
Abstract
Objective:
Post-diagnosis service delivery for young-onset dementia (with onset prior to 65 years) recently moved to the disability system in an attempt to address systemic barriers to best practice in aged care. The objective of this study was to examine experiences and satisfaction with disability services so far among people with young-onset dementia and their care partners and identify strategies for service and system improvement.
Methods:
The 151 participating Australians living with young-onset dementia or providing informal care to a person with young-onset dementia were recruited via social media, advocacy bodies and specialist medical clinics. A cross-sectional online survey asked participants to provide a timeline of their interactions with the disability system so far and rate their satisfaction with the disability system, aged care and disability services.
Results:
Participants reported a mean age at symptom onset of 55 years. In all, 53% were diagnosed with Alzheimer’s disease and 25% were diagnosed with frontotemporal dementia. Sixty percent had received an approved plan from the National Disability Insurance Scheme, although 3% were rejected. More than 27% waited longer than 6 months to receive their plan, and half waited at least a month post-approval to access services. Less than 30% agreed that the National Disability Insurance Scheme understands dementia, and fewer than half felt that the process of accessing National Disability Insurance Scheme funding is easy and fast enough. Nonetheless, respondents remained overwhelmingly in favour of young-onset dementia services remaining in the disability system rather than in aged care.
Conclusions:
While people with young-onset dementia and their care partners strongly agree with their inclusion in the National Disability Insurance Scheme, a relatively low level of experience with dementia in the disability workforce and a lack of integration with the healthcare and aged care systems continue to create important barriers for accessing the services they need.
Introduction
Young-onset dementia (YOD), with symptom onset prior to 65 years, accounts for up to 10% of all dementias internationally (Withall et al., 2014). Young people with dementia and their families commonly experience higher levels of stress and burden than older people with dementia owing to their relatively greater family, financial and occupational responsibilities (Arai et al., 2007; Hvidsten et al., 2014, 2018). Diagnosis is often delayed by several years (Draper et al., 2016) partly because people with YOD are at high risk of misdiagnosis (Loi et al., 2020).
Internationally, most post-diagnosis care for people with dementia is integrated into the aged care and/or healthcare system and delivered via primary care, hospitals and aged care organisations (Draper et al., 2018). This has historically been problematic for people with YOD, who report difficulties accessing services because of bureaucratic (e.g. age limits) and practical barriers (e.g. no available child care) (Cations et al., 2017). More importantly, people with YOD are reluctant to engage with services designed for people older than them. Some evidence suggests that receiving inappropriate dementia care can hasten cognitive decline (Tolhurst et al., 2014). Accordingly, people with YOD and their families report a strong preference for services that are tailored to their unique circumstances and needs (Cations et al., 2017; Stamou et al., 2020). This has created barriers to service access as there have been few YOD-specific services (Cations et al., 2017).
In 2016, YOD was included as an eligible condition for the Australian National Disability Insurance Scheme (NDIS). The introduction of the NDIS in 2013 was a revolution for social care in Australia, as the Australian Government implemented an insurance model to cover the lifetime costs of disability-related care for those with permanent and significant disability (Australian Government, 2013; Walsh and Johnson, 2013). For the first time, the NDIS provides people with a disability a legislated entitlement to care and support (Reddihough et al., 2016). The individualised funding model of the NDIS is a shift from the block-funding model used previously in the disability sector and currently for aged care (Collings et al., 2016).
People with YOD are eligible to access NDIS funding if they have a dementia diagnosis and make an ‘access request’ prior to turning 65 years old. They must also meet the standard NDIS eligibility criteria including that their impairments cause substantially reduced capacity to undertake one or more relevant activities such that social or economic participation is diminished (Joint Standing Committee on the National Disability Insurance Scheme, 2020). The NDIS funds can be used to access reasonable and necessary services and supports to help the person to achieve their goals, including assistance with daily living, transport, assistive technology, allied health and social programmes. Allied health services may also be available via the health system, but availability and eligibility for these services vary between regions (Low et al., 2020). Importantly, NDIS funding cannot be used to access medical care services or support services for informal carers (aside from respite) (Australian Government, 2013). Once the person turns 65 years old, they can choose to remain an NDIS participant or move to the aged care system.
People with YOD and their families initially welcomed their inclusion in the NDIS because, in theory, the premise of the NDIS is consistent with evidence-based recommendations for YOD service design (Cations et al., 2017): they are consulted to determine the needs most important to them, are afforded choice and flexibility in deciding how to use their funding, and can be supported and guided by a centralised and consistent plan manager. The conceptualisation of dementia in young people as causing disability, and therefore eligible for NDIS inclusion, is a novel approach and is unique internationally (Cations et al., 2018; Clare, 2017; Draper et al., 2018; Shakespeare et al., 2019). This conceptualisation is consistent with growing advocacy from consumer groups who argue that dementia and its secondary effects reduce workforce and community participation consistent with the World Health Organization’s definition of disability (Dementia Alliance International, 2016).
