
Abstract
To the Editor,
Steroid-responsive encephalopathy associated with autoimmune thyroiditis (SREAT) is characterized by neuropsychiatric symptoms, including cognitive impairment, seizures and focal neurologic deficits (Castillo et al., 2006). SREAT is still a diagnosis of exclusion, based on the presence of serum anti-thyroid peroxidase (TPO) and/or anti-thyroglobulin (TG) antibodies and responsiveness to corticoid treatment (Endres et al., 2017).
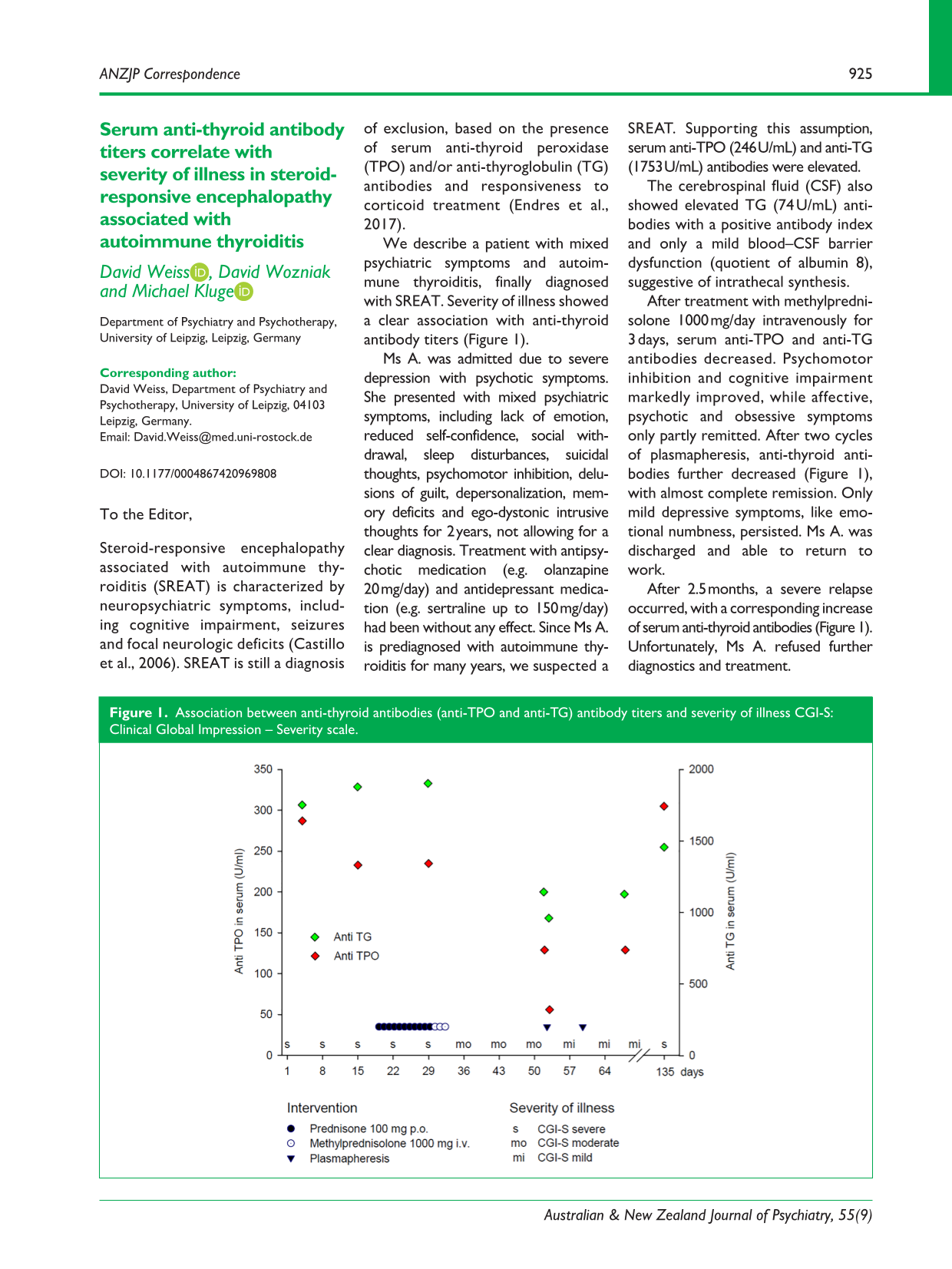
We describe a patient with mixed psychiatric symptoms and autoimmune thyroiditis, finally diagnosed with SREAT. Severity of illness showed a clear association with anti-thyroid antibody titers (Figure 1).
