
Abstract
Objective:
To investigate the accuracy of a diagnosis of pediatric bipolar disorder in the Danish National Register compared to the patient charts. Second, we reported on the occurrence of a diagnosis of pediatric bipolar disorder during the study period.
Methods:
All persons appearing in the Danish nationwide registers between 1995 and 2014 with an incident ICD-10 diagnosis of single hypomanic/manic episode or a diagnosis of bipolar disorder (summarized as bipolar disorder [BD]) before turning 18 years were identified (n = 521) and a random sample (n = 131) hereof was selected for chart review. Each chart was reviewed by two independent Schedules for Clinical Assessment in Neuropsychiatry (SCAN) certified raters to assess whether symptoms documented in the chart were consistent with a formal diagnosis of BD according to the ICD-10 criteria or not.
Results:
The formal diagnostic criteria for BD according to the ICD-10 were fulfilled in 48 charts (45.3%, 95% CI: [36.1%, 54.8%]) out of 106 reviewable charts, age at index = 16.4 ± 1.6 (range = 9.1–18.3) years. Cohen’s Kappa ranged from 94.4% to 100%. The estimate of a lifetime prevalence up till the current age for bipolar disorder for those of aged 5–18 years, was 0.019% in 2014.
Conclusion:
Less than half of the register-based pediatric BD diagnoses were confirmed by chart review, which was lower than expected. The occurrence of a register diagnosis of pediatric BD was relatively low.
Background
Bipolar disorder (BD) with onset in childhood or adolescence is referred to as pediatric bipolar disorder (PBD). PBD is associated with severe morbidity and interferes with normal development often causing malfunctioning in school and in relation to peers (Birmaher, 2013). Moreover, PBD is often associated with substance misuse, crime and suicidality (Birmaher, 2013).
The estimated prevalence of PBD is 1.8% based on a meta-analysis including studies of BD-I, BD-II and BD NOS in patients aged 7–21 years from 1985 to 2007 (n = 16,222; Van Meter et al., 2011). An updated meta-analysis of epidemiologic studies of PBD was published in 2019 by the same author group, using the same inclusion criteria but adding eight additional studies (total n = 56,103), concluded that the prevalence of PBD was stable over time (Van Meter et al., 2019). This result was based on seven studies from the United States and 12 studies from outside the United States, albeit earlier studies had reported increases in incidence of PBD in the United States in the period 1996–2004 (Blader and Carlson, 2007).
Studies have indicated that PBD is associated with high rates of psychiatric comorbidity, making it challenging to diagnose BD in youth (Biederman et al., 2004; Tillman et al., 2003), leading to both diagnostic and treatment delays (Egeland et al., 2000; Hirschfeld et al., 2003). Indeed, several symptoms of hypomania and mania overlap with those of attention-deficit/hyperactivity disorder (ADHD; Biederman et al., 2004; Grande et al., 2016; Soutullo et al., 2009), thus creating a diagnostic challenge and potential misclassification. In addition, there is still a potential risk of PBD being perceived as a controversial diagnosis resulting in potential underdiagnosing or misclassification as described by Malhi et al. (2020). Furthermore, various atypical presentations and attenuated forms of PBD may not be captured in the current classification systems, in particular in the ICD-10, for example, frequent mood shifts or subtle changes in behavior. This may result in lower rates of PBD diagnoses. Finally, the diagnostic delay often seen in patients eventually diagnosed with BD may be particularly pronounced in childhood and adolescence and may move patients from pediatric to adult onset BD.
The primary aim of the current study was to investigate the accuracy of the diagnosis PBD as registered in the Danish healthcare registers by comparing these diagnoses with those based on chart reviews, using a randomly selected sample of a nationwide cohort. Secondarily, we aimed at assessing the occurrence of PBD over the study period in the national Danish cohort.
Methods
Design
A Danish nationwide register- and chart-based study.
Registers and database program used
A unique person identification number called The Civil Person Registration number (CPR-number) is assigned to all Danish citizens upon birth or migration (Pedersen, 2011). Data on an individual can be linked across registers via the CPR-number.
