
Abstract
Background and Aims:
Police and paramedics play a crucial role in responding to suicide crises in the community. However, little is known about the nature, extent, precipitating factors, pathways and outcomes of a suicide-related call to emergency services and what responses will most effectively and compassionately meet the needs of those in crisis. Partners in Prevention: Understanding and Enhancing First Responses to Suicide Crisis Situations (PiP) was established to address these knowledge gaps.
Methods:
This article describes (1) the methodology used to construct the PiP dataset, a population-wide linked dataset that investigates the characteristics and health pathways of individuals in Queensland who were the subject of a suicide-related call to police or paramedics; and (2) preliminary findings on service demand, demographics and health services utilisation.
Results:
We identified 219,164 suicide-related calls to Queensland Police Service or Queensland Ambulance Service that were made over the 3-year period 1 February 2014 to 31 January 2017. A total of 70,893 individuals were identifiable via records linkage. The cohort linked to more than 7,000,000 health records. We estimated that police or paramedics in Queensland received on average 209 calls per day, with increases year on year over the study period. Analysis of demographic data highlighted the heterogeneous nature of this cohort and important demographic variations between individuals in contact with police versus ambulance services.
Discussion:
The PiP dataset provides a strong foundation for a multi-modal dataset that can be built on over time, both cross-sectionally and longitudinally. Further linkages to Medicare Benefits Schedule, Pharmaceutical Benefits Scheme and social care datasets are planned.
Conclusion:
Detailed population-level analysis that data linkage can provide is critical to improving understanding and responses to suicide crisis situations. The PiP study is a world first and provides a unique opportunity to improve responses to this public health problem.
Introduction
Suicide and suicidality are highly distressing events with wide-ranging impacts on the individual, their family, carers, friends, responders and the community. Police and paramedics are frequently the first to respond to people experiencing suicide crises (World Health Organization, 2009). While there is a growing evidence base to inform police and paramedic responses to individuals with mental illness, there is a paucity of research that focuses on suicidality, including self-harm, specifically (Crilly et al., 2019a, 2019b; Lubman et al., 2019; Parker et al., 2018; Puntis et al., 2018). In particular, limited evidence is available to help inform improvements in, and around, the crucial ‘touch point’ between police, paramedic, mental health and related services (Meurk et al., 2020a; 2020b). There is an imperative need to overcome this knowledge gap and develop an evidence base that is specific to suicidality, informs care pathways and helps to inform our understanding of the intersections and differences between suicidality and mental disorder (Hjelmeland, 2011; Hjelmeland and Knizek, 2017; Phillips, 2010).
Partners in Prevention: Understanding and Enhancing First Responses to Suicide Crisis Situations (PiP) is a large Queensland-based multi-stakeholder initiative, comprising police, ambulance and health services, along with primary health networks, the community-based mental health sector, Queensland Mental Health Commission, research organisations and a lived experience organisation. PiP has sought to develop a holistic and comprehensive evidence base through a multi-component research project, comprising literature reviews; service mapping; mixed-methods study of the knowledge, skills, attitudes and confidence of police in responding to suicide crisis situations; and consultation with individuals with lived experience of suicide, about what constitutes an optimal first response (Meurk et al., 2020a). In addition, this project resulted in the establishment of a unique linked dataset. The Partners in Prevention–linked dataset provides a globally unique multi-modal dataset, designed to be extended over time in a way that supports multiple types of analysis (Meurk et al., 2020b). The dataset has been developed to find answers to questions about the extent of demand that suicide-related calls place on police and ambulance services; the demographic and health characteristics of individuals who are the subject of a suicide-related call to police and ambulance services; the temporal aspects of health services contacts; and outcomes following a suicide-related call.
The aim of this article is to describe the construction of the Partners in Prevention–linked dataset, its preliminary findings and identify future opportunities to expand this resource.
Method
Governance
The study was approved by the Royal Brisbane and Women’s Hospital Health Research Ethics Committee (HREC/17/QRBW/666) and the Queensland Police Service (QPS) research committee (DOC17/1772716). Health data was released under Queensland’s Public Health Act (RD007342). The principle of separation was strictly followed to protect individual privacy. This entailed separating identifying data from content data through engagement of a mediating agency (Statistical Services Branch, Department of Health [Qld]).
Study setting
The setting for this study is the state of Queensland, Australia. Queensland spans an area of 1.853 million km2 and encompasses 16 Hospital and Health Services districts, 15 corresponding Local Ambulance Service Networks (LASN) and 15 QPS districts that are geographically offset to the health and ambulance districts. In 2017, the estimated Queensland population was 4.9 million. From 2014 to 2017, the population in Queensland grew by approximately 4.38%; the majority of the population resides in the Southeast corner of the state.
Study overview
The study cohort was identified via identification of a set of suicide-related calls for service to QPS and Queensland Ambulance Service (QAS), and these data linked to a variety of state-wide data sources. An overview of this process is provided in Figure 1.
