
Abstract
Objective:
Problematic Internet and smartphone use is associated with serious mental health problems. We thus investigated the effectiveness of psychological interventions on problematic Internet and smartphone use.
Methods:
We conducted a systematic review and meta-analysis and searched in PubMed, PsyArticles, PsycInfo, Medline and Google Scholar for peer-reviewed experimental and quasi-experimental research published between 2008 and 2021.
Results:
A total of 10 studies accompanied by 14 effect sizes were included in the meta-analyses for problematic Internet use and 3 studies accompanied by 4 effect sizes for problematic smartphone use. The total sample size was n = 1439 with a mean age of 20.34 (SD = 6.63) years. Psychological interventions were effective for both problematic Internet use (g = −1.41, 95% confidence interval = [−1.90, −0.91], p < 0.001) and problematic smartphone use (g = −0.40, 95% confidence interval = [−0.79, −0.01], p < 0.001).
Conclusion:
Current evidence indicates that psychological interventions can be effective in reducing problematic Internet use/problematic smartphone use. However, the results must be considered preliminary due to the limited number of studies available in the respective fields.
Introduction
The negative mental health effects of excessive technology use have been increasingly discussed in the public domain and in research since the beginning of widespread Internet use more than 20 years ago (Young, 1998).
The main areas of interest are problematic Internet use (PIU) and—more specifically—problematic smartphone use (PSU). PIU has been associated with a wide range of negative mental health consequences such as symptoms of distress, social withdrawal, familial conflicts and clinical conditions like social anxiety disorders or depression (Cerniglia et al., 2017). There is a convincing relationship between PSU and serious mental problems and symptoms (Grant et al., 2019; Winkler et al., 2020).
However, the main function of smartphones is the availability of the Internet. Thus, recent research has shown that PIU and PSU overlap in some key features, although not in all. Tateno et al. (2019) revealed a highly significant correlation of r = 0.67 (p < 0.0001) between Internet addiction measured by the Internet Addiction Test (IAT) and smartphone addiction as measured by the Smartphone Addiction Scale–Short Version (SAS-SV) in a Japanese sample. In their study, Lee et al. (2020) found a significant correlation of r = 0.49 (p < 0.001) between Young’s Internet Addiction Test (Y-IAT) and the Smartphone Addiction Scale (SAS).
Research has used the terms Internet addiction and smartphone addiction extensively to express similarities in key features of other substance-related and behavioral addictions such as excessive use, problems with impulse control, continuation of certain behavior despite conflicts at work and in the family, and withdrawal symptoms (Cash et al., 2012).
Especially, excessive online gaming has been addressed in recent reviews dealing with diagnosis and treatment (Costa and Kuss, 2019; Zajac et al., 2020). Gaming disorder has been included in the International Classification of Diseases, 11th Revision (ICD-11) in the group ‘disorders due to addictive behavior’, and Internet gaming disorder is part of the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (American Psychiatric Association (APA), 2013). Recent research reports insist that ‘general Internet addiction’ and ‘online gaming’ should be addressed separately from each other (Petry et al., 2018; Zajac et al., 2017). Thus, a ‘general Internet addiction’ is still not part of a disease classification system, but can be assigned to ‘other specific disorders due to addictive behaviors’ in the ICD-11 (Brand et al., 2020).
Since recent studies have disputed the assertion that mental health problems associated with excessive technology use can be regarded as addictions without playing down other addictions (Panova and Carbonell, 2018), current discussion focuses on development of valid criteria for considering if a problem behavior is an addictive behavior in line with ICD-11 (Brand et al., 2020). In this study, we use the designations PIU and PSU. In analogy to problem vs disordered gambling, PIU and PSU also include behaviors that may not fulfill all criteria to be considered as ‘addiction’ (Pfund et al., 2020). Thus, we understand PIU/PSU in this meta-analysis as the inability to control screen time, which is accompanied by serious consequences in daily life. Recently, we have clarified that these consequences can imply symptoms of dependence or dysfunctional social interactions (Augner and Hacker, 2012).
Despite these diagnostic controversies, it is unquestionable that PIU and PSU are a key public health concern given the ubiquitous dissemination of the Internet in general and, more specifically, of smartphone use. However, evidence of the effects of psychological interventions or psychotherapy is surprisingly fragmented and thus limited.
Winkler et al. investigated 16 pharmacological and psychological intervention studies on Internet addiction. The meta-analysis revealed a high level of effectiveness of the interventions in reducing levels of Internet addiction, cutting time spent online, as well as reducing depression and anxiety scores from pre- to post-treatment (Winkler et al., 2013). However, online activities may have changed and spread since this review was published.
Another review assessed psychological e-health interventions for PIU. However, since the authors identified only three articles meeting the study selection criteria, no meta-analysis was calculated and no convincing conclusions about effectiveness could be drawn (Lam and Lam, 2016).
Another narrative review identified studies from a wide range of interventions including prevention programs, psychosocial treatments (e.g. cognitive behavioral therapy [CBT]), pharmacotherapy and treatment camps. Unfortunately, the authors did not include information about their literature search strategy and did not calculate a meta-analysis. The studies concerned were partly rather old, and with very heterogeneous backgrounds (e.g. video gaming) (Nakayama et al., 2017).
Zajac et al. analyzed 13 intervention studies on Internet gaming disorder and 13 more on Internet addiction. However, the authors did not calculate a meta-analysis. They reported on methodical flaws in the available studies, such as small sample sizes, a lack of control groups and a lack of consistent definitions of Internet addiction (Zajac et al., 2017).