Information about psychiatric diagnoses was retrieved from the Danish Psychiatric Central Research Register (DPCRR; Mors et al., 2011) and the Danish National Patient Register (NPR; Lynge et al., 2011) in order to identify those below age 18 years who had a BD diagnosis registered in the study period. Only hospitals are obligated to send information about diagnoses to the registers.
The secure online browser-based software solution Research Electronic Data Capture (REDCap) was used to collect the chart data added by the investigators (Harris et al., 2009).
Study population
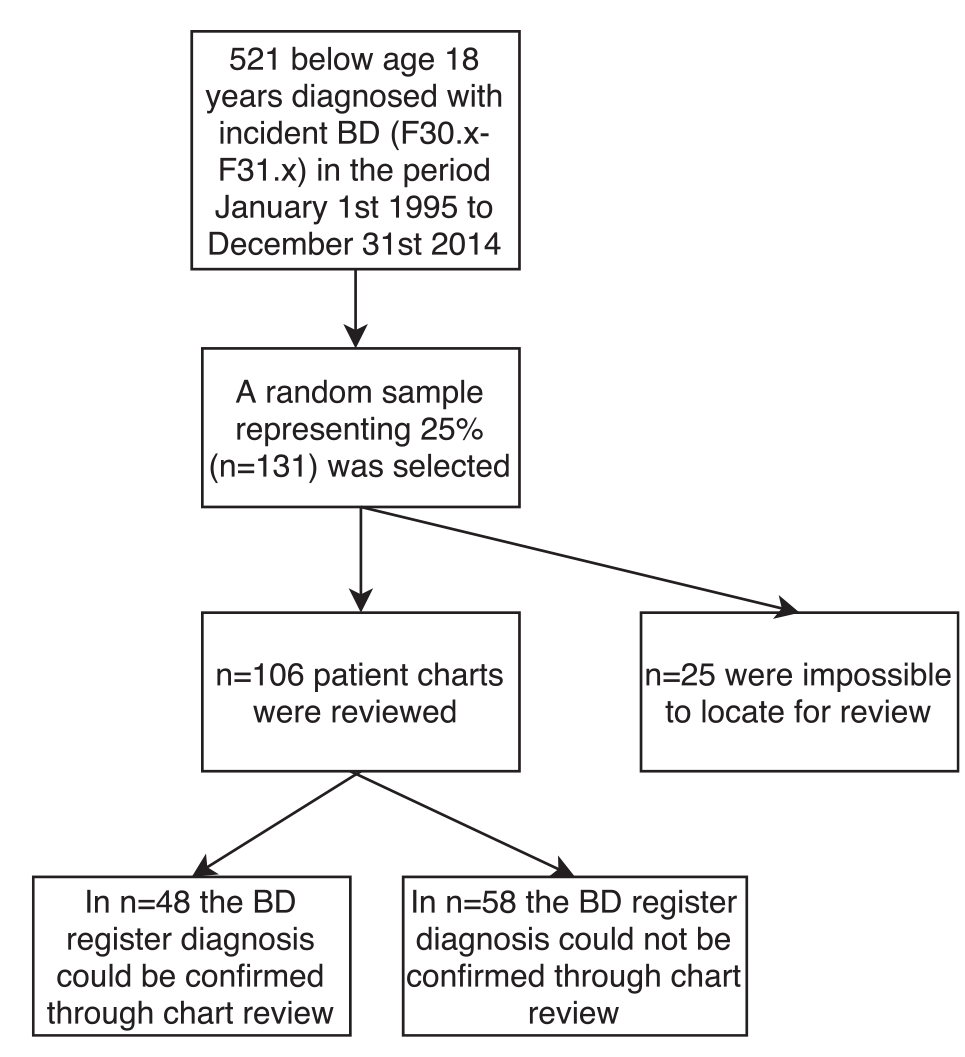
All children and adolescents below 18 years of age at the time of a first-ever ICD-10 single hypomanic/manic episode or BD (ICD-10 F30.X or F31.X, in the following summarized as BD) (World Health Organization, 1992) registered in the NPR (Lynge et al., 2011) between 1 January 1995 and 31 December 2014 (Figure 1) were included.
Sample description.