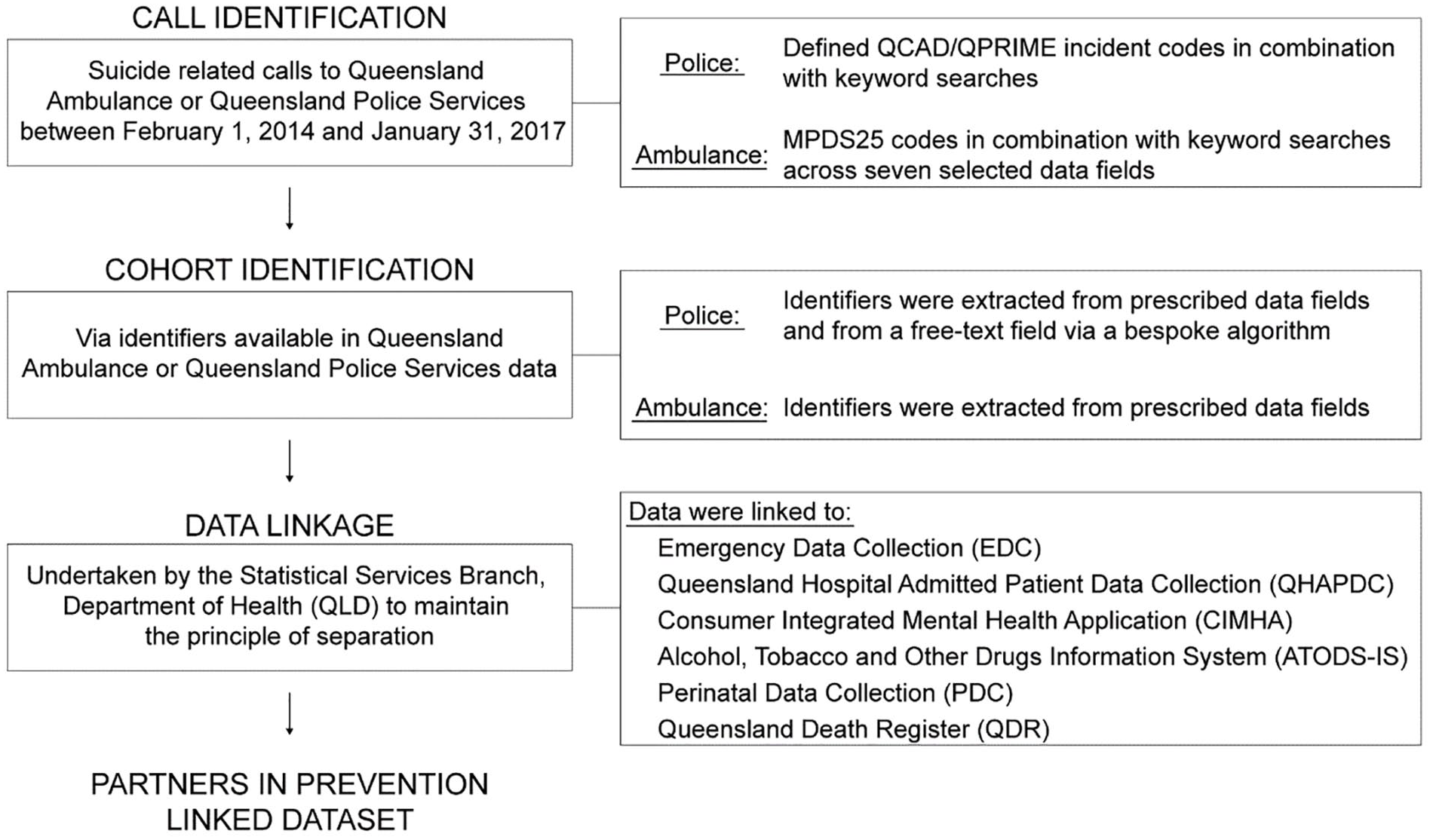
Schematic of the data linkage process.
Call identification
For this study, a suicide crisis was defined as a documented instance or account of suicidal ideation, threatened suicide, threatened intentional self-harm, intentional self-harm, suicide behaviours and suicide attempts. A suicide death was a documented instance or account of first responder attendance to a suicide death. A suicide-related call to emergency services was a call to emergency services that was initially or subsequently determined to be suicide related, as identified in QAS and/or QPS records. A suicide-related call included calls that were classified as a suicide crisis or a suicide death. Suicide-related calls to police were identified via the QPS computer-aided dispatch (QCAD) and Queensland Police Records Information Management Exchange (QPRIME) databases. Suicide-related calls to ambulance were identified via the QAS computer-aided dispatch (CAD) and electronic Ambulance Report Form (eARF).
Suicide-related calls to QAS
For QAS, all CAD records classified as MPDS25 (‘Psychiatric, Abnormal Behaviour/Suicide Attempt’) were included. Additional cases were identified through suicide-related keyword searches across seven selected data fields in eARF. The selection of ambulance records is summarised in Figure 2.
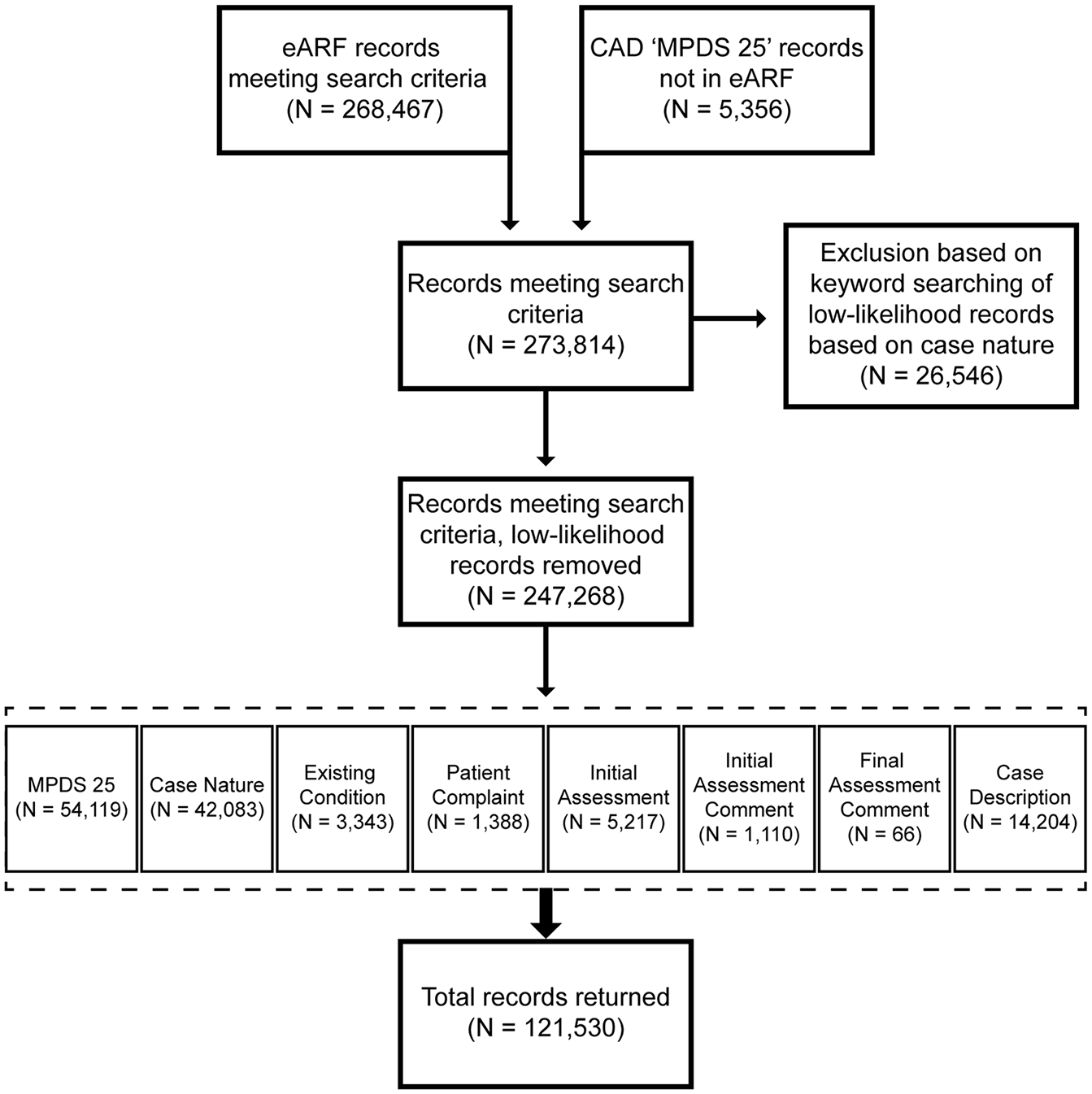
Flowchart showing selection of calls from QAS records.