A recent review by Kim and Noh included five randomized controlled trials (RCTs) and six quasi-experimental studies. A meta-analysis indicated a significant reduction of symptom severity as a result of psychological interventions. Unfortunately, its validity is very limited due to the mixture of Internet addiction and Internet gaming disorder (Kim and Noh, 2019).
A recent meta-analysis supports the assumption that psychological interventions can be effective for Internet and smartphone addiction (Malinauskas and Malinauskiene, 2019). However, only six studies were included in the calculation, which combined Internet and smartphone addiction. In relation to PSU or smartphone addiction, there was only one review which dealt with exercise-based interventions in exclusively Chinese studies, and none with psychological interventions (Liu et al., 2019).
Due to a lack of robust evidence, the objective of this meta-analysis is to identify the available studies focusing on psychological interventions for PIU and PSU. Since PIU and PSU are related, but not identical, we aimed to identify studies for both, but to analyze them separately.
Methods
In accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) method (Moher et al., 2009; Walther et al., 2011), we prepared a review protocol that included a working title, review objective, search strategies, study selection criteria, interventions and end points.
Eligibility criteria and study selection
The objective of the study was to identify evidence of the effectiveness of psychological interventions on PIU and PSU. The inclusion criteria were that the studies:
Evaluated the effect of a psychological intervention and/or treatment and/or psychotherapy on PSU (including ‘smartphone addiction’) and PIU (including ‘Internet addiction’);
Used standardized questionnaires to assess PIU/PSU as the outcome;
Used a (quasi-) experimental design that included an intervention/control group;
Published or online first in peer review journals.
We excluded studies that:
Used psychopharmacological interventions.
Focused on Internet gaming or Internet pornography use.
Focused on clinical samples with significant comorbidities such as depression or anxiety; first, psychological interventions for other mental health problems have a different focus; second, even for significant comorbidities of substance abuse, therapeutic effectiveness and implications remain unclear and cannot be compared to treatment of each health issue alone (Hides et al., 2019).
Did not report relevant data in English.
Literature search
We conducted a systematic literature search in PubMed, PsyArticles, PsycInfo, Medline and Google scholar, whereby we used the following combinations of terms:
((addiction) OR (smartphone addiction) OR (cellular phone addiction) OR (problematic Internet use) OR (problematic smartphone use) OR (problematic cellular phone use)) AND ((treatment) OR (intervention) OR (psychotherapy)). We defined a time span for publication date in order to have at least somehow comparable Internet/smartphone disseminations. We chose 2008 as our earliest reference point, because proportion of worldwide Internet users crossed the 20% threshold shortly before 2008 and cellular phone subscriptions reached about 60% (ITU, 2019). We applied a time filter including studies published from 1 January 2008 to 1 January 2021 only.
Furthermore, we used backward snowballing from the reference lists of existing reviews on PIU or PSU (Kim and Noh, 2019; Lam and Lam, 2016; Malinauskas and Malinauskiene, 2019; Nakayama et al., 2017; Winkler et al., 2013; Zajac et al., 2017).
Screening abstracts
Two authors of the study screened the research literature. We identified relevant articles via three steps: (1) title, (2) abstract and (3) full text and imported them into Endnote X9. Two authors screened the records independently of each other. A consensus was reached via discussion or—if not resolvable—by a senior author’s decision. Duplicates were removed from the reference list (see Figure 1).
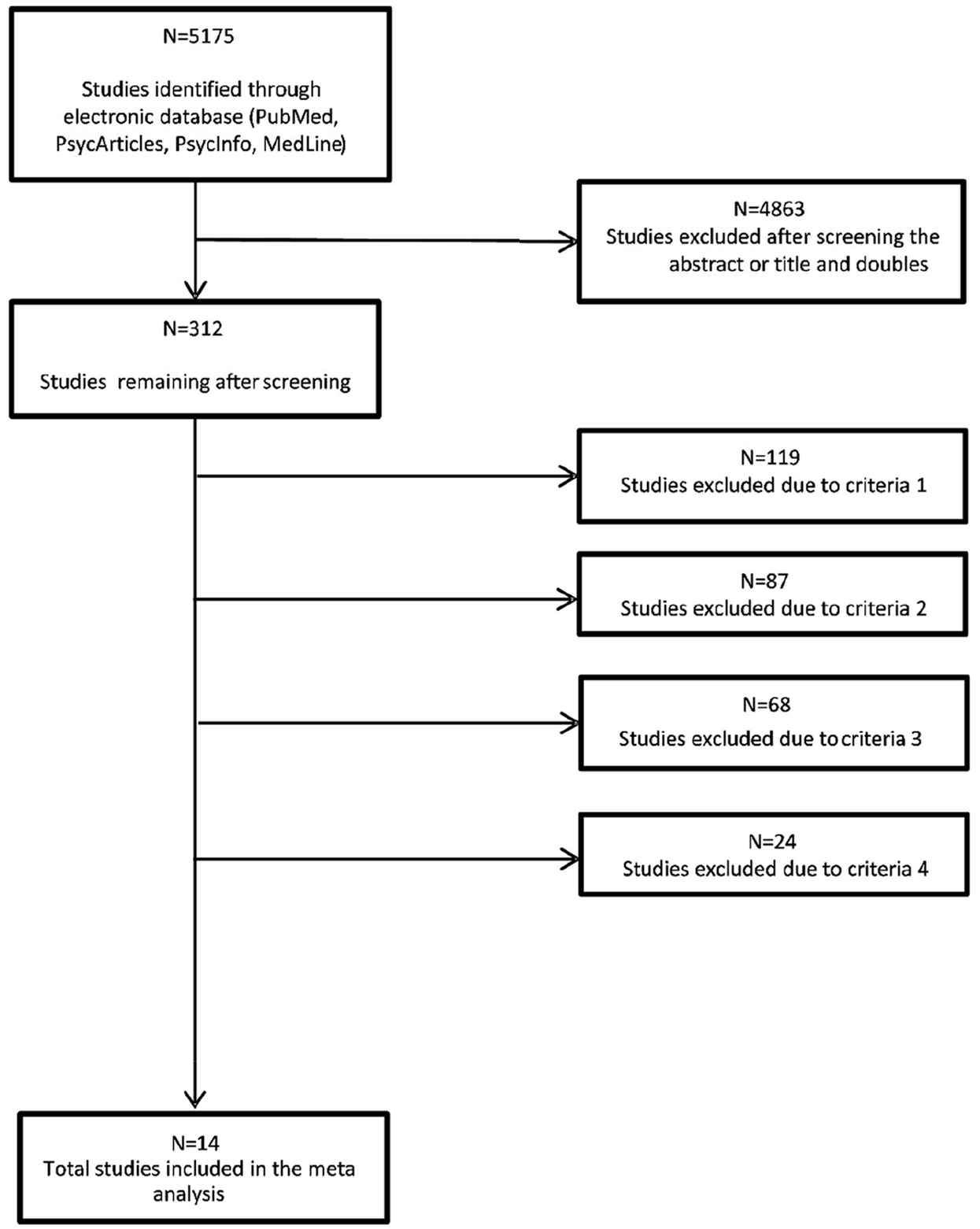
Flow chart study selection process.