However, it is not yet known how effectively care provision for people with YOD under the NDIS is meeting its intended aims. Advocacy bodies have raised concerns about the disability sector’s lack of experience with dementia especially considering that progressive illnesses are relatively uncommon in the NDIS (compared with, for example, intellectual disability or autism spectrum disorder) (Neurological Alliance Australia, 2017). Anecdotal reports note that people with YOD may have difficulty meeting the NDIS eligibility requirements (Coleman, 2018) and that the yearly review practices of the NDIS may be insufficient to adapt to the sometimes rapidly changing needs of a person with YOD (Neurological Alliance Australia, 2017). Understanding the initial experiences of people with YOD and their families with the NDIS will assist with fine-tuning service design and delivery efforts. As such, the aim of this study was to examine the experiences of people with YOD and their care partners with the NDIS, determine satisfaction with NDIS services and identify strategies for service and system improvement for this group.
Materials and methods
Design and participants
We conducted an online cross-sectional survey of Australians living with YOD and informal (i.e. unpaid) care partners of a person with YOD from October 2019 to July 2020. As the national roll-out of the NDIS was completed in 2020, there was geographical variation in NDIS availability over time. Participants were recruited via social media, newsletters circulated by Dementia Australia and other peak bodies representing people with YOD, snowball sampling and the StepUp for Dementia Research platform in which people with dementia and their families opt in to be informed of research trials seeking participants (The University of Sydney, 2019). Flyers were also available in specialist memory clinics inviting eligible participants to complete the survey (Queen Elizabeth Hospital in South Australia, Hornsby Hospital in New South Wales and the Royal Brisbane and Women’s Hospital, Queensland). Eligible participants were (a) living with a diagnosis of YOD or providing informal care to a person with YOD and (b) able to provide informed consent to participate. People with YOD (with symptom onset prior to 65 years) who were aged >65 years at the time of survey completion were eligible to participate. Participants were not required to have accessed the NDIS, as the survey sought to gather a wide range of experiences. People providing paid support to a person with YOD or who used to provide support to a person with YOD who had died were excluded from this analysis. Recruitment continued until responses slowed to include less than one new participant per week.
Assessment
The online survey (see in full in Supplementary Table S1) gathered demographic data about the person with YOD, including age at symptom onset and at diagnosis, living situation, country of birth, type of dementia and diagnosing physician type. The severity of functional disability was self- or carer-reported using the 12-item self-administered version of the World Health Organization Disability Assessment Schedule 2.0 (WHODAS) (Ustun et al., 2010), in which respondents are asked to rate difficulty in the past 30 days with a range of cognitive and functional tasks (e.g. learning a new task, joining in community activities, washing whole body) on a scale from 1 (none) to 5 (extreme or cannot do). Scores are summed to indicate a total disability burden (range, 12–60), with high internal consistency (α = 0.90–0.97) (Sousa et al., 2010) and good discriminating validity for identifying varying levels of disability (Luciano et al., 2010).
Survey questions about NDIS experiences were designed specifically for this research project by the research team, which includes clinical and research experts in YOD post-diagnosis care and consumer experts (i.e. people with YOD and care partners; Supplementary Table 1). The survey was piloted with three people with YOD and/or care partners and refined to improve the clarity of the question wording. Respondents were first asked about their engagement with the NDIS to date, including whether they had heard of the NDIS, knew that YOD was an eligible condition in the NDIS, had made an access request, received an access decision, participated in a planning meeting and/or received an NDIS-approved plan. Those who had received an approved plan were asked how long they waited from the time of access request to receipt of their plan and whether they received help with the process. Those who had accessed services with their plan were also asked to indicate how long they waited to access the service. Finally, participants were asked to rate their satisfaction with the NDIS and disability services by indicating their agreement with a series of statements (e.g. ‘I am happy with my NDIS plan’, ‘Disability providers are good at responding to my needs’) on a 5-point scale from 1 (completely disagree) to 5 (completely agree).
Analysis
Analysis was conducted using SPSS statistical package version 22 (SPSS Inc, 2017). Results are presented descriptively using percentages and averages. Differences in experiences and satisfaction with services were examined comparing (a) respondents with YOD and care partners completing the survey on behalf of a person with YOD, (b) people with Alzheimer’s disease (AD) compared with people with other types of YOD and (c) people living within and outside major cities. These factors impact service access and satisfaction for people with dementia (Draper et al., 2016; Sansoni et al., 2014). Comparisons were conducted using chi-square tests or independent-samples t-tests (with α = 0.05) depending on data type and sample distribution. Missing data were managed via case-wise deletion.
Ethics
Ethical approval for this study was provided by the Flinders University Social and Behavioural Research Ethics Committee (project 8331).