The random sample and the rating process
The Danish Data Health Authorities provided CPR-numbers of all persons in the study population together with a date corresponding to the start of the contact leading to the first BD register-diagnosis. A sample was randomly shuffled by a computer using Stata (StataCorp, 2015), and the first 131 CPR-numbers, consisting of 25% of the cases, were selected, representing all cases. The charts from the random sample were retrieved with assistance from relevant psychiatric departments from all over Denmark.
The selected charts were reviewed for diagnostic purposes by one Schedules for Clinical Assessment in Neuropsychiatry (SCAN; World Health Organization, Division of Mental Health, 1994) certified psychiatric specialist (either fifth author, A.K.P. or sixth author, R.E.N.). Each chart was also independently reviewed by a second SCAN certified (World Health Organization, Division of Mental Health, 1994) resident (the first author, M.F.L.) for diagnostic purposes. The raters collected information on symptoms described at the episode leading to the first BD register-diagnosis (the index episode) and at previous episodes, if any. The information was systematically entered into REDCap (Supplemental Appendix 1). After listing symptoms from the index and representative previous episodes, if any, the raters rated the presence of the BD diagnosis in the respective chart as ‘yes’, ‘very likely’, ‘not likely’, or ‘no’. When the BD diagnosis was categorized as ‘yes’ or ‘very likely’, the diagnostic accuracy was considered established.
‘Yes’ was used when all criteria for the BD diagnosis were fulfilled according to the ICD-10.
‘Very likely’ was used when almost all criteria for the BD diagnosis were fulfilled, for example, the number of symptoms was almost sufficient to fulfill the BD diagnosis, but some symptoms were perhaps less than adequately described, or the duration of symptoms almost fulfilled diagnostic criteria.
‘Not likely’ was used when the chart stated a BD diagnosis with either an insufficient number of symptoms or too short symptom duration to fulfill the time criteria according to ICD-10.
‘No’ was used when there were no symptoms in the chart describing a hypomanic or manic episode or when it was clear to the rater that there was a registration mistake.
All raters used the ICD-10 Classification of Mental and Behavioral Disorders Diagnostic criteria for research as the reference (World Health Organization, 1993) and used the SCAN glossary (World Health Organization, Division of Mental Health, 1994) as the reference for each diagnostic criterion. If the two independent raters disagreed on whether the final diagnosis reported in the chart was concurrent according to the ICD-10 criteria, both raters discussed their point of view until consensus was reached. The ICD-10 BD diagnosis appearing in the register is, in principle, also based on the ICD-10 Classification of Mental and Behavioral Disorders Diagnostic criteria for research, as this is the official version for routine clinical use in Denmark, albeit in a Danish translation.
Descriptive variables identified from charts
Mood symptoms
Presence of the following symptoms of depression and hypomania/mania was identified from the charts prior to and/or during the episode leading to the first BD register-diagnosis: (1) Depressed mood, (2) Decrease in energy, (3) Decrease in self-esteem, (4) Hypersomnia, (5) Irritability, (6) Distractibility, (7) Insomnia, (8) Eating less, (9) Daily mood swings, (10) Eating more, (11) Restlessness, (12) Decreased need for sleep, (13) More talkative than usual, (14) Racing thoughts, (15) Elevated mood, (16) Reckless behavior, (17) Pressured speech, (18) Over-familiarity, (19) Grandiosity, (20) Spending sprees, (21) Increased sex drive, (22) Psychomotor retardation, (23) Psychomotor agitation, (24) Loss of normal social inhibitions, (25) Anhedonia/loss of pleasure, (26) Feelings of self-reproach, (27) Recurrent thoughts of death, (28) Diminished ability to concentrate and (29) Hyperactivity.
Age at first diagnosis
Age at first ICD-10 BD was calculated using the date of first BD chart-diagnosis and the date of birth retrieved from the CPR register (Pedersen, 2011).
Diagnostic instrument
The diagnostic instruments for BD considered were the Present State Examination (PSE) (Cooper, 1985) and the Kiddie Schedules for Affective Disorders or Schizophrenia (K-SADS) (Kaufman et al., 1997).
Diagnostic setting
The diagnoses could be established in the following settings: (1) outpatient hospital-based settings or (2) during hospitalization.
Substance abuse
Positive information on substance abuse (including one or more of the following: alcohol, cannabis, or other drugs) was registered as present or not.