Data extraction and quality assessment
Via a coding scheme which we developed, the data extraction was carried out by three authors. An inter-rater reliability of 0.97 based on mean rating and a two-way mixed-effects model (k = 3, absolute agreement) was computed and differences were solved by consensus. The variables of data extraction consisted of the authors of the publication, year of publication, effect sizes as well as the characteristics of the samples. If studies reported results for subgroups (e.g. gender) rather than for the total sample, groups were entered into the meta-analysis as independent samples. The quality of the methodology of the studies included was evaluated by all three authors using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (QATOCCSS) of the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH) (n.d.). This assessment tool consists of 14 questions regarding various methodological aspects (e.g. research process, sample size justification) and provides an overall score of bad, fair or good quality. An inter-rater reliability of 0.93 was estimated for study quality.
Data synthesis and analysis
Since the studies reported the mean difference between exposure and control groups for both outcome variables, Hedge’s g was selected as the effect size for the meta-analysis. In comparison to Cohen’s d, Hedge’s g leads to a more precise estimation of true effect sizes due to less bias, particularly in small sample sizes (Hedges, 1981). Cujipers et al. (2017) suggest avoiding pre-post effect sizes in meta-analysis focusing on the effects of therapeutic interventions. Since correlations between pre-post scores are hardly given, and the therapeutic setting and process as well as the patients influence the effect of the intervention, results are more biased with considerable errors in estimation. Due to this, Cuijpers et al. (2017) recommend using between-group mean differences since they control for these biased outcomes. Therefore, the meta-analytic results are based on the post-intervention between-group mean differences between the exposure and control groups. Regarding the direction of effect, positive effect sizes indicate higher scores in the exposure group, while negative effect sizes reflect higher values in the control group for Internet and smartphone addiction. Outliers in effect size were identified before calculating the average study effects by applying Cook’s distance (Viechtbauer and Cheung, 2010). A random-effects model with restricted likelihood estimator using Hedge’s invariance weighting was carried out for pooling the effect sizes with the appropriate 95% confidence intervals separately for Internet and smartphone addiction. For the quantification of the homogeneity of pooled effect sizes, τ2 was used, while Q statistic indicated significance levels (Cochran, 1954). Sensitivity analysis was carried out when heterogeneity of the effect sizes was given, while possible publication bias was examined by funnel plots and Egger’s tests (Egger et al., 1997), and p-hacking was addressed by p-curve diagrams and analyses (Simonsohn et al., 2014). Weighted mixed-effects meta-regressions were carried out regarding potential moderating effects, and subgroup analyses following a random-effects model further examined the heterogeneity of effect sizes. In general, statistical analyses were carried out using the software R with the metafor package (Viechtbauer, 2010).
Measurement of PSU/PIU
All studies included in this meta-analysis used questionnaires to assess PSU and PIU (see Table 1).
Raw data for the meta-analysis.