Results
Participants were 42 people with YOD and 109 people providing care for a person with YOD (Table 1). Three of the care partners reported about people with YOD who also completed the survey themselves, but their responses are retained here to provide dual perspectives. People with YOD who completed the survey were 61 years old on average and 48% were female. Half of the respondents with YOD were living outside a major city, 76% were born in Australia and all were living in the community (i.e. not in residential aged care) at the time of survey completion. In all, 45% had a diagnosis of AD, while 38% were diagnosed with frontotemporal dementia (FTD), with median age at symptom onset of 54 years and age at diagnosis of 57 years. Care partners were aged 56 years on average (range, 20–73 years) and were spouses (65%), children (19.8%), parents (2.7%) or friends of people with YOD (12.6%). Twenty-six care partners (23.9%) supported a person with YOD living in residential aged care or supported disability accommodation at the time of survey completion. In total, 56% of care partners supported a person with AD, while 19% supported a person with FTD, with a median age at symptom onset of 55 years and age at diagnosis of 58 years. People with YOD who completed the survey themselves reported a lower level of functional disability overall compared with those whose care partners completed the survey (t =−4.23, df = 94.7, p < 0.001).
Characteristics of sample.
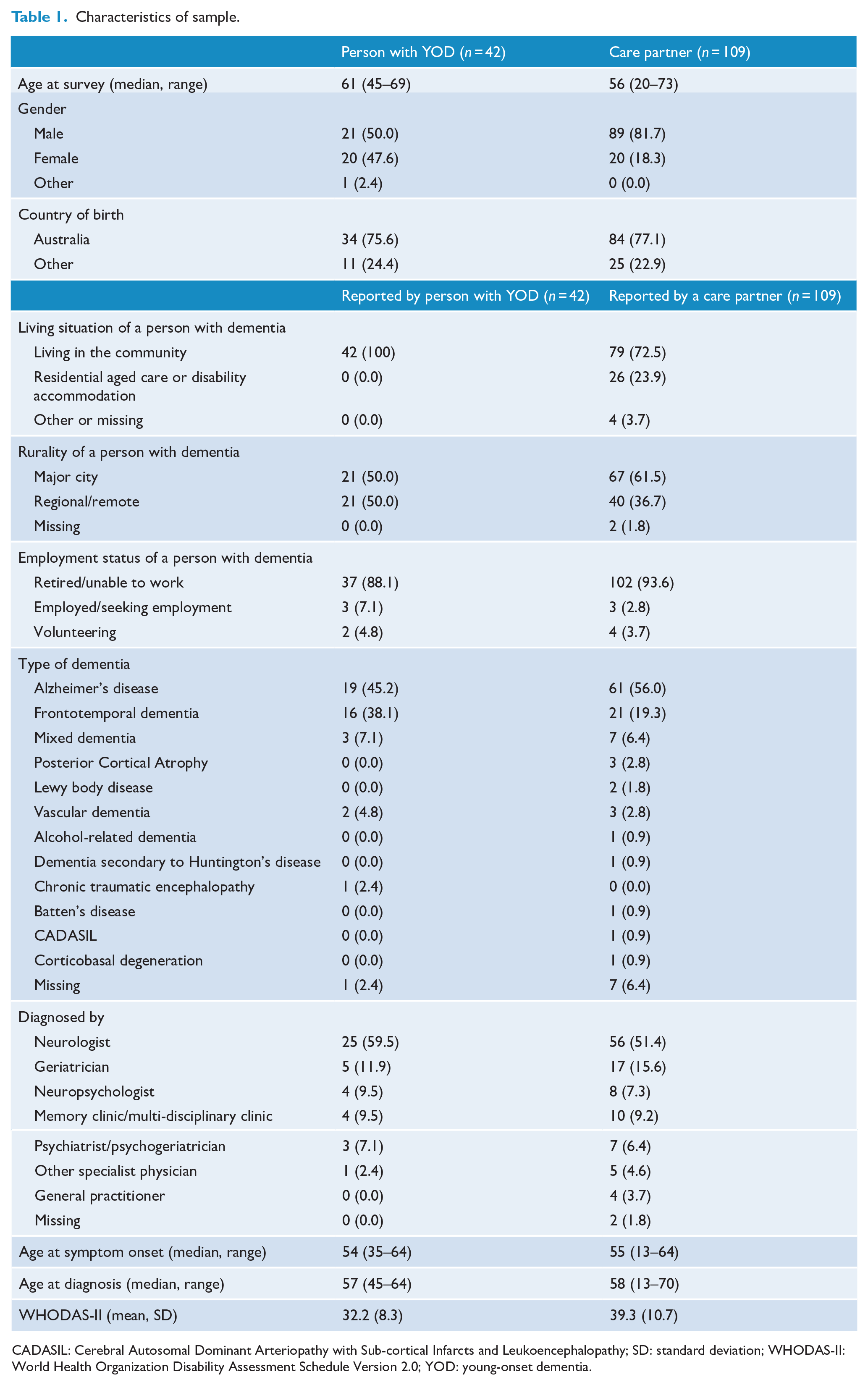
CADASIL: Cerebral Autosomal Dominant Arteriopathy with Sub-cortical Infarcts and Leukoencephalopathy; SD: standard deviation; WHODAS-II: World Health Organization Disability Assessment Schedule Version 2.0; YOD: young-onset dementia.
