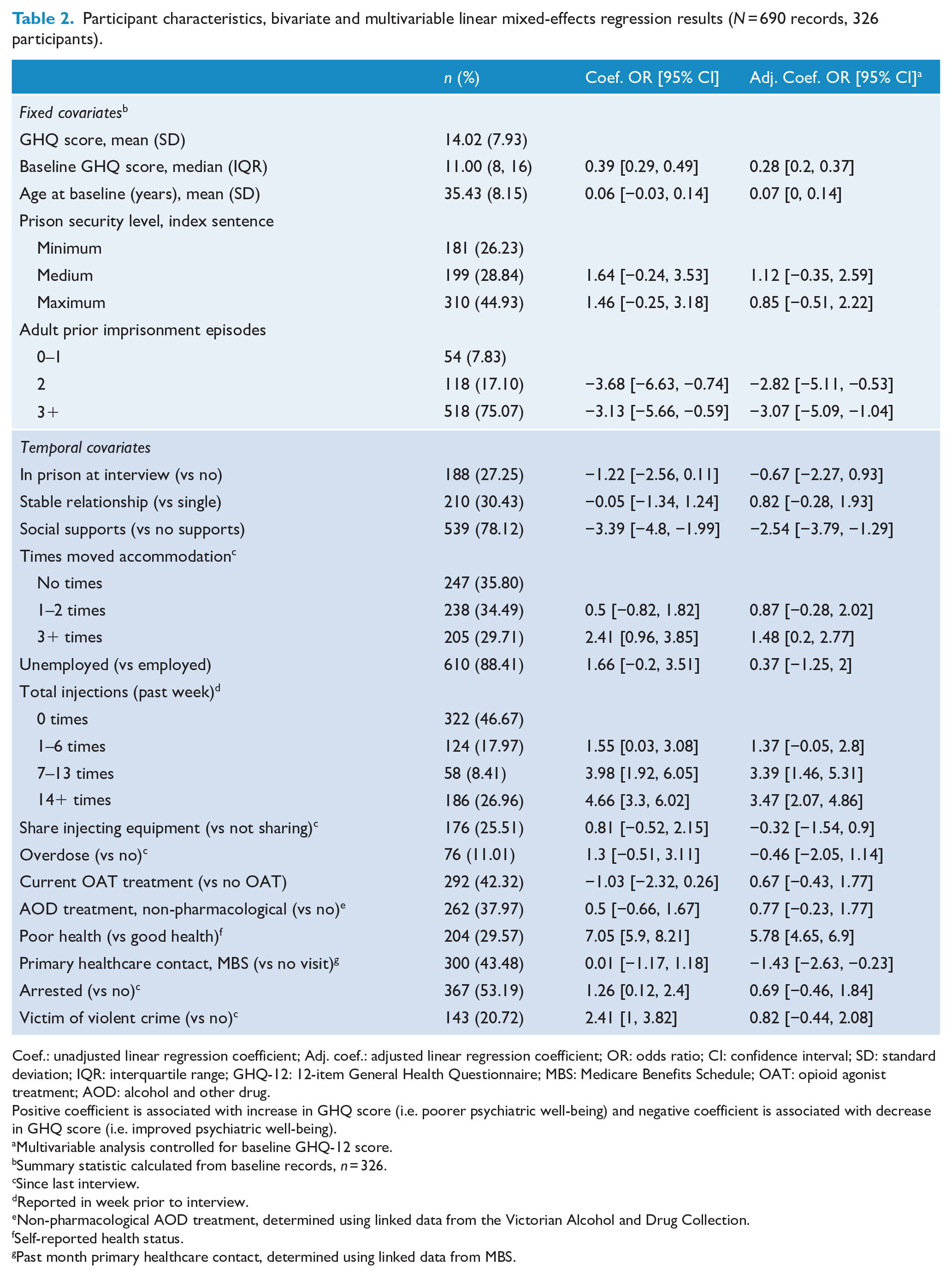
Coef.: unadjusted linear regression coefficient; Adj. coef.: adjusted linear regression coefficient; OR: odds ratio; CI: confidence interval; SD: standard deviation; IQR: interquartile range; GHQ-12: 12-item General Health Questionnaire; MBS: Medicare Benefits Schedule; OAT: opioid agonist treatment; AOD: alcohol and other drug.