Suicide-related calls to QPS
Calls to QPS were included if they had an initial or revised QCAD dispatch code of 502 (‘Suicide’) or 503 (‘Attempting/Threatening Suicide’). In addition, dispatch codes considered to be potentially suicide related, namely 312 (‘Domestic Violence’), 313 (‘Disturbance/Disputes’), 504 (‘Mentally Ill Person’), 513 (‘QAS’), 610 (‘Community Assistance’) and 619 (‘Welfare Check’), were searched for suicide-related keywords. This was informed by our review of dispatches identified in previous service evaluations (Queensland Forensic Mental Health Service, 2016), expert advice from police collaborators and inductively. A keyword list was developed iteratively, based on manual review of dispatch records, and included common misspellings, grammatical errors and abbreviations. Keywords were selected with a view to reducing false positives in calls identified. The process of manual review identified that keywords were context specific to dispatch codes, resulting in a high rate of false positives for some keyword by dispatch combinations that were excluded post hoc (Supplementary File 1). Figure 3 summarises the selection of QPS records.
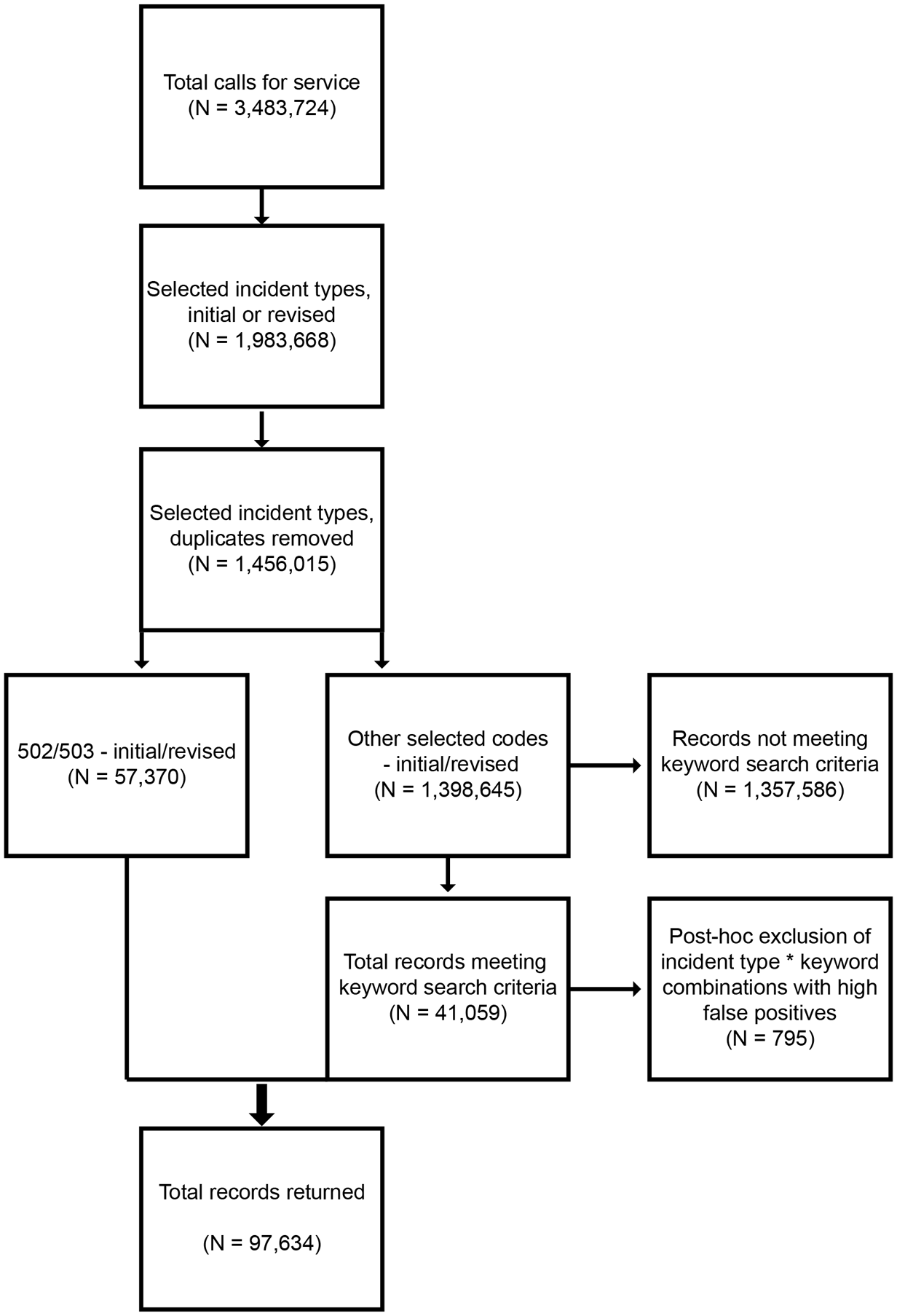
Flowchart showing selection of calls from QPS records.
Cohort identification
The cohort for this study encompasses individuals who were the subject of a suicide-related call to QAS or QPS between 1 February 2014 and 31 January 2017. Identifiers were extracted from detail fields of QAS records, while for QPS records, identifiers were extracted from detail fields of QPRIME records, but via a bespoke algorithm that extracted identifiers from free-text data for QPS QCAD records (Supplementary File 2).