Figure 1 demonstrates engagement with the NDIS among our sample, with most being aware that YOD is an eligible NDIS condition and more than 60% receiving an approved NDIS plan. A small group of participants (n = 5) made an access request but were deemed ineligible by the NDIS. Reasons given for ineligibility included that their impairments were not considered to cause ‘significant disability’ (n = 1), the assessor was not aware that YOD was an eligible condition (n = 3) or they turned 65 during the assessment process and were diverted to the aged care system (n = 1). Thirty-eight per cent of the sample had been an NDIS participant for at least a year and participated in a second planning meeting. Most participants reported that the time from making an access request to receiving an approved plan took 1–6 months, although 27% waited longer than 6 months. Twenty-two respondents with YOD (52%) and 67 people with YOD whose care partner completed the survey (61%) had the help of a family member or friend to access the NDIS. Thirty-six per cent of each group engaged the help of a YOD Key Worker, an advisory service delivered by Dementia Australia to help people with YOD navigate support services until mid-2019. Whether respondents waited longer than 6 months for their NDIS plan was not affected by the use of the Key Worker service (χ2 = 0.24, df = 1, p = 0.62), living within or outside a major city (χ2 = 1.34, df = 1, p = 0.25) or whether the person with YOD had AD or another dementia type (χ2 = 0.04, df = 1, p = 0.85).
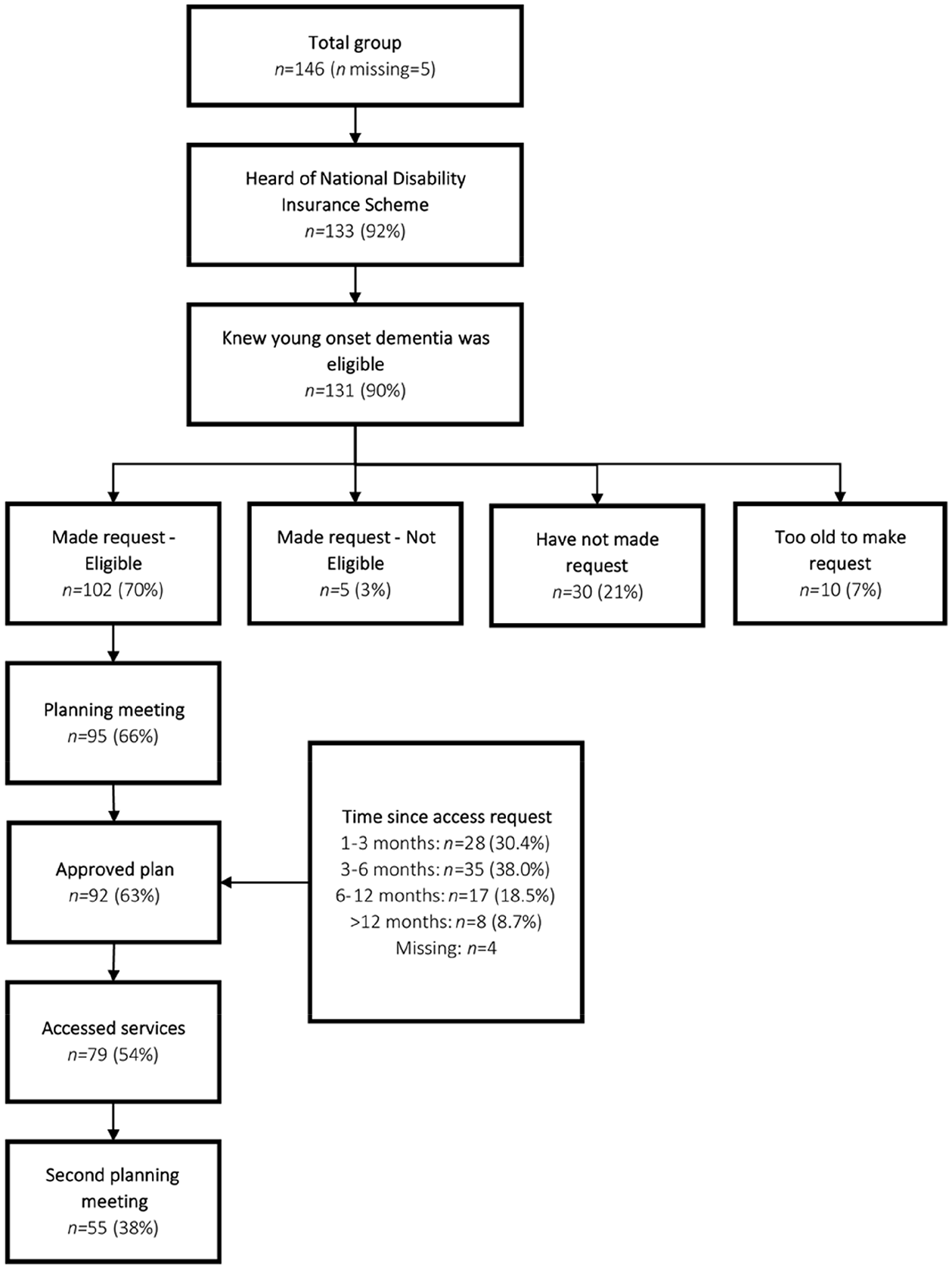
Experience with the National Disability Insurance Scheme among participants so far.