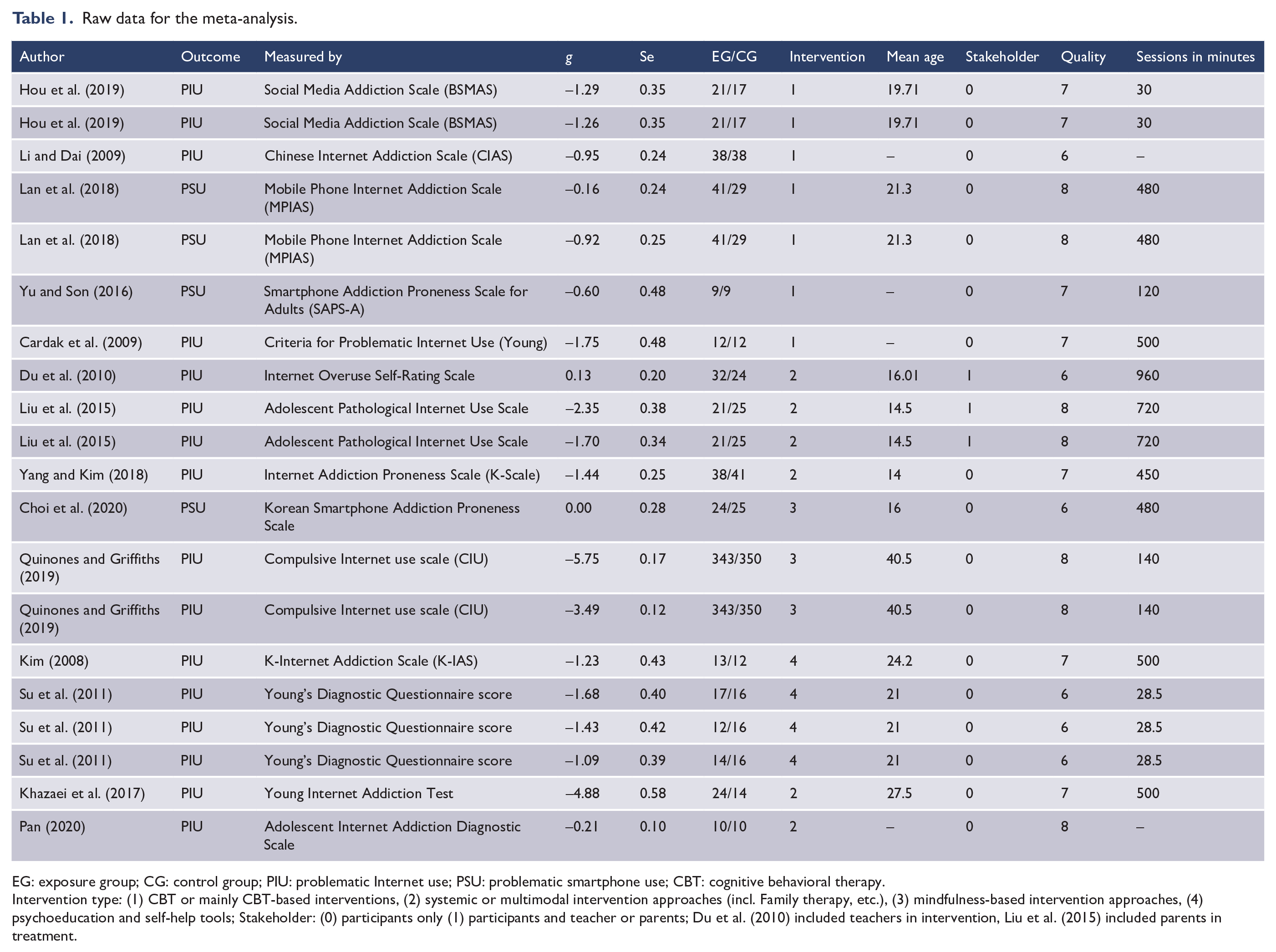
EG: exposure group; CG: control group; PIU: problematic Internet use; PSU: problematic smartphone use; CBT: cognitive behavioral therapy.
Intervention type: (1) CBT or mainly CBT-based interventions, (2) systemic or multimodal intervention approaches (incl. Family therapy, etc.), (3) mindfulness-based intervention approaches, (4) psychoeducation and self-help tools; Stakeholder: (0) participants only (1) participants and teacher or parents; Du et al. (2010) included teachers in intervention, Liu et al. (2015) included parents in treatment.
Instruments varied between the studies. However, for PIU most common symptoms assessed were compulsive Internet use, negative outcomes, mood alterations (withdrawal) and tolerance (Cardak et al., 2009; Khazaei et al., 2017; Kim, 2008; Liu et al., 2015; Pan, 2020; Quinones and Griffiths, 2019; Su et al., 2011; Yang and Kim, 2018). Where reported, reliability of measurements was high and Cronbach’s alpha values of the instruments above 0.80 (Hou et al., 2019; Kim, 2008; Liu et al., 2015; Pan, 2020; Quinones and Griffiths, 2019; Yang and Kim, 2018).
For PSU only one study reported psychometric details about the instrument used. The Korean Smartphone Addiction Proneness Scale includes subscales ‘daily life disturbance’, ‘directivity to virtual world’, ‘tolerance’ and ‘withdrawal’. Reliability in the primary study was high (Cronbach’s alpha = 0.88) (Choi et al., 2020).
Treatment classification
Two authors defined the intervention types used in the studies and assigned one intervention type to each study (see Table 1):
(a) CBT or mainly CBT-based interventions, i.e. interventions that involve elements of cognitive reconstruction and/or behavioral changes. Hou et al. (2019) for example used reflection questions to cognitive reconstruct social media use (e.g. ‘Why did they use social media and were there alternative way to achieve the purposes?’) and behavioral change strategies to reduce online time (Hou et al., 2019).
(b) Systemic or multimodal intervention approaches (including family therapy, etc.), i.e. interventions that include family environment of participants and/or used different modalities to address PIU or PSU. Interventions in Liu et al. (2015) focused on parent–adolescent interaction, while Pan (2020) for example used a set of psychological and sports interventions (Liu et al., 2015; Pan, 2020).
(c) Mindfulness-based intervention approaches, i.e. interventions that use meditation as essential part of the therapeutic process. Choi et al. (2020) for example used mind subtraction meditation to reduce PSU (Choi et al., 2020).
(d) Psychoeducation and self-help tools, i.e. intervention that focused mainly on providing information about PSU or PIU, e.g. Su et al. (2011) used an online expert system named Healthy Online Self-helping Center (HOSC) (Su et al., 2011).