Data linkage
Data linkage was undertaken by the Statistical Services Branch (Department of Health, [Qld]) in accordance with the Queensland Data Linkage Framework (Department of Health, 2016). QAS records and the QPS QPRIME extract for individuals whose death was recorded as ‘sudden death – suicide’ were linked deterministically as well as probabilistically on first name, surname and date of birth using the LinkageWiz software (www.linkagewiz.net/index.htm). The remainder of QPS QPRIME-identified records and QCAD records were matched deterministically on first name, surname and date of birth. Linkage was facilitated via a Master Linkage File (www.health.qld.gov.au/hsu/link/datasets) which contains information on individuals for frequently requested data. All linkage underwent quality assurance checks to ensure compliance with privacy protocols and data quality.
Extracted identifiers were linked to the Emergency Data Collection (EDC); the Queensland Hospital Admitted Patient Data Collection (QHAPDC); the Consumer Integrated Mental Health Application (CIMHA) database; the Alcohol, Tobacco and Other Drugs Information System (ATODS-IS) database; the Perinatal Data Collection (PDC); and the Queensland Death Register (QDR). Each of these datasets provide information on a range of demographic and socioeconomic variables, as well as the frequency and nature of health services contacts. Linkage was undertaken for the period spanning 1 February 2013 to 31 January 2018. This period was selected to ensure that data for at least 1 year before and after the first call to QAS or QPS was available for analysis.
Linked datasets
QAS records
Content data provided by QAS included the date and time when information about an incident was received, the LASN and postcode of the incident, the dispatch priority level, the destination facility the individual was transported to, the case nature, the initial and final assessment along with assessment comments, and the date of birth, gender, and ethnicity of the individual.
QPS records
Content data provided by QPS included the date and time of the incident as well as the date and time when the call was received, the call source, the police district, postcode and statistical area codes of the incident, initial and revised codes, and the dispatch priority level. In addition, QPRIME-linked records provided information on gender and age.
EDC
The Queensland EDC holds records of all presentations to Queensland hospital emergency departments. Content data from the EDC includes information on individual demographics, triage category, mode of presentation, diagnoses (International Classification of Diseases, 10th Revision [ICD-10]) and the end status of the service episode.
QHAPDC
The QHAPDC contains data on admitted patients within the state of Queensland, both public and licensed private facilities. Content data for this study includes demographic and clinical information, diagnoses (ICD-10) and other features associated with health services contact (e.g. length of stay).
CIMHA
The CIMHA is a platform for recording information relating to public mental health services contacts within Queensland. Content data provided for this study includes information on demographics and socioeconomic status, presenting problems and referral source, diagnoses, intervention type and admissions under Queensland’s Mental Health Act.
ATODS-IS
The ATODS-IS holds records on consumers in contact with public alcohol and other drugs services in Queensland. Content data provided for this study includes information on demographics, drugs of concern and intervention type.
PDC
The PDC collects information on live births and stillbirths occurring at or after 20 weeks gestation and/or at least 400 g in weight in Queensland. Information accessed includes demographic and clinical information relating to the mother and her child, including the date of birth of the child and number of birth events per mother.
QDR
The QDR, administered by the Queensland Government, records all deaths within Queensland. Information collected includes the date of death, and the underlying and contributing cause of death codes according to the International Classification of Diseases.
Analysis
This article reports on data from 69,451 individuals drawn from the total cohort of 70,893 individuals for whom linkage was complete. Records were excluded for individuals identified within QPRIME whose death was recorded as ‘sudden death – suicide’, but where a call-for-service record could not be identified. This group included individuals who died outside of the period within which the cohort was defined (i.e. 1 February 2017–31 January 2018); individuals where the call source was identified as being a CAD call source, but specific incident details could not be found; and individuals for whom there appeared to be no CAD dispatch (including counter drop-ins, police call-ins and PoliceLink calls not routed to CAD). A total of 1442 records were excluded. Analyses were conducted using R (R Core Team, 2019).
Demand
Call centres in QPS districts Capricornia, Ipswich, Mackay and North West were not upgraded to the QPS QCAD system for part of the study period, leading to an underreporting of incoming calls in these areas. Thus, the number of QPS calls was imputed from the data, based on population estimates of those districts. Estimates for QPS calls were derived separately for the overall study period and per year.
Demographic data
Demographic data were measured per individual as follows:
Sex was measured based on the mode of all sex values (Male, Female).
Aboriginal and/or Torres Strait Islander status was assigned if there was at least one record for an individual that identified them as Aboriginal and/or Torres Strait Islander (Thompson et al., 2012).
Age was measured based on an individual’s age at their index suicide-related contact with QAS or QPS. Where two or more ages were provided for the same year, the lowest age was chosen.
Country of birth was identified based on the mode of all country of birth values.
A new or expectant mother was defined as someone who had delivered a baby in the same calendar year, or the calendar year before or after their first contact with police or ambulance services.
Descriptive statistics were calculated out of the number of known values. The percentage of missing values across all demographic variables ranged from 0.3% to 4%. Inferential statistics were used to examine demographic differences between individuals who were the subject of a QAS or QPS response. Differences in proportions were assessed using Pearson’s chi-square test using the prop.test base R function. The Wilcoxon rank-sum test was used to compare age data, which was non-normally distributed, using the wilcox_test and wilcox_effsize functions embedded within the rstatix package (Kassambara, 2020). Results were considered statistically significant if p < 0.05.
Results
In total, we identified 219,164 suicide-related calls for service (QAS, 121,530 and QPS, 97,634) over the 3-year study period (2014–2017). From these calls, 70,893 individuals were identifiable via record linkage of which 69,451 linked to a police or ambulance dispatch. There was an increase in suicide-related calls of approximately 28% for calls to police and 23% to paramedics over the study period.
Demand
After adjusting for missing data, we estimated that there were 228,549 calls for service over the 3-year study period (1096 days). This amounted to an average of 209 calls per day (QAS, 111 and QPS, 98). Table 1 shows the estimated average daily calls per year, over the study period. After adjustment, the increase in suicide-related call becomes more alike across services (21% increase for QPS and a 23% increase for QAS).
Estimated average daily calls to QAS and QPS per year and percentage of change over the study period.