Positive coefficient is associated with increase in GHQ score (i.e. poorer psychiatric well-being) and negative coefficient is associated with decrease in GHQ score (i.e. improved psychiatric well-being).
Multivariable analysis controlled for baseline GHQ-12 score.
Summary statistic calculated from baseline records, n = 326.
Since last interview.
Reported in week prior to interview.
Non-pharmacological AOD treatment, determined using linked data from the Victorian Alcohol and Drug Collection.
Self-reported health status.
Past month primary healthcare contact, determined using linked data from MBS.
Discussion
Approximately half of the PATH study participants with histories of injecting drug use experienced poor psychiatric well-being at each interview following release from prison, and poor psychiatric well-being was more prevalent post-release than pre-release. This finding is consistent with high rates of mental health morbidity among people in prison reported in local and international contexts (Butler et al., 2011; Fazel and Seewald, 2012; Prince and Wald, 2018), and the additional challenges faced upon release for people with substance use histories, such as resumption of substance use (Winter et al., 2016). Although there was little change in the prevalence of poor psychiatric well-being across interview waves in our sample, this masked large variations in individuals’ GHQ scores. These changes were associated with prior imprisonment history, accessing healthcare, having available social supports, accommodation stability and patterns of high-frequency drug use. These findings point to potential targets for tailored interventions to address poor psychiatric well-being and prevent subsequent associated health, social and offending outcomes.
Participants who reported previous episodes of adult imprisonment reported improved psychiatric well-being in our study. First episode of imprisonment is associated with higher levels of stress related to uncertainties associated with expectations of both time in prison and community transition (Souza and Dhami, 2010). Following release from prison, people often face several challenges, such as reconnecting with family and friends, seeking employment (Wildeman and Muller, 2012), accessing stable housing (Baldry et al., 2016) and addressing healthcare needs (Young et al., 2015). Repeated episodes of imprisonment may result in people becoming better at navigating the prison system and the immediate period following release from prison, or at least be able to anticipate challenges they experienced in the past. Our findings highlight a need for greater levels of support embedded within reintegration programmes for people completing their first period of imprisonment. Such programmes require continuity of care and in-reach programmes that link people in prison with community health and social services. The benefits of post-release engagement with health services have been demonstrated previously; early primary healthcare contact has been shown to improve health-seeking behaviours and facilitate health system navigation (Young et al., 2015). Similarly, in our study, past month engagement with primary healthcare was associated with improved psychiatric well-being. This reinforces the importance of targeted post-release supports to enable better access to healthcare, particularly following the first period of imprisonment. Special consideration should be given to mental health service contact in the community, which has been shown to reduce reoffending (Adily et al., 2020).
In our study, changing accommodation three or more times since the last interview was associated with poorer psychiatric well-being. This is consistent with previous research (Singh et al., 2019; Western et al., 2015) and underscores the importance of post-release accommodation support, particularly given the association between homelessness and experiencing physical health morbidity and reimprisonment (Aldridge et al., 2018; Baldry et al., 2016). Access to safe and stable housing is necessary for successful reintegration into the community and is crucial in fulfilling parole requirements and the capacity to seek employment (Walker et al., 2014). Short periods of imprisonment can result in displacement from housing. In 2018–2019 in Australia, the median sentence length in prison for all offences was 8 months (Australian Bureau of Statistics [ABS], 2020). Illicit drug offences were also the second most common offence recorded for people in prison (ABS, 2019), which typically attract shorter prison sentences. In Victoria, existing public housing temporary absence policies (i.e. periods of time away from public housing) include a maximum period of absence of 6 months, with extensions (up to 6 months) granted only in special circumstances (Victorian State Government, 2018). This policy may result in many people being released into homelessness and partially explains the high levels of transience within our cohort. Providing greater flexibility in such policies (e.g. lengthening of temporary absences and funding to assist in sustaining tenancies while absent) may aid in preventing release into homelessness. Additionally, consideration of non-custodial sentences for minor non-violent offences would facilitate greater stability for this population and may mitigate against a deterioration of psychiatric well-being.