Statistical analyses
Kappa statistic was used to test interrater reliability.
All categorical variables are presented as percentages with total numbers while the continuous variables are presented as means with standard deviations.
To investigate the representability of the randomly selected subsample compared to the remaining sample, we compared the distribution of sex, year of diagnosis and substance use disorder, using chi-square test and Fishers’ exact test where appropriate. Comparison of mean age at index register-diagnosis between the two groups was performed using a t-test.
To investigate the similarity of the patients with a confirmed BD diagnosis and the patients without a confirmed BD diagnosis, we compared the distribution of sex, diagnostic setting, substance use disorder and whether diagnostic interview was conducted or not, using chi-square test and Fishers’ exact test where appropriate. Comparison of mean age at index register-diagnosis between the two groups was performed using a t-test.
The proportion of incident BD cases for each year in the study period from the background population in the same year (incidence proportion) was computed. For each year, the background population used as the denominator comprised all persons in Denmark of age 5 up to below 18 years (Statistics Denmark, nd). The lifetime prevalence of bipolar disorder between 5 and 18 years of age was calculated for the year 2014. The number of individuals diagnosed with BD between 2001 and 2014 and who were still below 18 years in 2014 was divided by the size of the population between 5 and 18 years living in Denmark in 2014 (Statistics Denmark, nd).
These analyses were performed with Stata 14 (StataCorp, 2015). Results with p values <0.05 were considered statistically significant.
Ethics
The project was approved by the Danish Data Protection Agency (id-number 2015-79), the Danish Health Data Authority (FSEID-00002605) and the Danish Health Authority (id-number 3-3013-1470/1/), which authorized the use of the CPR-numbers.
Data were stored and treated according to current laws and regulations, and there is no material that can identify an individual in the database. Utilizing chart-based data, required no informed consent by the local clinical ethics committee.
Results
The total sample from the NPR comprised 521 children and adolescents with a register-based ICD-10 diagnosis of BD. From the random sample of 25.0% (n = 131) patients, we retrieved 106 patient charts with sufficient material to investigate whether symptoms listed in the charts matched the BD register-diagnosis (Figure 1).
There were no statistically significant differences regarding demographic characteristics between the 106 patients whose charts were reviewed and the remaining sample, whose charts were not reviewed (data not shown).
In 48 patients (45.3%, 95% CI: [36.1%, 54.8%]) of the 106 rated, the ICD-10 BD register-diagnosis could be confirmed based on the symptoms listed in the charts.
Demographic and clinical characteristics for the 48 children and adolescents with a confirmed BD diagnosis and for the 58 with a diagnosis of BD which could not be confirmed are shown in Table 1. The average age at the episode leading to the index BD register-diagnosis was 16.4 ± 1.6 (range: 9.1–18.3) years, only 2 were a couple of months older than 18 years at BD diagnosis, but the psychiatric contact leading to index BD register-diagnosis was initiated before age 18 years, while 2 other were diagnosed before age 13 years. Half of the patients were females. A semi-structured diagnostic instrument (PSE or K-SADS) was used for 37.5%, and 62.5% were diagnosed during hospitalization.
Demographic and clinical characteristics of the patients with a registered incident bipolar disorder diagnosis between 1 January 1995 and 31 December 2014 whose chart was reviewed (n = 106).