Differences in classification among the authors were resolved by discussion.
Stakeholder inclusion
Furthermore, we identified whether the intervention only addressed the target group (stakeholder = 0) or included teachers and/or parents (stakeholder = 1) in any way.
Results
Study characteristics
Overall, we included 13 studies accompanied by 18 effect sizes, achieving a total sample of n = 1439 participants with a mean age of 20.34(SD = 6.63) years, while the publication date ranged from 2008 to 2020. In general, seven effect sizes (38.89%) are based on cognitive behavioral interventions, five effect sizes (27.78%) followed systemic intervention approaches while two effect sizes (11.11%) come from mindfulness-based interventions and four effect sizes (22.22%) are based on psychoeducation. Overall, the study quality was considered fair to good, while in most studies information about the characteristics of the sample, intervention process and statistical analyses was lacking. The total mean duration of therapeutic intervention across all studies was 356.00 (SD = 301.43) minutes.
Meta-analytic results
PIU
For PIU, the test for homogeneity indicated heterogeneous effect sizes of the included studies, Q(13) = 504.84, p < 0.001, with τ2 = 0.78. The random-effect model meta-analysis across 10 studies including 14 effect sizes showed significant differences between exposure and control groups with g = −1.41 (95% confidence interval from −1.90 to −0.91, p < 0.001). Therefore, individuals participating in psychotherapeutic treatment show significantly lower scores in PIU than their controls (see Figure 2).
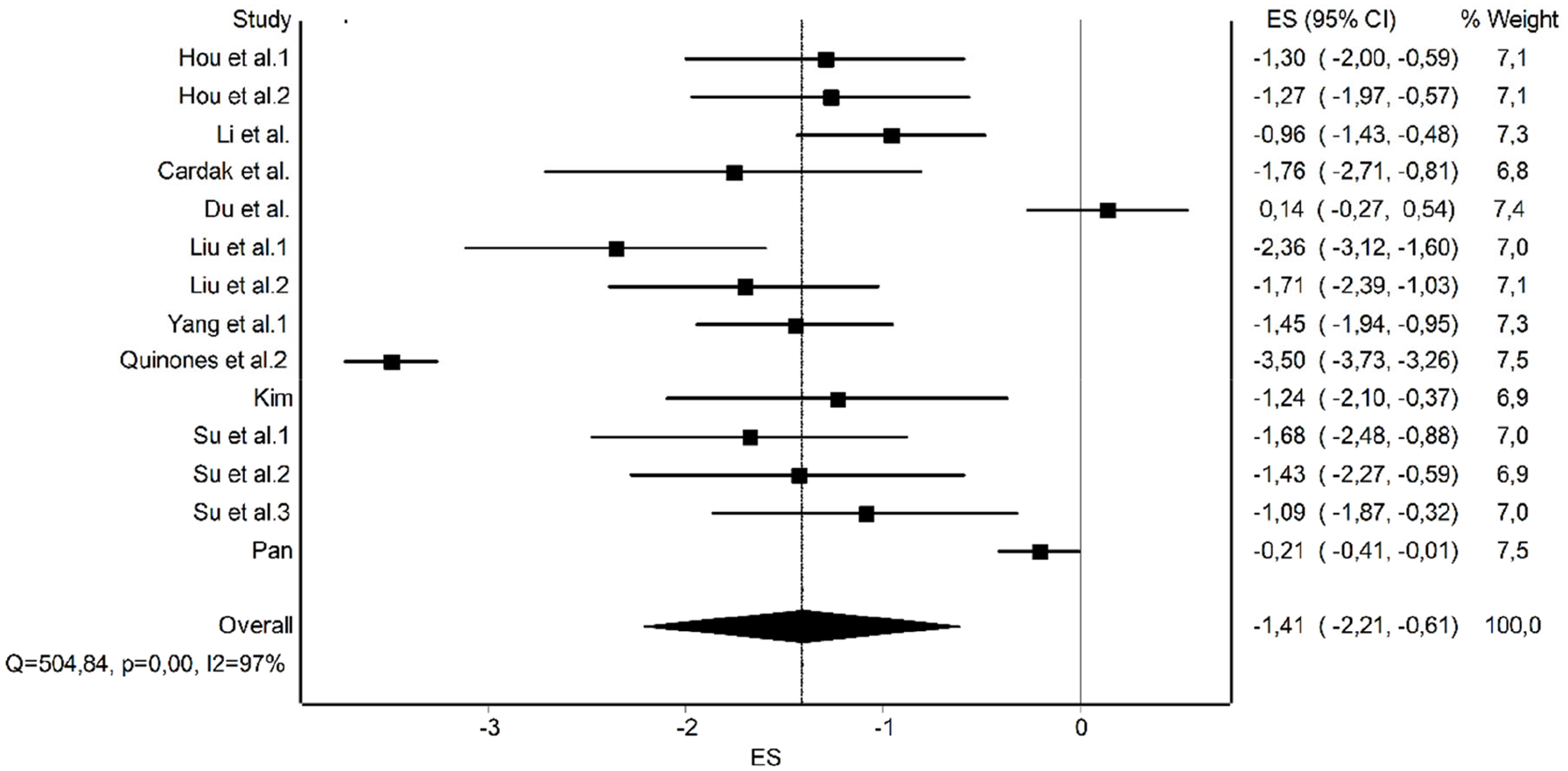
Forest plot PIU.