The availability of social supports was associated with improved psychiatric well-being in this study; this is consistent with previous research among general prison populations (Wallace et al., 2016). Lengthening periods of visitation with family members has been recommended previously as a method of facilitating better psychological well-being for people in prison (Wallace et al., 2016). In Victorian correctional facilities, current visitation policies specify a maximum of two people (including children) per visit (Corrections Victoria., 2020). Extending the number of visitors per visit may allow for greater maintenance of family connections during imprisonment, therefore building family connectedness for support after release from prison. Strong social support networks have also been shown to contribute to a range of other desirable health and psychosocial outcomes that were significant in our model such as housing stability and a reduction in substance use. Previous research has identified a link between the availability of social support and access to stable housing, demonstrating a reliance on families and other social supports as a source of housing after release from prison (Western et al., 2015). In addition, having social supports has been associated with lower levels of substance use and crime, which also promotes psychiatric well-being after release from prison (Boman and Mowen, 2017; Mowen and Visher, 2016).
The link between substance use and mental well-being has been well documented (Scott et al., 2016). It was also supported in our study, which showed that frequency of injecting drug use (rather than returning to injecting or not) was associated with poorer psychiatric well-being. This finding raises the question of strategies that aim to promote abstinence versus those that aim to reduce frequency of injecting. Abstinence as a programme outcome continues to be the primary objective for several major programmes in the state of Victoria, including drug courts (KPMG, 2014) and within conditions of drug treatment orders (Sentencing Advisory Council, 2019). Previous research findings illustrate the shortfalls of abstinence-based programmes, such as consumer disengagement from services (Stanhope et al., 2009) and lower success rates (Gallagher et al., 2019), while highlighting their contribution to higher rates of reimprisonment due to breaches of parole. Services and programmes working within an abstinence-based approach should consider how reduced frequency of injecting can be adopted as a goal, at least in the short term, for clients who are challenging to engage. Opiate agonist therapy promotes both cessation and reduction in substance use, with episodes of imprisonment providing opportunities to initiate and maintain people on OAT. Opiate agonist therapy has been shown to improve psychological well-being (Mitchell et al., 2015) and reduce substance use (Dong et al., 2020) and behaviours associated with increased exposure to blood-borne viral infections (Blanco and Volkow, 2019; Chandler et al., 2009).
A key strength of this study is the measurement of individual-level changes in psychiatric well-being. The extent of individual variation measured in this study highlights the importance of analysing individual-level longitudinal data to identify patterns of psychiatric morbidity and other health outcomes, in addition to patterns of change in aggregated outcomes. This study also demonstrates the responsiveness of the GHQ to change over time in concordance with significant time-varying events (Mokkink et al., 2010).
This study has some limitations. The sample does not represent all people in correctional settings, but it is one of few to focus on people who inject drugs who represent a significant proportion of people imprisoned and people at high risk of reimprisonment. Due to the primary study eligibility criteria of regular injecting drug use prior to imprisonment, it was not logistically possible to collect data on people in prison who were not eligible for the study on this basis; therefore, it is not possible to determine potential differences between people who were eligible for the study and those who were not. Change in GHQ score over time was assessed across interviews, which resulted in differing time periods for measuring changes in psychiatric well-being. We note some caution in the interpretation of results as being among those only residing in the community given a proportion of the sample were in prison at the time of their follow-up interview. However, the recall period for the GHQ related to the past 4 weeks, meaning for some participants who completed follow-up in prison, their experiences may relate to time in community. There was some error inherent in comparing variables with different timescales in the model. For example, the outcome measure is based on symptoms experienced in the previous 4 weeks, while injecting frequency and times moved accommodation relate to time periods of 1 week and since last interview, respectively. Substance use ubiquity and poly-drug use in this cohort make it difficult to isolate the roles of specific drug types; therefore, we did not assess individual drug types used. This study used self-report data and may be subject to social desirability and recall biases. This study may be subject to attrition bias, and while a range of baseline characteristics were assessed, finding differences in only age and health status (see Supplementary Table 1), other differences that were not measured in this study may exist.