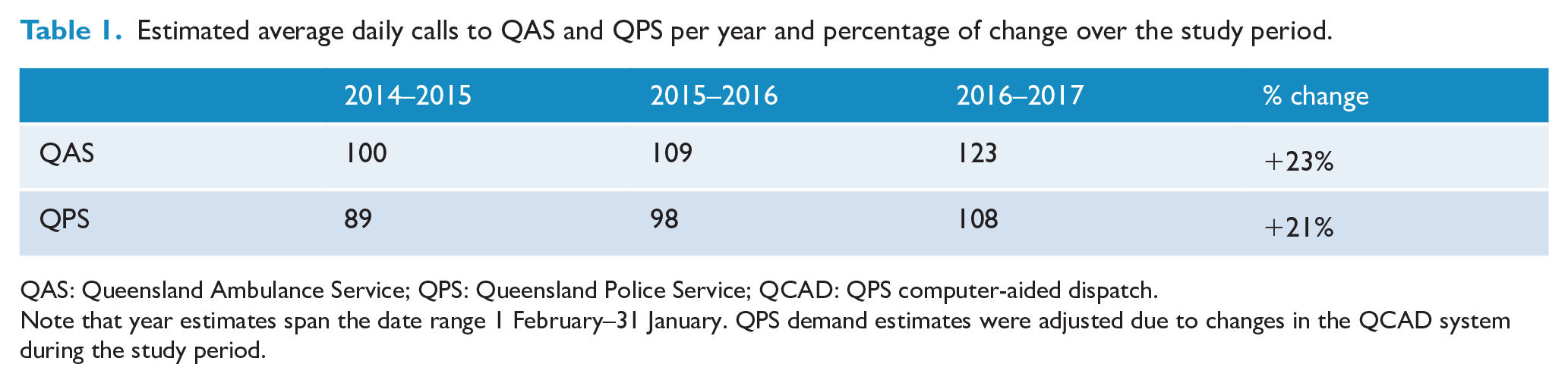
QAS: Queensland Ambulance Service; QPS: Queensland Police Service; QCAD: QPS computer-aided dispatch.
Note that year estimates span the date range 1 February–31 January. QPS demand estimates were adjusted due to changes in the QCAD system during the study period.
Cohort
Contact with QAS or QPS
Most individuals were identified via QAS records. Approximately 89% of individuals in the cohort had an identified contact with QAS, 22% had an identified contact with QPS and 11% had an identified contact with both QAS and QPS. This discrepancy between the number of individuals identified via QPS and QAS databases is attributable to differences in recording identifying information by the respective agencies, necessary for linkage, and should not be interpreted as a prevalence estimate.
Demographic characteristics
Fifty-two percent of the cohort were female. The gender distribution was significantly different for individuals who had a contact with QAS versus QPS (χ2 = 687.47, df = 1, p < 0.0001). Specifically, more than half of the individuals (54%) who came into contact with QAS were female, while more than half of individuals (58%) who came into contact with QPS were male. Of those who had contact with both services, 54% of the individuals were male and 46% female.
The median age of the cohort was 33 years (interquartile range [IQR] = 22–47 years), 11% were below the age of 18 years at the time of their index contact with QPS or QAS and 8% were 65 years or older at the time of their index contact with police or paramedics. Individuals who came into contact with QAS were older overall, with a median age of 33 years (IQR = 22–48 years), than individuals who came into contact with QPS, who had a median age of 32 years (IQR = 22–43 years). This difference was statistically significant; however, the effect size of this difference was small (r = 0.03, p < 0.0001). Table 2 provides summary statistics by gender and service type.
Median age in years, with interquartile range, by gender and service type, and summary Wilcoxon rank-sum test statistics.
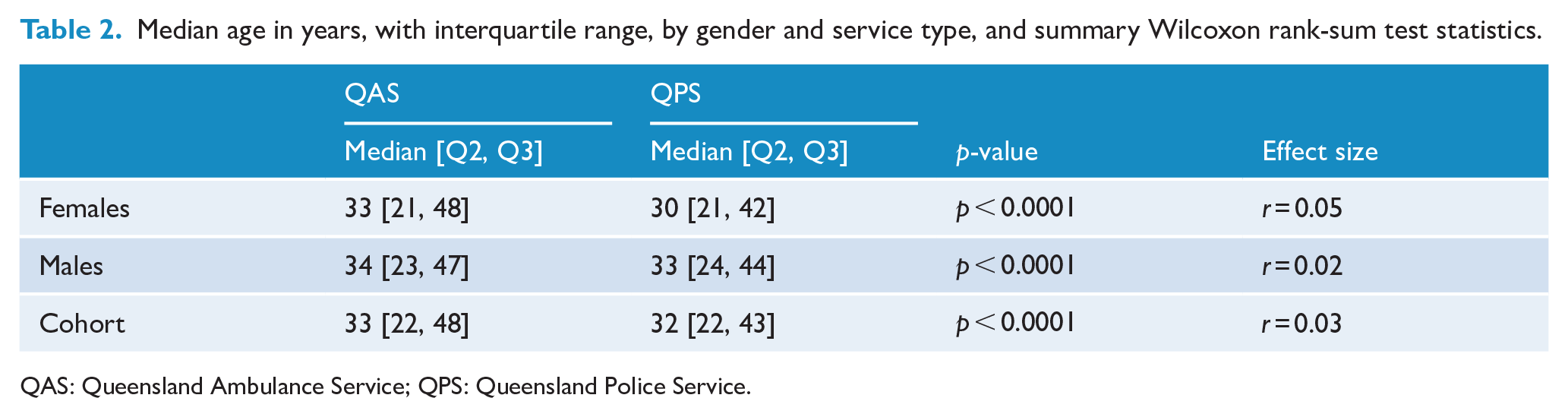
QAS: Queensland Ambulance Service; QPS: Queensland Police Service.
Most of the individuals in the cohort were born in Australia (84%), and 16% were born overseas. The percentage of Aboriginal and/or Torres Strait Islander individuals identified as having a contact with QAS was 12%, lower than the percentage of Aboriginal and/or Torres Strait Islander individuals identified as having a QPS contact (15%). This difference was statistically significant (χ2 = 69.56, df = 1, p < 0.0001).
