
Abstract

Introduction
The Australian mental health system is weathering a deep crisis that places us at a critical juncture. The decisions to be made in the coming months could have adverse impact for decades. The Allison et al. (2020) paper tackles two critical issues in this process, though largely based on arguable premises: (a) the number of psychiatric hospital beds needed, and (b) the role of the National Mental Health Services Planning Framework (NMHSPF) as a planning tool for the public resourcing of mental health services.
Local estimates based on the Atlases of Integrated Mental Health Care (Romero-López-Alberca et al., 2019) partially support Allison’s claim. The number of acute beds in Western Europe is broadly similar to that in Australia, but the number of subacute and non-acute hospital beds and the number of community residential beds are fewer in Australia. However, there is a substantial difference between stating that ‘the total availability of non-acute psychiatric beds in Australia is lower than in country “X”’, and inferring from this that ‘psychiatric non-acute beds should be increased by N% in the health district “Y”’. Such national figures provide no useful indication of a local mental health system’s need for hospital beds or effective community alternatives.
The misuse of psychiatric beds as a sentinel health system indicator
Incredibly, there is no international agreed definition of ‘hospital’ (Montagni et al., 2018). While some hospitals do not have 24-hour medical coverage (similar to nursing homes), some community residential facilities provide full equivalents of hospital care. In Australia, ‘hospital in the home’ programmes are funded essentially as hospital-equivalent ‘non-admitted bed-based care’ but not counted as hospital beds, therefore falling outside length of stay (LOS) requirements for Activity Based Funding. The differences between provision of emergency, acute, subacute and non-acute beds vary across jurisdictions and patient groups (e.g. intellectual disabilities). Moreover, the activity of a facility may not be related to its official name – ‘subacute’ facilities often provide long-term care due to the lack of community provision.
This terminological conundrum extends to the definition of ‘hospital’ used by the Commonwealth Metadata (METeOR) glossary: ‘A health care facility established under Commonwealth, state, or territory legislation as a hospital … and authorised to provide treatment and/or care to patients’. This is actually a designation, not a definition.
The lack of standard units of analysis to facilitate like-for-like comparisons (non-commensurability) is a fundamental problem in real-world service planning (Romero-López-Alberca et al., 2019). Bed types and numbers referenced by Allison et al. do not allow meaningful international comparison, as countries may incorporate different service types when counting their bed provision.
A mental healthcare ecosystem approach
Local, state and national indicators can only be usefully understood within an interactive healthcare ecosystem approach (Rock and Cross, 2020; Rosen et al., 2020). Only using aggregate figures may lead to an ‘ecological fallacy’ (assuming population means and national averages apply directly to individuals or local services). Moreover, the risk of only using ‘average man’ indicators can also objectify language, treating persons as beds and acuity levels when their needs and preferences should be our ‘Pole Star’ (Rock and Cross, 2020).
Next, there is a tendency to disregard that health systems are complex and consequently non-linear, and context- and time-dependent. Minor changes in bed numbers in a ward, or losing one staff member in a community facility, may have unanticipated multiplier effects within the whole system and its key indicators such as hospital LOS.
Moreover, the use of enumerative indicators can lead to ‘surrogation’ (the tendency to replace the goal with its measure). For example, hospitals may substitute their ultimate goal (resolving a crisis in a short time frame) by a designated indicator such as bed availability or readmission rates. This risk is higher when the objective is vague, the metrics are concrete and conspicuous, and the establishment (including clinicians and managers) accepts the substitution.
The need for better decision-support systems for mental health planning
We agree with Allison et al that the algorithm underpinning the NMHSPF should be available for scrutiny, and that epidemiologically based models are insufficient on their own for estimating the number of beds for a given population. NMHSPF summary documentation, core algorithm and layers of its system architecture should be available to enable the development of alignment and communication (i.e. interoperability) with other tools. Providing meaningful access to key elements of NMHSPF is the best strategy to encourage engagement, development and innovation, as we need to build on and improve the framework we have. The restrictions to core NMHSPF documents mean arguments and decisions about if and how to use the planning framework are based on who makes them, which groups they seem to support and little else. Even taking into account this limitation, Allison’s tacit dismissal of the participation of experts in the development of NMHSPF as just ‘opinion’ disregards the relevance of expert and experiential knowledge in decision-support systems. A healthcare ecosystems approach formalises expert input as essential to develop decision-support tools (Rosen et al., 2020), and NMHSPF is based on extensive consultation with mental health domain experts, including clinicians.
Contrary to Allison’s claim, the sophistication of the NMHSPF places it several orders above translating Organisation for Economic Co-operation and Development (OECD) and World Health Organization (WHO) bed rates to planning and bed allocation. However, the value of using NMHSPF can be enhanced by the use of additional tools to drive planning. For example, NSW Health Mental Health Workforce Plan 2018–2022 has recognised NMHSPF as ‘one of a range of resources that could be used for mental health service planning’ (1.1.3, p. 102). In 2017, the WA Primary Health Alliance commissioned a study that analysed the combined use of NMHSPF and Description and Evaluation of Services and DirectoriEs (DESDE), an international classification system enabling bottom-up comparison of actual local service provision across regions and countries (Romero-López-Alberca et al., 2019). The study demonstrated synergies in using both systems for commissioning services, but again is not publicly available.
Complementary characteristics of these two tools for guiding decision-making are shown in Table 1.
Comparison of tools for the standard typification of services in Australia: DESDE-LTC and NMHSPF.