The most common services approved by the NDIS for our sample were in-home support, allied health, transport and social support (including day respite centres) (Table 2). Those who had accessed the service by the time of survey completion usually encountered only a brief wait time, finding a service within a month. However, more than half of those approved for home modifications, allied health services, counselling or psychology, and residential aged care waited at least a month to access the service.
Services approvals and time taken to find the service.
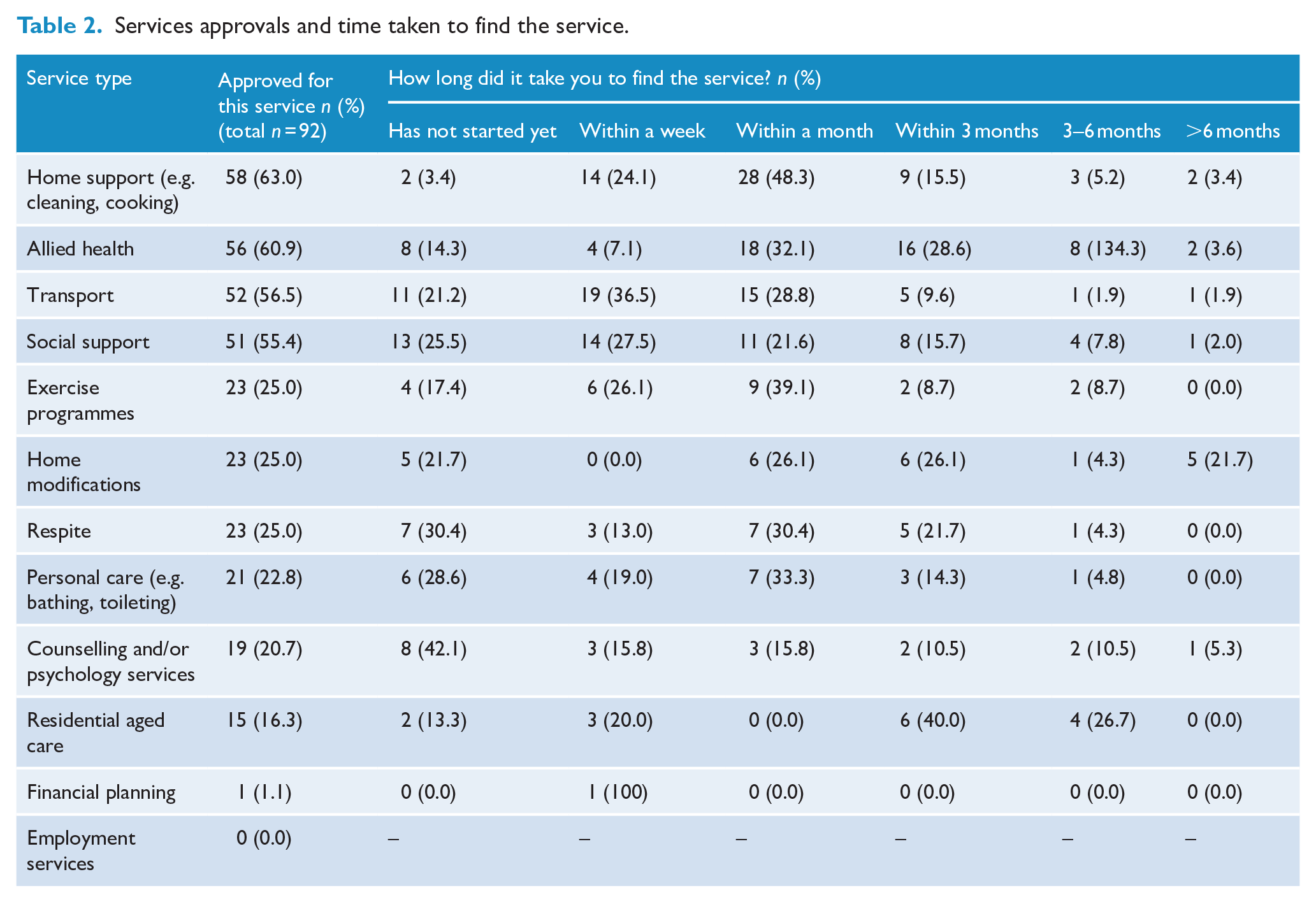
Figure 2 displays the overall participant satisfaction with the NDIS and disability care services. Most participants disagreed that the NDIS understands dementia and particularly the physical needs of people with dementia, and fewer than half endorsed the statement that the process of accessing NDIS funding is easy and fast enough. Nonetheless, more than 60% of those who received an NDIS plan were satisfied with the plan. There were no differences in plan satisfaction (i.e. those who responded to this statement with agree or completely agree) between people with YOD who completed the survey and care partners who completed the survey on behalf of a person with YOD (χ2 = 0.32, df = 1, p = 0.57), those living within or outside a major city (χ2 = 0.01, df = 1, p = 0.91) or between those with AD and another type of YOD (χ2 = 0.84, df = 1, p = 0.36). There was also no impact of time from access request to plan approval on plan satisfaction (χ2 = 1.66, df = 3, p = 0.65). Fewer than 30% of respondents agreed that disability service providers understand dementia, or that finding a provider with whom to use their NDIS funds is easy. However, respondents more often endorsed disability providers as more capable of meeting their needs than aged care providers.