Conclusion
Our study shows that people released from prison who have a history of injecting drug use often have poor psychiatric well-being, indicating a need to continue efforts to improve mental health outcomes among this population. Psychiatric well-being for individuals in the cohort changed considerably over time after release from prison. Our findings identified individual characteristics and events that influence psychiatric well-being after release from prison that can be used to target programmes and resource community reintegration programmes more effectively. Such programmes include those that facilitate access to safe and secure housing, continuity of healthcare from correctional facilities to community settings and reductions in the frequency of drug use to support successful transitions and reduce mental health–related morbidity among people after release from prison.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211048143 – Supplemental material for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis
Supplemental material, sj-docx-1-anp-10.1177_00048674211048143 for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis by Ashleigh C Stewart, Reece Cossar, Anna Lee Wilkinson, Nick Scott, Paul Dietze, Brendan Quinn, Stuart A Kinner, Campbell Aitken, Shelley Walker, Michael Curtis, Tony Butler, James R. P. Ogloff and Mark Stoové in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-jpeg-1-anp-10.1177_00048674211048143 – Supplemental material for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis
Supplemental material, sj-jpeg-1-anp-10.1177_00048674211048143 for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis by Ashleigh C Stewart, Reece Cossar, Anna Lee Wilkinson, Nick Scott, Paul Dietze, Brendan Quinn, Stuart A Kinner, Campbell Aitken, Shelley Walker, Michael Curtis, Tony Butler, James R. P. Ogloff and Mark Stoové in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-tif-1-anp-10.1177_00048674211048143 – Supplemental material for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis
Supplemental material, sj-tif-1-anp-10.1177_00048674211048143 for Psychiatric well-being among men leaving prison reporting a history of injecting drug use: A longitudinal analysis by Ashleigh C Stewart, Reece Cossar, Anna Lee Wilkinson, Nick Scott, Paul Dietze, Brendan Quinn, Stuart A Kinner, Campbell Aitken, Shelley Walker, Michael Curtis, Tony Butler, James R. P. Ogloff and Mark Stoové in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the participants involved in the PATH Study for the time and knowledge they contributed. Thanks to the Burnet Institute fieldwork team for their tireless efforts with data collection. The authors would also like to acknowledge the Victorian Department of Justice and Community Safety for the support they have provided throughout the study and since its conclusion.
Author Contributions
A.S., supported by M.S. and P.D., led the concept of the paper, including writing, editing and statistical analysis. R.C., A.L.W. and N.S. assisted with statistical analysis, code review and editing. B.Q., T.B., S.A.K., J.O., S.W. and M.C. provided editorial comments and feedback. M.S. is the chief investigator of the PATH study and provided guidance for paper development and editorial support throughout the planning and writing. All authors read and approved the final manuscript.
Data Access
There are provisions for data access, however, dependent upon relevant ethics approvals due to the sensitive nature of the study data. Persons interested in obtaining data files, including code, from the Prison and Transition Health Study should contact the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.S. has received investigator-initiated funding from Gilead Sciences, AbbVie and Bristol Myers Squibb for research unrelated to this work. P.D. has received investigator-driven funding from Gilead Sciences for work related to hepatitis C treatment and an untied educational grant from Indivior for work related to the introduction of buprenorphine/naloxone into Australia. He has also served as an unpaid member of an Advisory Board for an intranasal naloxone product. The remaining authors declare that they have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by an Australian National Health and Medical Research Council Project Grant (APP1029915). M.S. and P.D. are supported by NHMRC senior research fellowships. We gratefully acknowledge the support provided to the Burnet Institute by the Victorian Government Operational Infrastructure Support Program. R.C. and A.S. are supported by Research Training Program Stipend. M.C. is supported by an NHMRC postgraduate scholarship and Monash Addiction Research Centre PhD top-up scholarship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.