Health services contacts
Table 3 summarises health services contacts. Overall, nearly all individuals within the cohort had an emergency department contact (96%). Similarly, the majority of individuals had a recorded hospital admission or contact with public mental health services (84% in both cases). Eighteen percent had a record in the ATODS-IS database and approximately 14% of all females over the age of 10 within the cohort (i.e. 7% of the entire cohort) had given birth over the period 1 February 2013 to 31 January 2018.
Health services contacts for the cohort as ascertained via EDC, QHAPDC, CIMHA and ATODS-IS databases, and the PDC.
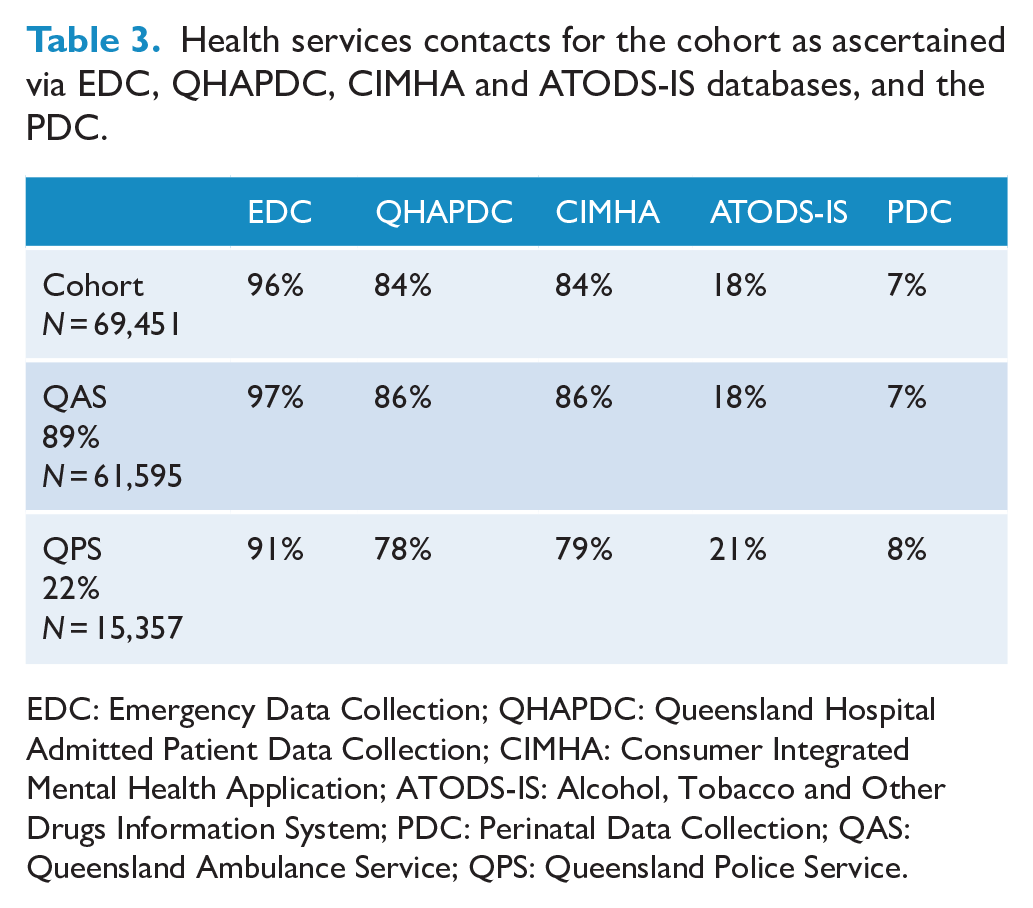
EDC: Emergency Data Collection; QHAPDC: Queensland Hospital Admitted Patient Data Collection; CIMHA: Consumer Integrated Mental Health Application; ATODS-IS: Alcohol, Tobacco and Other Drugs Information System; PDC: Perinatal Data Collection; QAS: Queensland Ambulance Service; QPS: Queensland Police Service.
Data describing health services utilisation before and after the index contact with QAS or QPS for the cohort are summarised in Table 4. Notably, the combined number of health services records (EDC, QHAPDC, CIMHA, PDC and ATODS-IS) increased in the year following the index call to QAS or QPS in comparison to the same period before the index event. The number of records peaked on the day of the first call to QPS or QAS for the QHAPDC and EDC, and an increase in service provision for mental health (CIMHA) and alcohol and other drugs services (ATODS-IS) was evident in the week following the index event.
Health services contacts and death registrations over the study period.
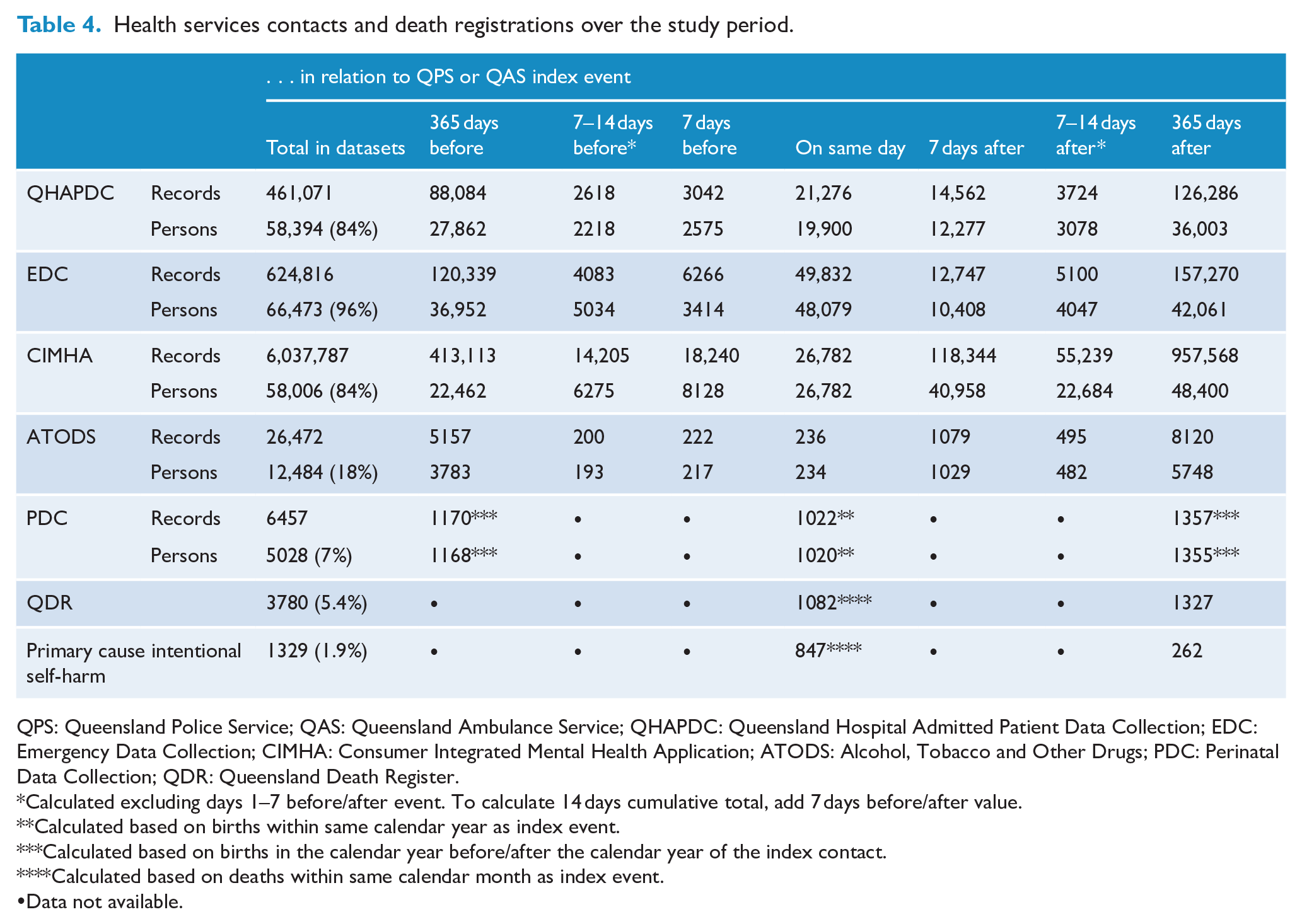
QPS: Queensland Police Service; QAS: Queensland Ambulance Service; QHAPDC: Queensland Hospital Admitted Patient Data Collection; EDC: Emergency Data Collection; CIMHA: Consumer Integrated Mental Health Application; ATODS: Alcohol, Tobacco and Other Drugs; PDC: Perinatal Data Collection; QDR: Queensland Death Register.
Calculated excluding days 1–7 before/after event. To calculate 14 days cumulative total, add 7 days before/after value.
Calculated based on births within same calendar year as index event.
Calculated based on births in the calendar year before/after the calendar year of the index contact.
Calculated based on deaths within same calendar month as index event.
Data not available.
Deaths
Overall, 5.4% of the individuals in the cohort died within the study period. Specifically, 1.9% of the cohort died, where the identified cause was due to intentional self-harm (ICD-10 codes X60-84; World Health Organization, 2004), while 3.5% died due to a cause other than intentional self-harm (i.e. 35% of deaths were recorded as deaths due to intentional self-harm).
Discussion
The evidence base to inform police and paramedic responses to suicide crisis situations has been lacking. Given the significant impact of suicidality on the community, it is incumbent upon health professionals and researchers to develop a comprehensive evidence base to inform responses. To the best of our knowledge, this is the first study to quantify and characterise the nature of suicide-related calls to police and paramedics (Meurk et al., 2020b).
This study uncovered the extraordinary, and increasing, frequency of suicide-related calls made to QAS and QPS in Queensland. Through linkage, it was possible to profile the demographic and health characteristics of individuals at the time of their crisis and their subsequent health services utilisation and outcomes, in ways that have not previously been possible. In particular, producing a demographic profile of individuals who were the subject of a police response was made possible, for the first time, through linkage.