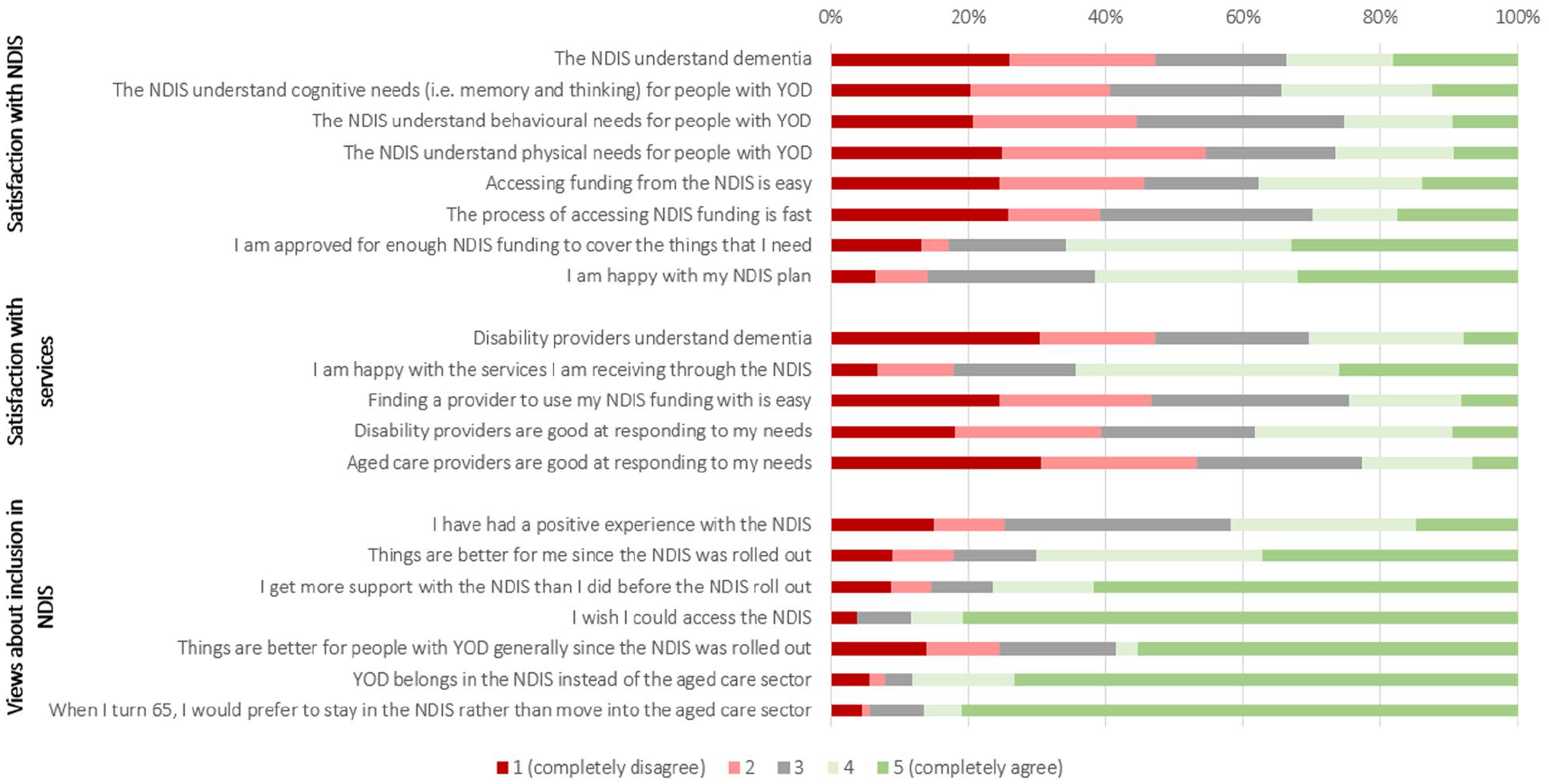
Overall sample satisfaction with the NDIS, disability services and NDIS eligibility in general (respondents with YOD and care partners pooled here).
Despite these relatively negative views of the NDIS and disability providers specifically, respondents remained overwhelmingly in favour of YOD services remaining in the disability system rather than in the aged care system. Most agreed that things were better for them personally (70%) and for people with YOD more generally (58%) since the NDIS roll-out and the move out of the aged care system. Almost all (87%) of those who were NDIS participants at the time of survey completion indicated that they would prefer to remain in the NDIS rather than move to aged care when they turn 65 years old.