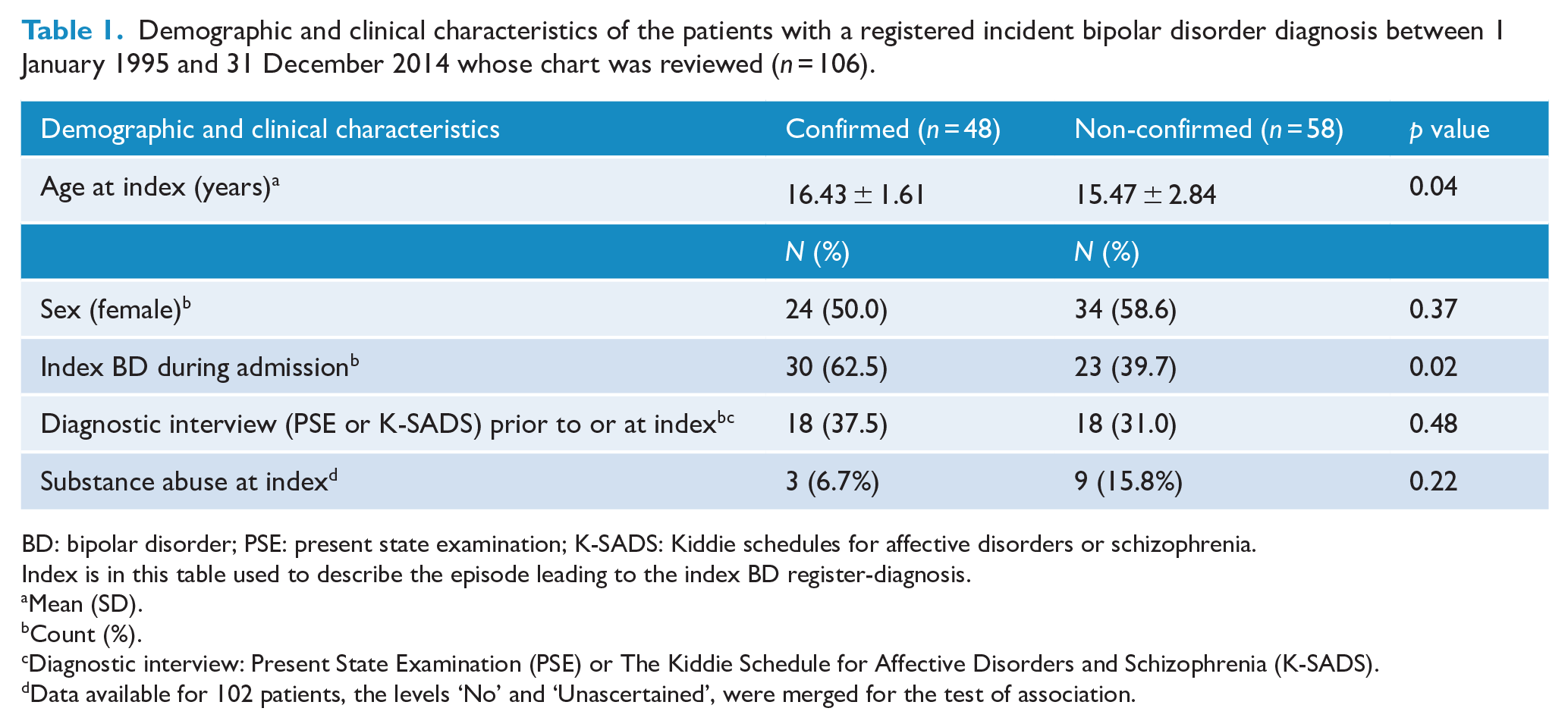
BD: bipolar disorder; PSE: present state examination; K-SADS: Kiddie schedules for affective disorders or schizophrenia.
Index is in this table used to describe the episode leading to the index BD register-diagnosis.
Mean (SD).
Count (%).
Diagnostic interview: Present State Examination (PSE) or The Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS).
Data available for 102 patients, the levels ‘No’ and ‘Unascertained’, were merged for the test of association.
The mean age at the episode leading to the index BD register-diagnosis for the 58 patients with a non-confirmed BD diagnosis was 15.5 ± 2.8 years and 58.6% were female. Semi-structured diagnostic instruments were used in 31.0% of the cases, and 39.7% of them received their diagnosis during hospitalization. When comparing the 48 patients with an ICD-10 chart-based confirmed BD diagnosis to the 58 patients without an ICD-10 chart-based confirmed BD diagnosis we found a statistically significant difference in diagnostic setting, where the majority of the patients with a confirmed BD diagnosis were diagnosed during inpatient hospitalization and not in outpatient settings whereas the opposite was true for the patients without a confirmed BD diagnosis. Likewise, the difference in age between the patients with a confirmed BD diagnosis and the patients without a confirmed BD diagnosis showed to be statistically significant, with patients with a confirmed BD diagnosis being almost 1 year older on average at time of index BD register-diagnosis.
The annual incidence proportion of BD during the study period is displayed in Figure 2 showing an increasing trend. As migration in and out of Denmark is very low and only very few die in this age group, this incidence proportion roughly reflects an incidence rate. The lifetime prevalence in 2014 for those between 5 and 18 years was 0.019%.