Differences in age and gender distribution, as well as variation in prevalence of individuals of Aboriginal and/or Torres Strait Islander background who had a QAS versus QPS, were all statistically significant. Notable findings were the high proportion of Aboriginal and Torres Strait Islander people who had a suicide-related contact with police versus paramedics, and the variation in gender distribution across the services. However, the effect size of age differences between services was small, even when disaggregated by gender. Further investigations are warranted into age distributions of sub-populations within the cohort, such as those under the age of 18. The unexpectedly high number of women who were the subject of a suicide-related call and who gave birth in or around the time of this contact also warrant closer investigation. Records for 1442 individuals who were suspected to have died by suicide, but for whom no call-for-service to QAS or QPS could be identified, are also an important sub-group, as this cohort may differ from the overall cohort.
Implications for policy and practice
Suicide-related contact with police or paramedics reflect both an ‘outcome’ and an ‘intervention’. Considered as an outcome, the growing demand on police and paramedics suggests gaps in preventive responses. Indeed, contact with health services increased across the board following an index police or paramedic contact, indicating the crucial interventional role that police and paramedics play in facilitating contact with health services for individuals in need. However, the high rates of transportation to emergency departments identified indicate substantial opportunities for system redesign, based on alternative, including non-clinical, pathways tailored to heterogeneous needs. Recent reports published by the Australian Government Productivity Commission (2019) and Australasian College for Emergency Medicine (2018; Duggan et al., 2020) are consistent with the perspectives of those with lived experience, in identifying that emergency departments are inappropriate therapeutic environments for many of those who experience crisis (Queensland Forensic Mental Health Service Metro North Hospital and Health Service and Queensland Centre for Mental Health Research, 2020). The Partners in Prevention dataset provides opportunities for further examination of pathways, including pathways through and across hospital services, mental health services and primary care, as well as to evaluate the impact of implementing new service types (such as safe haven cafes and crisis care units) in reducing emergency department visits and improving outcomes.
Strengths and limitations
Identifying suicidal behaviours, particularly in non-health records such as those of police, is challenging, as is identification across service types (e.g. police and ambulance) in ways that are meaningfully comparable. As with much routinely collected data, records created by these agencies serve the purposes of facilitating their roles; for police and ambulance services, these roles are to preserve life and public safety, and provide effective provision of lifesaving treatment in an emergency situation, respectively. Nevertheless, ascertaining cases via systems designed for emergency responsiveness presents a key opportunity for understanding the temporal variation that characterises suicidality, and to fill in a much needed gap in understanding suicidal behaviours (that can often abate before or during a presentation to an emergency department) at the point of crisis. Understanding the profile of those who have contact with police and paramedics, together, is also advantageous to efforts to maximise diversion of vulnerable individuals who experience crisis from criminal justice pathways to health or therapeutic pathways instead.