Discussion
This study of 151 Australians with YOD and care partners is the first to examine their experiences and satisfaction with post-diagnosis care provision since the NDIS roll-out. In some ways, the results confirm what was suspected from anecdotal reports (Coleman, 2018; Neurological Alliance Australia, 2017) in that respondents noted concerns about the delivery of care by the NDIS and the disability sector as a whole. Our data suggest that NDIS applications for a small group of people with YOD are being rejected based on a lack of knowledge among assessors or because impairments are deemed insufficiently severe to meet the criteria for disability. Difficulty meeting the NDIS eligibility requirements has been documented by other groups including those with mild intellectual disability and psychosocial disability (Hamilton et al., 2020; O’Connor, 2014).
While difficulties accessing the NDIS were relatively uncommon in our sample, they do highlight a need for better awareness among NDIS assessors about the nature of dementia and the value of early intervention. The disability sector has historically had little experience with dementia, and YOD is rare relative to other conditions in the NDIS (Productivity Commission, 2017). Pre-planning support, in which the person with disability is guided to prepare for their access request and planning meeting, has been suggested as a potentially effective method to improve plan quality (Collings et al., 2019) and may also assist people with YOD and their care partners to gather high-quality evidence to support their application.
Nearly 30% of our participants waited longer than 6 months to receive an approved funding plan from the NDIS. Coupled with the median 2- to 3-year delay in diagnosis reported by our participants, this additional delay has important implications. Early access to intervention can slow the progression of cognitive and functional decline in people with dementia (Laver et al., 2016; Robinson et al., 2015). Whether early intervention is the responsibility of the health or disability sector remains unclear, especially considering that the most effective treatments for dementia are non-pharmacological and delivered by allied health professionals (access to which can be funded by either sector) (Laver et al., 2016). While the delivery of these treatments in the healthcare system is inconsistent and inequitable (Cations et al., 2019a; Low et al., 2020), people with YOD may not have timely access to them in the disability sector either. Even if one sector delivered early intervention well, the lack of integration between the health and disability sectors in Australia has been criticised such that people with YOD are vulnerable to falling through the gaps (Royal Commission into Violence Abuse Neglect Exploitation of People with Disability, 2020). Diagnosis of YOD is becoming more sophisticated with the identification of pre-symptomatic and early symptomatic biomarkers (Colom-Cadena et al., 2020) and will continue to occur earlier when relatively few impairments have developed. This will make it more difficult to meet NDIS eligibility criteria, emphasising the need for action to improve integration and/or clarify who does what and when. Improved transition between diagnostic and post-diagnostic care services has been highlighted as a priority for people with YOD and their families in many countries (e.g. 10) and appears to remain in need in Australia. Lack of care integration and yearly NDIS review practices also increase the risk that changing health needs will go undetected (Cations et al., 2019b; Neurological Alliance Australia, 2017). Efforts to improve the delivery of early intervention in either sector must therefore be complemented by system change to increase the integration of care (Chase et al., 2020; Draper et al., 2018).
Participants also noted that it remains difficult to find services with which to use their NDIS funding. This problem has persisted over time, across countries (Kerpershoek et al., 2020; Stamou et al., 2020), and was a key barrier to service access in Australia when YOD was managed in the aged care system (Cations et al., 2017). Delivery of tailored services for people with rare conditions is a perennial challenge (Castro et al., 2017), especially in Australia where the population of people with YOD is spread out across a large geographical area. Disability providers may encounter very few people with YOD (if any) each year, reducing the imperative to stay abreast of best-practice recommendations for their care. Innovative approaches to address this issue are needed, for example, examining the potential value of tele-support and training, local ‘champions’ or hybrid services co-funded and delivered by aged care and disability service providers (Castro et al., 2017). In addition, an advisory ‘key worker’ programme was available for Australians with YOD from 2013 to 2019, which provided navigational support that was highly valued where it was used (Westera and Fildes, 2016). The discontinuation of this service leaves people with YOD with little support to traverse complex, intersecting systems and access the support that they need. Renewed efforts are required to address this gap in cost-effective ways.
Despite these concerns about the delivery of services under the NDIS, participants remained overwhelmingly positive about their inclusion in the NDIS and their desire for YOD to remain managed in the disability sector. These results may suggest that, overall, people with YOD and their care partners support the conceptualisation of dementia as a disability and favour the individualised, goal-directed funding model of the NDIS over the deficit model that dominates in aged care. A recent study demonstrated that people with mild to moderate severity YOD have a relatively sophisticated understanding of the relationship between dementia and disability, and feel they should have access to rehabilitation services to promote their social and community participation. Older participants who also had mild to moderate symptoms of dementia were more ambivalent about these concepts (Laver et al., 2020). This may signal the onset of generational changes in the way that dementia is conceptualised and treated, supported by the recent international emergence of propositions for the adoption of a social or relational model approach to dementia care based on disability theory (Shakespeare et al., 2019; Swaffer, 2015; Vernooij-Dassen et al., 2021).