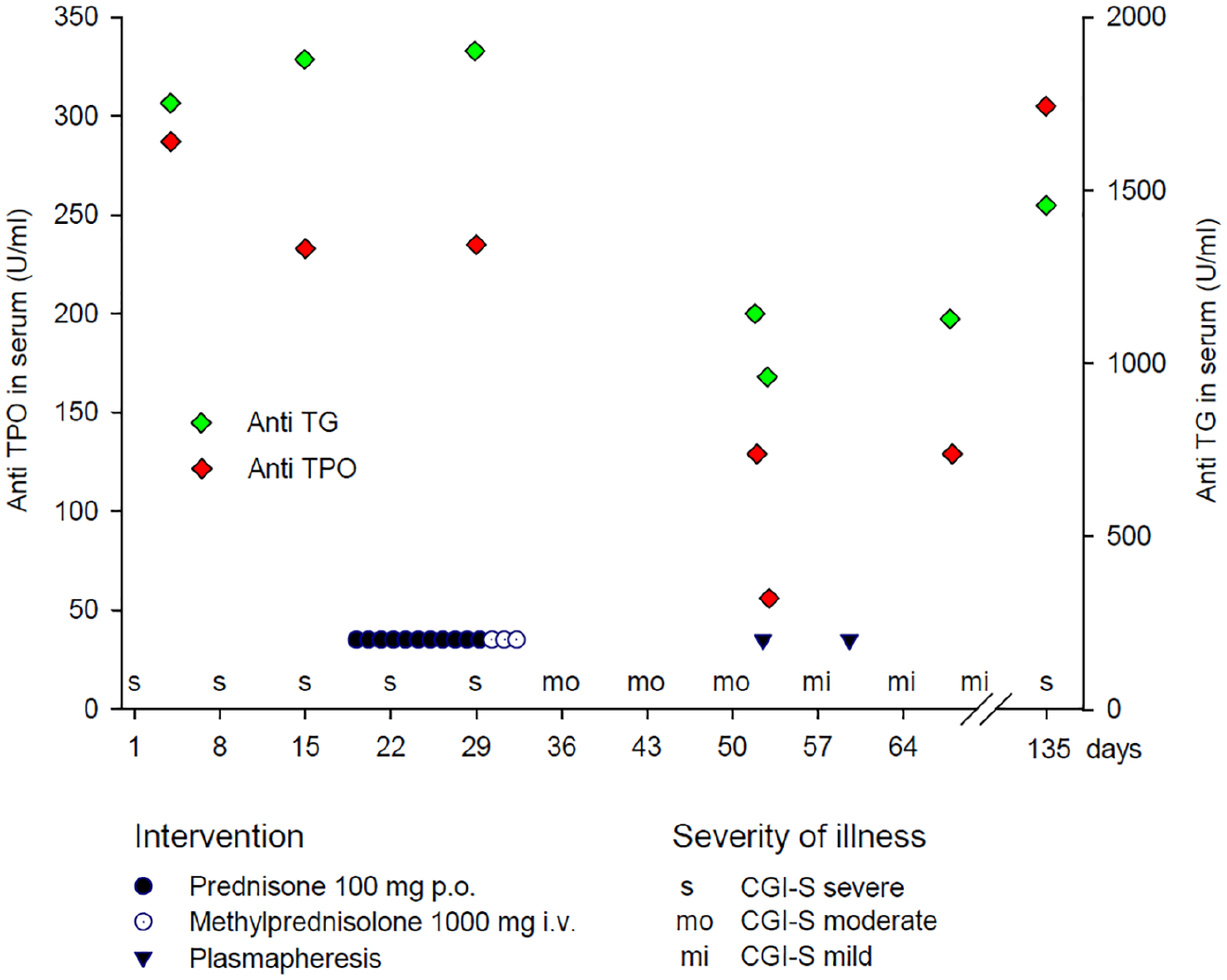
Association between anti-thyroid antibodies (anti-TPO and anti-TG) antibody titers and severity of illness CGI-S: Clinical Global Impression – Severity scale.
Ms A. was admitted due to severe depression with psychotic symptoms. She presented with mixed psychiatric symptoms, including lack of emotion, reduced self-confidence, social withdrawal, sleep disturbances, suicidal thoughts, psychomotor inhibition, delusions of guilt, depersonalization, memory deficits and ego-dystonic intrusive thoughts for 2 years, not allowing for a clear diagnosis. Treatment with antipsychotic medication (e.g. olanzapine 20 mg/day) and antidepressant medication (e.g. sertraline up to 150 mg/day) had been without any effect. Since Ms A. is prediagnosed with autoimmune thyroiditis for many years, we suspected a SREAT. Supporting this assumption, serum anti-TPO (246 U/mL) and anti-TG (1753 U/mL) antibodies were elevated.
The cerebrospinal fluid (CSF) also showed elevated TG (74 U/mL) antibodies with a positive antibody index and only a mild blood–CSF barrier dysfunction (quotient of albumin 8), suggestive of intrathecal synthesis.
After treatment with methylprednisolone 1000 mg/day intravenously for 3 days, serum anti-TPO and anti-TG antibodies decreased. Psychomotor inhibition and cognitive impairment markedly improved, while affective, psychotic and obsessive symptoms only partly remitted. After two cycles of plasmapheresis, anti-thyroid antibodies further decreased (Figure 1), with almost complete remission. Only mild depressive symptoms, like emotional numbness, persisted. Ms A. was discharged and able to return to work.
After 2.5 months, a severe relapse occurred, with a corresponding increase of serum anti-thyroid antibodies (Figure 1). Unfortunately, Ms A. refused further diagnostics and treatment.
Conclusion
First, SREAT can mimic primary psychiatric disorders. Thus, determination of anti-thyroid antibodies should be considered in psychiatric patients, particularly in those with autoimmune thyroiditis.
Second, contrary to the notion that severity of illness is not correlated with antibody levels (Castillo et al., 2006), we saw a significant correlation between laboratory parameters and the clinical presentation. This suggests a direct pathophysiological link, also corroborated by the intrathecal production of anti-thyroid antibodies.
Third, anti-thyroid antibody testing in CSF, currently not established in the diagnostic work-up, could increase diagnostic reliability, since serum antibodies are not disease-specific (Endres et al., 2017; Ferracci et al., 2003).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
The patient provided written informed consent.