The strength of this research was that we were able to confidently establish a cohort that we believe captured the majority of individuals who were the subject of a suicide-related call to police or paramedics over the period examined. We achieved this by using a number of different variables and methods for identification. The state-wide cohort provides a unique opportunity to examine suicidality across an entire Australian jurisdiction with a uniquely large cohort for this type of study. In addition, having data on suicidality as well as suicide death means that we can not only identify demographic and health-related correlates of suicide death, but also comprehensively build the evidence base for the much greater number of individuals who experience suicidal crisis that does not result in death.
The research was strengthened by its lived experience involvement. In particular, the data linkage study was shaped by lived experience consultants in the analysis and interpretation of findings, including implications arising. The data linkage study also facilitated lived experience engagement, by identifying the extent of need, and providing findings that could form the basis of collaborative discussion with first responders. In practice, these collaborative discussions had unforeseen benefits, in terms of identifying opportunities for training and service redesign.
The key limitations of this study include the following: first, infractions on case ascertainment relating to the incorrect initial or revised classification in QAS or QPS codes or notes not made, even where responders may have been concerned that a person in their care may have experienced a suicide crisis. Use of keyword searches for indicated codes and other fields mitigated this limitation by identifying cases that may not have been given an explicit suicide dispatch code (e.g. police welfare checks); second, identifying data could not be ascertained for all suicide-related calls to QAS and QPS. This is due to the structure of police and ambulance databases and the potential for a person in need to be unknown to the person who makes a call to emergency services and/or for the caller to fabricate personal details in some cases. The most significant limitation relates to identification of individuals via QPS records, which precluded our producing prevalence estimates at an individual level for the cohorts. Third, it was a condition of linkage that a QAS or QPS record matched at least one health service record (excluding CIMHA, which was matched at a subsequent step). Consequently, to be included in the dataset, an individual needed to have at least one health service contact over the period 2013–2018 or have a registered death between 2014 and 2018. The impact of these three limitations is the likelihood that our analysis will underestimate demand on first responders and fail to identify some persons who may have experienced suicide crisis. Nevertheless, the methodology used to identify individuals in QPS data is likely to be unbiased and thus is unlikely to impact on the validity of the profile of the cohort. Fourth, it was anticipated that individuals of Aboriginal and/or Torres Strait Islander descent would be overrepresented in the datasets. Yet, it was also expected that this overrepresentation may be an underestimate of the true extent of suicide crises among Aboriginal and Torres Strait Islander people, due to known failures to ask about and/or correctly record Aboriginal and/or Torres Strait Islander identity in the administrative datasets that were linked to, gaps in first response data and services to rural and remote locations, and discrimination-led mis-identification of suicidal crisis, particularly where substance use is a factor. We thus followed best practice for data linkage, which is to identify a person as Aboriginal and/or Torres Strait Islander based on a single confirmatory record (Thompson et al., 2012). Fifth, limitations in the reach of QAS and QPS mean that first responses to suicide crises in rural and remote locations will be incomplete. Sixth, administrative datasets being used in this study almost exclusively identify subjects by sex, which means a Male/Female designation. Consequently, it was not possible to examine variability relating to people who identify with diverse gender identities (information on sexual identity was also not available). Seventh, health services utilisation presents an incomplete picture of utilisation of private health and/or non-government organisation services. Data are presently limited to state-based health linkage; however, important information based on health services contact funded by Australia’s Medicare Benefits Schedule and prescribing through Australia’s Pharmaceutical Benefits Scheme will be forthcoming. Finally, this study examines one Australian jurisdiction and may not be representative of the national perspective. The National Ambulance Surveillance system initiative suggests that Queensland may have the highest rates of suicide-related presentations in Australia (Lubman et al., 2020).
Conclusion
Despite public health efforts and investment, suicidality remains a pressing public health issue. It is also an issue that impacts significantly on both emergency and health services. An examination of the nature of suicide-related calls to emergency services, and individual pathways and outcomes can inform understandings and the responses required. Partners in Prevention demonstrates a successful methodology for identifying individuals who are the subject of a suicide-related call to police or paramedics. This dataset provides a foundation for further data linkage and analysis. The cohort will soon be updated for a further 3 years, until 2020 (content data until 2021). This will enable longitudinal analysis, providing much needed evidence to inform and evaluate responses.
Supplemental Material
sj-docx-1-anp-10.1177_00048674211009604 – Supplemental material for Suicide crisis calls to emergency services: Cohort profile and findings from a data linkage study in Queensland, Australia
Supplemental material, sj-docx-1-anp-10.1177_00048674211009604 for Suicide crisis calls to emergency services: Cohort profile and findings from a data linkage study in Queensland, Australia by Carla Meurk, Lisa Wittenhagen, Emma Bosley, Megan L Steele, Denise Bunting, Elissa Waterson, Bronwen Edwards, Ben Martain and Ed Heffernan in Australian & New Zealand Journal of Psychiatry
Supplemental Material
sj-docx-2-anp-10.1177_00048674211009604 – Supplemental material for Suicide crisis calls to emergency services: Cohort profile and findings from a data linkage study in Queensland, Australia
Supplemental material, sj-docx-2-anp-10.1177_00048674211009604 for Suicide crisis calls to emergency services: Cohort profile and findings from a data linkage study in Queensland, Australia by Carla Meurk, Lisa Wittenhagen, Emma Bosley, Megan L Steele, Denise Bunting, Elissa Waterson, Bronwen Edwards, Ben Martain and Ed Heffernan in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to acknowledge the support and assistance from the Queensland Police Service and Queensland Ambulance Service in undertaking this research. The views expressed in this publication are not necessarily those of the Queensland Police Service or Queensland Ambulance Service and any errors of omission or commission are the responsibility of the authors. The authors would like to thank Dr Laura Ferris for her contribution to the definition of the study cohort. The authors would like to thank Jacinta Hawgood for her generous advice and suggestions for literature, included in this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the Partners in Prevention study was provided by the Suicide Prevention Health Taskforce, Queensland Health. C.M. and M.L.S. are employed by The Queensland Centre for Mental Health Research, which receives core funding from Queensland Health. E.H. is a recipient of an NHMRC Early Career Fellowship (APP 1162565).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.