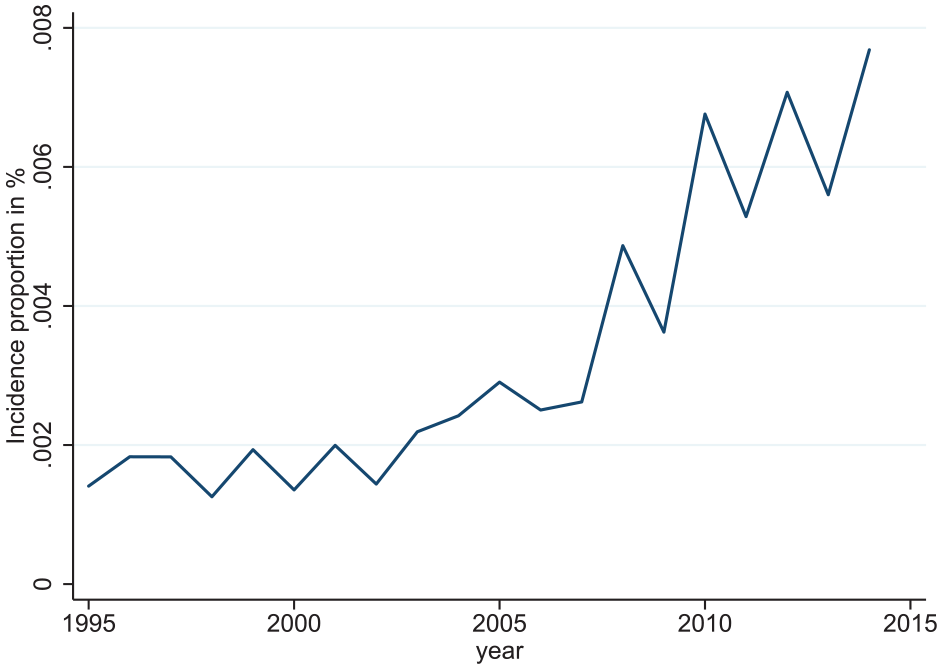
Incidence proportion.
There was a high degree of inter-rater reliability. First and sixth authors: Kappa: 0.887 (95% CI: [0.792, 0.983]); 94.4% agreement in 90 observations. First and fifth authors: Kappa: 1.0 (95% CI: [1.0, 1.0)]; 100% agreement in 16 observations.
Discussion
In a random sample of 131 patients taken from a nationwide Danish cohort of children and adolescents with a register-based ICD-10 diagnosis of BD, 106 had an accessible and reviewable chart, and diagnostic accuracy between register-based and chart-based diagnosis was reached for 48 patients (45.3%, 95% CI: [36.1%, 54.8%]). This finding is lower than observed for adult schizophrenia in which 97.5% were seen as valid (Uggerby et al., 2013) and lower than observed for pediatric schizophrenia in which 75.3% were seen as valid (Vernal et al., 2018).
As found for the accurate diagnosis of youth diagnosed with schizophrenia in the Danish registers (Vernal et al., 2018), we found that an inpatient diagnosis was more common among the 48 patients with a confirmed BD diagnosis. It is likely that inpatient clinicians had more time to spend on the diagnostic process and that psychopathologic features were described in more depth during inpatient hospitalizations as a result of continuous observation by several healthcare professionals. The relatively low diagnostic accuracy between register-based and chart-based diagnosis could thereby also partly be due to inadequately documented symptoms, particularly in the charts in outpatient settings, where clinicians do not monitor patient symptoms continuously, but rely on retrospective information provided by patients and their caregivers.
The mean age at diagnosis was higher in the group with a confirmed BD diagnosis than in the group with unconfirmed diagnosis. This finding might be a result of lower age being associated with poorer report of symptoms and of lower age being associated with symptoms being milder or less characteristic for BD, thus not meeting the full criteria for an ICD-10 diagnosis of BD. Similar results have been found for less specific symptoms of attenuated and suprathreshold psychosis in younger children and adolescents (Gerstenberg et al., 2016; Kelleher et al., 2012).