PSU
The homogeneity test showed homogeneous effect sizes regarding the included studies for PSU, Q(3) = 7.28, p = 0.06, with τ2 = 0.06. A random-effect model meta-analysis including three studies with four effect sizes showed significant differences between exposure and control groups with g = −0.40 (95% confidence interval from −0.79 to −0.01, p < 0.001). According to this, individuals exposed to psychotherapeutic treatment show significantly lower scores in PSU than individuals in the control group (see Figure 3).
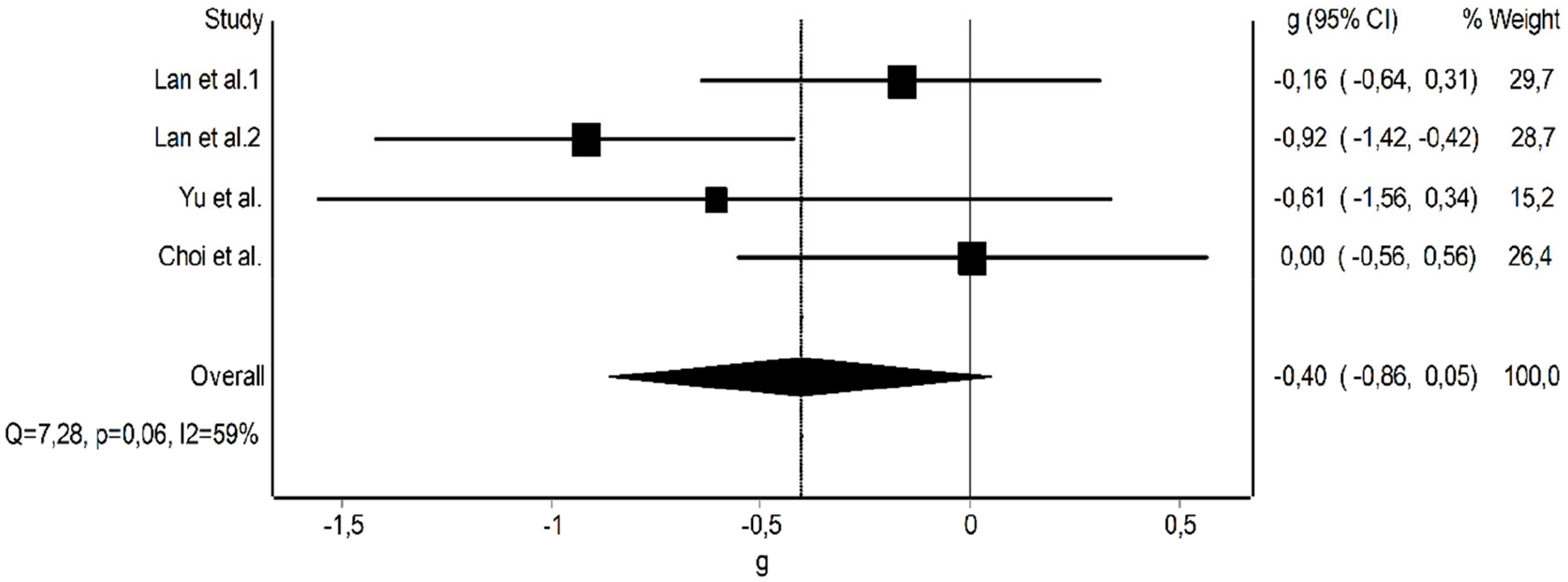
Forest plot PSU.
Sensitivity analysis
Outliers
Before computing the results, we excluded two effect sizes from two different studies (Khazaei et al., 2017; Quinones and Griffiths, 2019) from entering the meta-analysis for PIU, since their magnitude of effect differs substantially from the remaining studies (g = −5.75 for the mindfulness intervention in Quinones and Griffiths, 2019, and g = −4.88 for a range of positive psychology interventions in Khazaei et al., 2017, see further details in Table 1).
In general, three effect sizes from three studies (Du et al., 2010; Pan, 2020; Quinones and Griffiths, 2019) were detected as outliers by the analysis. Removing these outliers resulted in a homogeneity of effect sizes of, Q(10) = 12.24, p = 0.27, regarding PIU across 7 studies with 11 effect sizes while reducing τ2 from 0.78 to 0.04. Exclusion of outliers increased the magnitude of the effect size and the meta-analytic model remained significant with g = −1.43 (95% confidence interval from −1.67 to −1.204, p < 0.001). Further examination revealed that the reason for detection as outliers was either a disproportionate sample size or magnitude of effect in comparison to the remaining studies. Therefore, heterogeneity seems to be driven by these outliers.
No outliers could be detected in the included studies for PSU.
Subgroup and moderator analysis
For the subgroup analysis, PIU interventions based on mindfulness were excluded since only two studies, Choi et al. (2020) and Quinones and Griffiths (2019), were comparable. No significant subgroup differences could be found in relation to the type of intervention, Q(2) = 0.92, p = 0.63. Regarding moderator analysis, while mean age of the participants, χ2(1) = 6.70, p = 0.01; r2 = 0.42, b = −0.08, showed a significant moderation of effect sizes, neither publication year, χ2(1) = 0.64, p = 0.42; r2 = 0.00, b = −0.05, quality of the study, χ2(1) = 2.65, p = 0.10; r2 = 0.12, b = −0.48, stakeholder, χ2(1) = 0.09, p = 0.76; r2 = 0.00, b = 0.19, nor the duration of the intervention, χ2(1) = 0.86, p = 0.35; r2 = 0.02, b = 0.00, did. However, when entering all variables as multiple moderators in a meta-regression, χ2(5) = 31.77, p < 0.001; r2 = 0.78, bpublicationyear = 0.03, bmeanage = −0.04, bstakeholder = −0.17, bstudyquality = −0.92, bdurationintervention = 0.00, the moderating effects of mean age of participants did not remain significant (p = 0.62).