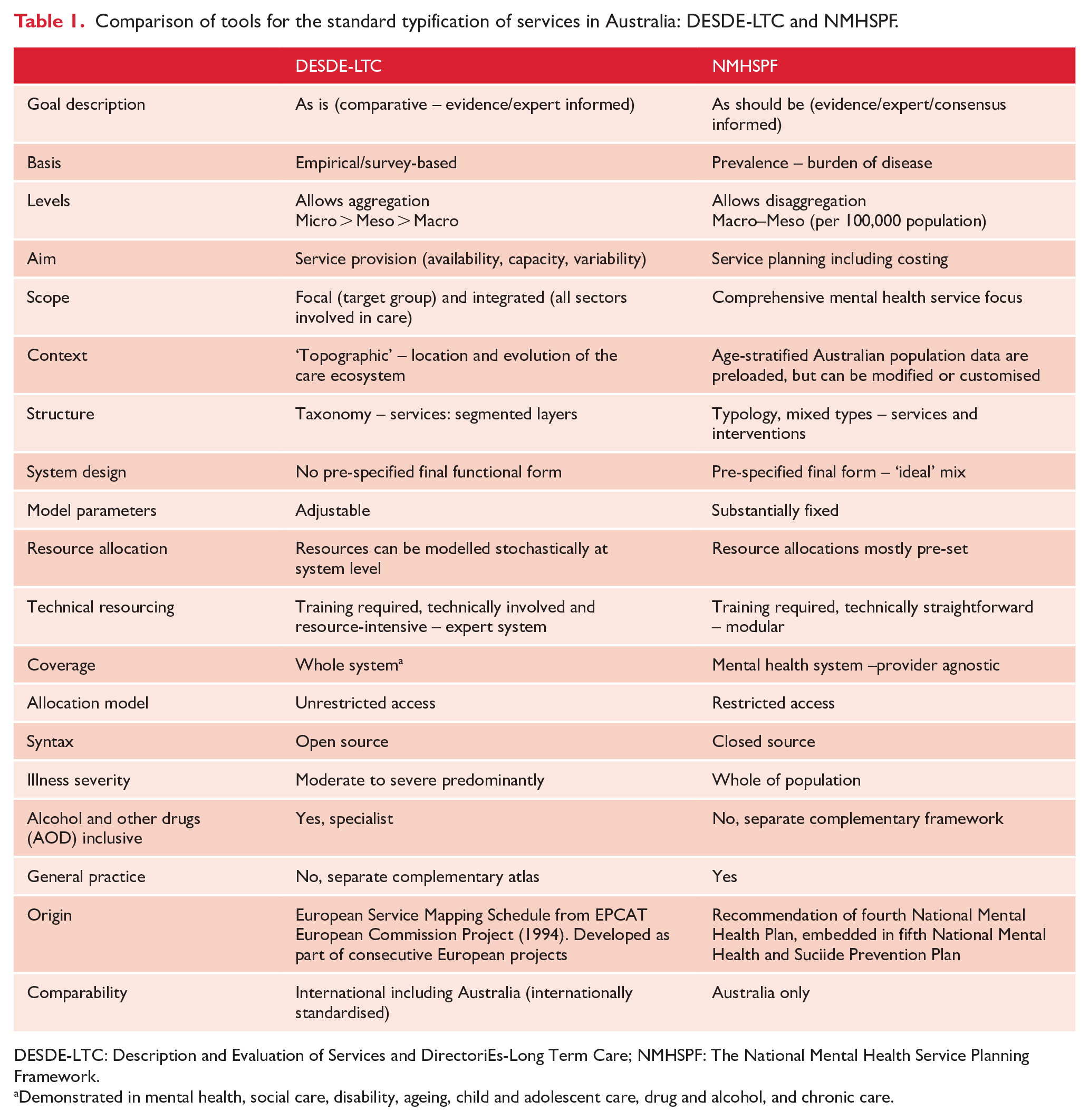
DESDE-LTC: Description and Evaluation of Services and DirectoriEs-Long Term Care; NMHSPF: The National Mental Health Service Planning Framework.
Demonstrated in mental health, social care, disability, ageing, child and adolescent care, drug and alcohol, and chronic care.
Conclusion
Over a century ago, Sigmund Freud’s The Interpretation of Dreams sparked a debate on the difference between scientific knowledge and other forms of inquiry. Ironically, substituting beds for dreams leads us over similar terrain. We refute the premises underpinning Allison’s arguments and advocate returning to a discussion grounded in scientific evidence to inform policy. The total number of hospital beds is an unreliable indicator for mental health planning due to non-commensurability bias, terminological variability, ecological fallacy, risk of surrogation and objectification. Bed numbers should be interconnected with other indicators in a healthcare ecosystem. A rational, scientific and humane approach to planning requires transparency, a common language and systematised domain expert input. The discourse on bed numbers misses the need to move past the current polarisation to the original purpose of the NMHSPF, to close the gap between the population need for care and current levels and types of provision. The summative lesson learned from more than four decades of evidence-based community care is the importance of appropriate balance between person-centred care in the community and inpatient services and resources. It is not a matter of hospital versus community, but both, with the balance determined on the basis of a transparent process that incorporates evidence, complexity variables and broad expertise of service providers, researchers and individuals, and families with living experience of mental disorders.
Footnotes
Acknowledgements
Our thanks for advice from Professors H. Killaspy, C. Harvey and P. McGorry, and Research Fellows Dr J Salinas and Ms M Furst and inspiration from Professors G. Thornicroft and M. Tansella (dec’d).
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: A.R. is a Senior Clinical Representative member of the Mental Health Working Group of the Independent Hospital Pricing Authority (Commonwealth Government of Australia). D.R. is a member of the Mental Health Information Strategy Standing Committee (Commonwealth Government of Australia). L.S.-C. is member of the non-for-profit Research Association Psicost that led the development of the Description and Evaluation of Services and DirectoriEs (DESDE) tool. He does not derive any commercial benefit from this organisation.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.