Furthermore, patients with a subtle presentation of PBD, for example, patients with repeated hypomanic episodes of less than 4 days duration, will not be diagnosed with BD applying the ICD-10, which is used in Denmark, whereas in countries where the DSM is used like in the United States, a diagnosis of BD NOS may be given. Such differences in the classification systems might explain some of the difference between the incidence of BD in Denmark versus the United States.
Also, the common use of SCAN as a diagnostic tool in clinical practice in Denmark may increase the threshold for the diagnosis of BD, which leads to patients with only attenuated symptoms of BD not being diagnosed with BD, and thereby not being represented in the registers.
As to the secondary aim of our study, the incidence proportion of BD in patients below age 18 years increased throughout the study period. However, when interpreting this part of our results, the poor diagnostic accuracy should be born in mind.
As to the observed, relatively poor diagnostic accuracy of the register-based diagnoses in our study, this discordance between diagnoses made as part of clinical practice and diagnoses in the context of research has been described before (Goodman et al., 2000; Reich, 2000), and according to a meta-analysis (Rettew et al., 2009), there is only a modest level of diagnostic agreement between routine clinical evaluation and the standardized diagnostic interview. Thus, in a study of 120 adolescents inpatients clinically diagnosed with mania, most patients did not meet the strict DSM criteria for a manic episode when evaluated using a standardized clinical interview (Pogge et al., 2001). The possibility that some symptoms used by the clinicians for the diagnosis of BD in children and adolescents were not recorded in the charts should also be noted.
The estimate of a lifetime prevalence for bipolar disorder for those of aged 5–18 years was 0.019% in 2014. Despite the potential cases with a false positive diagnosis of PBD among our total sample of 521 patients with a register-based diagnosis of PBD, this prevalence rate is lower than expected, based on the estimated lifetime prevalence of bipolar disorder in children and adolescents in a meta-analysis by Van Meter et al. (2011; prevalence of bipolar spectrum disorder: 1.8%) and in a study by Merikangas et al. (2010) reporting on prevalence of BD in 10,123 13–18 years old obtained through a face-to-face survey (lifetime prevalence of BD type I and II: 2.9%). However, the results cannot be directly compared due to difference in study designs and sample selection.
In the current study, we used a selected sample of patients diagnosed with BD in hospital based settings, whereas the study by Merikangas et al. (2010) was based on surveys from a representative part of the general population in which the prevalence of detected mental illness would most likely be higher. Using surveys for data collection allows for identification of mental disorders which might never reach hospital-based psychiatry, either due to lack of illness awareness, or because less severe cases may be well compensated for or accepted by the parents (and the child/adolescent), or because the patients are diagnosed and followed by private child and adolescent psychiatrists. Furthermore, the study by Merikangas et al. (2010) used a sample of patients from 13 up till 18 years of age, which yield a higher proportion of persons with mental disorders than younger age groups, which were included in the present study. Moreover, as we only investigated patients with a first time BD register diagnosis, we were not able to address the issue of false negatives, which would have required assessment of a much larger sample of charts, which was not feasible and beyond the scope of the present study. Cultural differences in referring and diagnosing children and adolescents in Denmark compared to the United States could possibly partly explain why a 40-fold increase in incidence of pediatric onset bipolar disorder occurring in the United States from 1996 to 2004 has not been observed in Denmark (Blader and Carlson, 2007).
Our reported estimates of the occurrence of register based BD should be interpreted cautiously due to our finding of a relatively poor diagnostic concurrency of these diagnoses.
Strengths and limitations
The main strength of the current study was the use of a randomly selected sample of a nationwide cohort of children and adolescents with incident BD over a 20-year time period. The register-based diagnosis provided during clinical routine was carefully re-evaluated by our team in which there was a high degree of inter-rater diagnostic reliability, with all discrepancies being solved by discussion and consensus. In the current design, we were unable to undertake a full clinical examination including a diagnostic interview, which would have been the golden standard to validate diagnoses. With the low incidence of pediatric BD, we chose to use chart review to investigate symptoms described in patients diagnosed with pediatric BD. Furthermore, the study did not investigate false negatives, which would have been a possibility if the authors had chosen to investigate a random sample of patients diagnosed with other psychiatric disorder potentially mimicking pediatric BD, for example, ADHD or depression. This might be investigated in future studies. Finally, the ICD-10 does not differentiate between BD-I and BD-II. Therefore, BD was not categorized by subtypes in the current study, although it would have been relevant, as BD-I might be misclassified less often than BD-II.