However, it is also possible that the preference for YOD to remain in the disability sector reflects a relative dissatisfaction or concern with the aged care sector. A Royal Commission into Aged Care Quality and Safety was occurring at the time of data collection for this project, which was scathing in its assessment of the aged care sector (Royal Commission into Aged Care Quality and Safety, 2019) and generated significant negative media attention. More research is needed to understand whether our participants’ relative preference for the NDIS reflects their own understanding of the disability framework and sense that dementia sits within this, a preference for the funding model offered by the NDIS, a rejection of themselves as ‘aged’ or a specific fear of or aversion to aged care.
Strengths and limitations
This is the largest ever survey of Australians with YOD and their care partners, and the first research to examine their experiences with the NDIS so far. The sample includes a wide range of dementia types, and the survey allowed us to gain a comprehensive picture of experience with the NDIS so far and potential points of dissatisfaction.
The limitations of this work include the use of an online platform for data collection. This introduces a sampling bias in favour of people with YOD with milder cognitive impairments, and both people with YOD and care partners with better digital literacy and fewer employment and familial responsibilities. Selection bias may also have been introduced by our advertising the study only selected in multi-disciplinary memory clinics. Our sample also did not include any people with YOD and few care partners of people with YOD living in supported accommodation or residential aged care. This is a unique group whose experience with the NDIS (and aged care) is likely to differ from those living in the community; future research should examine their experiences with disability care and its intersections with aged care. We also had insufficient data from dyads (e.g. people with YOD and their care partners together) to make meaningful intra-dyad comparisons here. Each member of the dyad is likely to have separate priorities and experiences, requiring individual responses. Including dyads also allows for dual perspectives to be provided including those of people with severe cognitive and/or functional impairments. Future research addressing this research gap will be important.
Our survey did not collect information about whether service use was dictated by lack of access, lack of uptake or both. Consistent with Andersen’s model of healthcare utilisation, previous research with people with YOD and their care partners has demonstrated that the extent to which an accessible service is used is mediated by the perception that the service will meet the person’s needs (Kerpershoek et al., 2020). This pattern has also been demonstrated in an Australian sample of people with YOD prior to NDIS roll-out (Cations et al., 2017). Analysis of the patterns of service within the NDIS framework will allow for deeper understanding of how accessibility and uptake interact in this new system.
Another limitation was the absence of Aboriginal or Torres Strait Islander Australians from our sample, despite this group having very high rates of YOD relative to non-Indigenous groups (LoGiudice et al., 2015; Radford et al., 2015). This likely reflects our failure (and lack of resources available) to conduct extensive consultation with the communities. This work is important especially given that socio-economic marginalisation, culturally inappropriate services and systemic racism can impact NDIS participation and satisfaction among Aboriginal and Torres Strait Islander people with other disabilities (Stephens et al., 2014; Townsend et al., 2018). Recent research has also demonstrated that older Aboriginal and Torres Strait Islander people prefer to access aged and health services designed with their cultural needs in mind (Larke et al., 2020). Understanding the experiences of those with YOD and the unique barriers to best-practice care encountered by this group is important for guiding appropriate service design and delivery.
Finally, the use of a cross-sectional design limits our ability to examine how experiences and satisfaction with the NDIS may change over time. The NDIS is still a relatively young scheme, and the disability sectors’ experience with dementia will grow with time. The progression of cognitive and functional impairment will also necessitate changes to formal supports with time, and most people with YOD will age over 65 years with their condition. Future longitudinal research should examine how these factors impact the suitability and acceptability of social care for people with YOD and their families and seek to understand whether the perceived benefits of staying outside of the aged care sector continue over time.
Conclusion
This study has demonstrated that people with YOD and their care partners are overwhelmingly satisfied with their inclusion in the NDIS. However, participants continue to encounter the barriers to accessing best-practice care that historically also occurred in the aged care sector. Our data indicate that key areas for improvement include knowledge and understanding of YOD among NDIS staff and disability providers, faster access to funding after application and increased accessibility of tailored services with whom to spend funding. Future research to examine strategies for tailored disability care provision where a condition is rare and encountered infrequently by a disability provider will be helpful for addressing these remaining gaps. In addition, research is needed to better understand the experiences of groups facing intersecting marginalisation, including people with YOD living in residential aged care or supported disability accommodation, and Aboriginal and Torres Strait Islander people living with YOD. The outbreak of the coronavirus disease 2019 (COVID-19) during and after data collection for this survey is also likely to have affected service access and experiences in important ways. Research examining the impacts of COVID-19 for people with YOD and their care partners will be important for establishing the tailored response required for this group.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211011699 – Supplemental material for Post-diagnosis young-onset dementia care in the National Disability Insurance Scheme
Supplemental material, sj-pdf-1-anp-10.1177_00048674211011699 for Post-diagnosis young-onset dementia care in the National Disability Insurance Scheme by Monica Cations, Sally Day, Kate Laver, Adrienne Withall and Brian Draper in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We would like to acknowledge the support of Ian Gladstone, Michael King and Sue King in completing this research, and Dementia Australia for their assistance with promotion.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.C. has been employed in the past 5 years to assist with data collection for Alzheimer’s disease drug trials funded by Janssen and Merck. All other authors declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Dementia Australia Research Foundation project grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.