Due to the small sample size, no meaningful subgroup and moderator analysis could be carried out for PSU.
Publication bias and p-hacking
The funnel plot does not visually suggest publication bias regarding the included studies and Egger’s test does not show significant results (p = 0.94) (see Figure 4). When testing for p-hacking by conducting p-curve analysis, effect sizes showed significant right-skewness (p < 0.001) and non-significant flatness (p = 0.99), indicating robustness against p-hacking (see Figure 5). Therefore, the results regarding the overall effect size of Internet addiction do not seem to be influenced by either publication bias or p-hacking. Again due to the small sample size, no meaningful analysis of publication bias or p-hacking could be carried out.
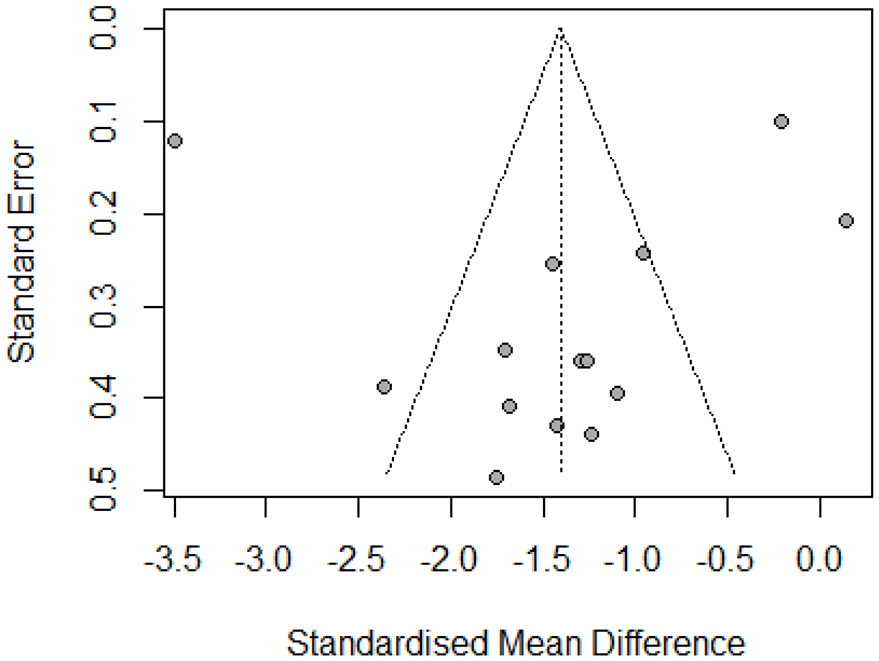
Funnel plot PIU.
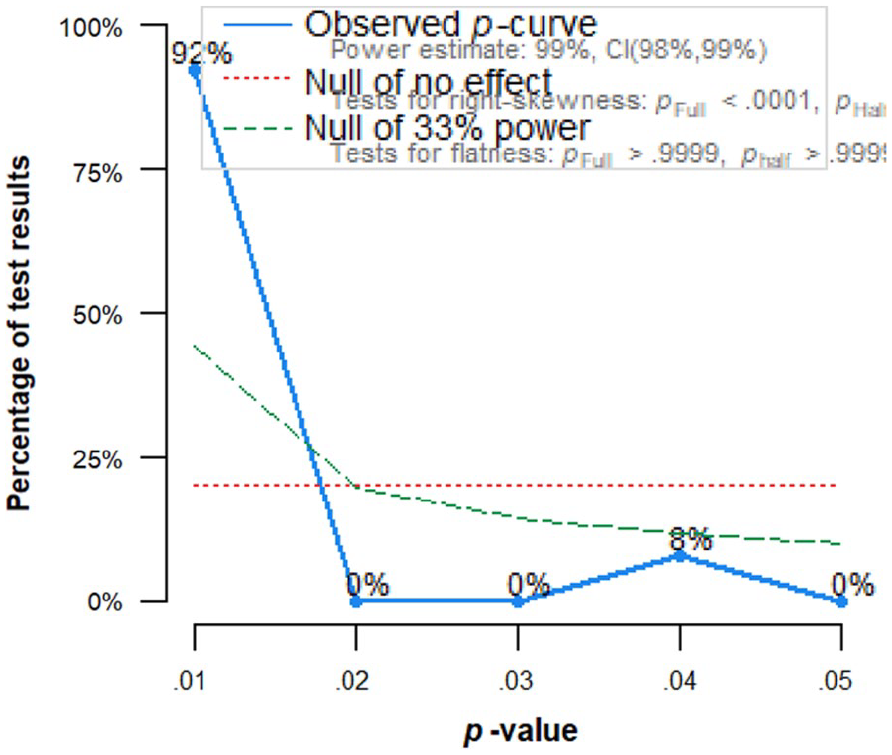
P-curve diagram PIU.
Discussion
PIU and PSU manifest a clear public health issue. Psychological interventions could possibly help to avoid or reduce negative behavioral and health effects of Internet and smartphone use. Indeed, the results of this meta-analysis indicate that psychological interventions can significantly reduce PIU/PSU scores measured by standardized questionnaires. Overall, the effect size can be regarded as high for PIU (Hedges g = −1.41, p < 0.001) and moderate for PSU (Hedges g = −0.40, p < 0.001).