The Danish healthcare system is free of charge, and it therefore includes all patients independently of socioeconomic status and geographic location if treatment is sought, resulting in a relatively unselected nationwide sample. However, the generalizability of our findings is limited by the fact that only patients diagnosed at hospital-based settings, which report continuously to the Danish healthcare register, are included in the registers. Therefore, less severely ill patients, for example, treated by general practitioners and private psychiatrists, are not represented in the registers.
The generalizability of our findings could also be compromised by failure of case identification in clinical practice, either in the primary sector or when the patients are evaluated in the hospital-based setting. However, this is a general limitation of the Danish registers. BD is particularly challenging to diagnose when patients only present mild mood episodes or symptoms and are below 18 years.
Taken together, the true occurrence of BD in persons below 18 years in Denmark is likely higher than the occurrence reported here.
Conclusion
This study demonstrated a relatively poor accuracy of the register-based PBD diagnosis, which could be due to a nonsystematic clinical documentation practice rather than actual low occurrence. Nevertheless, this finding underscores the need for a more systematic diagnostic approach and for a longitudinal observation of children and adolescents when diagnosing PBD. These findings are important when interpreting research conducted on register BD diagnoses in patients below 18 years, including our own reported estimated occurrence of PBD.
Supplemental Material
sj-pdf-1-anp-10.1177_00048674211009622 – Supplemental material for Occurrence and accuracy of a register-based diagnosis of pediatric bipolar disorder: A nationwide cohort study
Supplemental material, sj-pdf-1-anp-10.1177_00048674211009622 for Occurrence and accuracy of a register-based diagnosis of pediatric bipolar disorder: A nationwide cohort study by Mathilde Frahm Laursen, Christoph U Correll, Rasmus W Licht, Maria Rodrigo-Domingo, Anne Katrine Pagsberg and René Ernst Nielsen in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
Thanks to Tobias Kallehauge, who provided help with data management.
Thanks to Simon Grøntved for helping with presenting data graphically
Author Contributions
M.F.L., R.E.N., R.W.L. and M.R.-D. drafted the manuscript. M.F.L., A.K.P., R.E.N. and M.R.-D., analyzed the patient data. M.F.L., R.E.N. and M.R.-D. interpreted the data. R.E.N., R.W.L., A.K.P., M.R.-D. and C.U.C. revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: M.R.-D. has reported no biomedical financial interests or potential conflicts of interest. A.K.B. has reported no biomedical financial interests or potential conflicts of interest. M.F.L. has received speaking fees from Lundbeck. R.E.N has received research grants from H. Lundbeck and Otsuka Pharmaceuticals for clinical trials, received speaking fees from Bristol-Myers Squibb, Astra Zeneca, Janssen & Cilag, Lundbeck, Servier, Otsuka Pharmaceuticals, Teva and Eli Lilly and has acted as advisor to Astra Zeneca, Eli Lilly, Lundbeck, Otsuka Pharmaceuticals, Takeda and Medivir. C.U.C. has been a consultant and/or advisor to or has received honoraria from: Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Indivior, IntraCellular Therapies, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Medscape, Merck, Mylan, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Servier, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva. He provided expert testimony for Janssen and Otsuka. He served on a Data Safety Monitoring Board for Lundbeck, Rovi, Supernus and Teva. He has received grant support from Janssen and Takeda. He is also a stock option holder of LB Pharma. R.W.L. has within the preceding 3 years served an advisory board of Janssen-Cilag and SAGE and has received speaker honorarium from Astra-Zeneca, Janssen-Cilag, Servier and Lundbeck.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the Unit for Psychiatric Research, Psychiatry, Aalborg University Hospital, Aalborg, Denmark and Department of Clinical Medicine, Aalborg University Hospital, Aalborg, Denmark.
Availability of Data and Material
The datasets used and analyzed during the current study are only available after permission obtained from the Danish Health Data Authorities, the Danish Patient Safety Authority and Statistics Denmark.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.