The effects of psychotherapeutic interventions on different mental health problems are relatively well established. A recent meta-analysis reported significant effects of psychotherapy on depression (standard mean difference (SMD) = 0.71) (Munder et al., 2019). Furthermore, a review showed that CBT can reduce Internet gaming disorder symptoms (g = 0.92; [0.50, 1.34]) (Stevens et al., 2019).
We did not find significant differences between different intervention methods for PIU. Recent evidence rejects the assumption that special types of psychotherapy (e.g. CBT) may be more effective than other types. On the contrary, so-called non-specific aspects of psychotherapy and psychological interventions (e.g. format of the intervention, frequency, empathy or the motivation of the therapist) are decisive. Palpacuer et al. (2017) reported in a meta-analysis that the effects of different psychotherapy methods on depression failed to be significant in relation to a waiting-list control group when adjusted for non-specific aspects. If specific aspects of psychotherapy methods are of less importance, it is plausible that a wide range of different psychological interventions may be effective in reducing PIU/PSU scores.
Although PIU/PSU cannot be classified as disorders, addictions or illnesses, we can make analogies from psychotherapeutic research on the mode of functioning of psychological interventions that more or less reduce the problematic issues of Internet and smartphone use.
First, a convincing body of evidence suggests that the core symptoms of addictive behaviors in general include impaired self-control and increased stress reactivity (Tang et al., 2015). A wide range of psychological interventions focus directly or indirectly on these self-control and self-regulation functions.
Thus, several studies included in this meta-analysis have used elements that address self-control and self-regulation in the psychological intervention. Yang et al. integrated self-regulation strategies into their intervention. The experimental group improved significantly—not only in Internet addiction scores but also in self-control (Yang and Kim, 2018). Hou et al. (2019) based their interventions on considerations about self-regulation. Further evidence indicates that impaired self-control is the best predictor of problematic social media use (Blachnio and Przepiorka, 2016).
The physiological correlates of self-control problems are located in different areas of the brain. Decreased activity of the anterior cingulate cortex (ACC) and prefrontal cortex (PFC) and reduced connectivity between the ACC and striatum seem to be decisive for lower self-control and higher proneness to addictive behaviors (Tang et al., 2015). Moreover, in relation to Internet addiction, recent research indicates that dysfunctions in ACC and PFC as part of the default mode network (DMN) might lead to deficits in cognitive control and to reduced cognitive efficiency. This might also be associated with attention problems. Deficits of the inhibitory control network as identified in persons with a high PIU via task-related functional magnetic resonance imaging (fMRI) are responsible for the inability to stop or control online behavior (Darnai et al., 2019). There is neuropsychological evidence that different forms of therapy, e.g. mindfulness-based therapy and CBT, can significantly modulate the DMN (Fahmy et al., 2019; Li et al., 2018).
Besides individual and neuropsychological aspects of self-control and PIU/PSU, there are some social and cultural factors to be taken into account. A recent commentary underscores the relevance of social determinants of addictive behaviors (e.g. weak social ties, social exclusion, hyper-individualism) and hypothesizes that our society is somehow organized to consume and therefore to undermine our self-control (Van der Linden, 2015). This seems to be especially true for Internet and smartphone use and closely related behaviors like social media use.
However, this meta-analysis has some limitations. We evaluated exclusively short-term effects, since most studies did not include follow-ups. Actually, one main problem is that we have surprisingly little information about the long-term natural course of PSU/PIU which would determine the necessity of psychological intervention. One study reported that in a group of adolescent Internet addicts, a total of 71 were regarded as remissions and 67 as persistent addicts after 1 year (Ko et al., 2014). Another paper reports that Internet gaming disorder is relatively unstable over time; however, persistent rates vary between 26.5% after 2 years and 50% or 86% after 1 year (Mihara and Higuchi, 2017). Thus, there is a clear need for more research in this area, since a significant reduction in PSU/PIU scores might take place without any intervention.
Furthermore, there are some methodological issues to be taken into account. First, treatment types varied between studies. In some studies, superficial descriptions of procedures made it difficult to classify the intervention (classifications see Table 1). Second, we did not include studies in our meta-analysis that focused on clinical samples with significant comorbidities such as depression or anxiety. Although comorbidity rate between PSU/PIU is high, we aimed to isolate effects of psychological treatments on PIU/PSU, since psychological interventions for other mental health problems have a different focus. Furthermore, recent evidence for substance abuse disorder and depression as comorbidity indicate that therapeutic effectiveness and implications cannot be compared to treatment of each health issue alone (Hides et al., 2019). Nevertheless, this selection process may have influenced our results. Most probably, our sample is mentally healthier than clinical samples are. Thus, meaningfulness of our results on clinical samples may be limited. Third, the heterogeneity of effect sizes was given for the outcome ‘problematic Internet use’. Sensitivity analysis revealed that the inhomogeneous results are mainly driven by outliers. Although removal of these outliers reduced the magnitude of this effect to some degree, the pooled effect size remained significant while showing robustness against publication bias and p-hacking. In contrast, we found homogeneous effect sizes for PSU. However, due to the small sample size of studies, no meaningful sensitivity analysis could be carried out regarding the outcome. The interpretation of our results concerning PSU can thus only be regarded as preliminary. Consequently, we would recommend that future studies should increasingly focus on evaluating the effects of psychological interventions on PSU.
The present meta-analysis indicates that psychological interventions can be effective in reducing PIU/PSU scores in the short term. Against the background of the available evidence, interventions that directly or indirectly affect self-control functions may be especially effective. However, future research should focus on long-term effects of interventions. Moreover, the general lack of studies with high-quality designs in this research area should be addressed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Data Availability
This study is a meta-analysis, and all data are available in the public domain.