
Abstract
Objectives:
The challenges of implementing clinical practice changes are well recognised. Prevailing approaches to tackling them have largely relied on increasing control and standardisation, but with limited impact. We examine research from the behavioural sciences in an attempt to (a) build a clearer understanding of why the implementation of change in clinical settings has proved so elusive and (b) provide practical guidance on how organisations can create a climate that can nurture sustained behavioural change in their workforce.
Method:
We undertook a review of the behavioural science literature to gain a better understanding of the circumstances under which staff might willingly pursue goals that are externally generated. Three studies, derived from the mental health literature, are outlined to illustrate how the manner in which change is introduced can have a significant effect on its uptake and sustainability.
Results:
Research suggests that human behaviour is not as unpredictable as it might at first appear; rather, there are some deeply rooted, psychological processes at play. Self-Determination Theory, a theory of human motivation with an extensive body of research supporting its effectiveness, suggests that the manner in which change is introduced and implemented is critical.
Conclusion:
While improvement methodologies and the use of implementation strategies are necessary, experience would suggest that by themselves they are not sufficient. Overcoming the challenges of implementing change will require a significant shift in our thinking about organisational leadership and the way that change is introduced. Some practical ways leaders can foster staff buy-in for organisational change are proposed.
Keywords
Introduction
The challenges of translating research evidence into practice in healthcare are well documented. A wide range of interventions have been used in the implementation of clinical practice guidelines, but with varying effectiveness (Braithwaite, 2018). Similarly, evidence for the effectiveness of Quality Improvement (QI) has been mixed, with many well-designed studies showing disappointing outcomes (Dixon-Woods and Martin, 2016).
Braithwaite (2018), reflecting on the lack of progress in reducing the rate of adverse events and in the uptake of clinical practice guidelines, concluded, ‘For all the talk about quality healthcare, systems performance has frozen in time’. He argues that we need to tackle this ‘stagnation’ in a new and more effective way.
There has been growing interest in the application of theories (Nilsen, 2015) aimed at gaining a better understanding of how and why implementation succeeds or fails. There remains no generally accepted framework or theory for choosing strategies that are most appropriate for implementing practice change (Gagliardi and Alhabib, 2015). Such findings led Walshe and Freeman (2002) to conclude that the approach used in an organisation ‘probably matters less than how and by whom it is used’.
Rogers (2003) found that while decisions imposed on frontline staff led to high rates of initial adoption, they also met with high levels of resistance and difficulty with sustainability. Whole-team commitment, although more time-consuming, tended to lead to sustained change.
In a systematic review of healthcare organisations struggling to improve quality, Vaughn et al. (2019) found that all studies reported poor organisational culture, with the major themes revolving around (a) limited involvement and ownership by staff, (b) a non-collaborative work environment in which staff did not feel connected to each other or to their organisation and (c) a hierarchical orientation, associated with disconnected and unsupportive leadership and a lack of transparency.
Thakore (2019), professional lead for the Scottish Quality and Safety Fellowship Programme, concluded,
Without understanding the psychology of change, efforts to build knowledge, understand variation, or appreciate the system will have limited success, if any.
We present the argument that people are not passive, nor is their behaviour completely unpredictable. They form intentions and expend considerable effort in setting and achieving goals, and what is critical are the conditions under which they are willingly do so.
We propose that Self-Determination Theory (SDT), a theory of human need fulfilment and motivation with an extensive body of research supporting its effectiveness in health-related behaviour change (e.g. smoking cessation, weight loss, physical activity) as well as in a broad range of other areas (e.g. work, education, sport), holds considerable promise as a psychological theory for explaining behaviour change.
Finding behavioural patterns among complexity
There is a widespread perception that health systems are complex and unpredictable (Braithwaite, 2018), and to reduce potential errors or malfunctions, it is necessary to impose increased standardisation and control, particularly on staff who are perceived as the most variable part of the system (Hollnagel et al., 2015; Jordan et al., 2009). By contrast, studies have demonstrated that in a complex system like health, it is the motivation of staff and their ability to adapt to the situational context which is crucial for the provision of safer patient care (Sujan et al., 2015).
There are numerous examples of behaviours which provide evidence that human behaviour is not as random as it might appear, including the Iron Law of Evaluation, the IKEA Effect and the Not-Invented-Here Syndrome.
Rossi (1987) first coined the term ‘Iron Law of Evaluation’ to describe his observation that as a new model is implemented across a broad range of settings, the net effect will tend towards zero. This is consistent with the finding that many promising and apparently effective health care innovations have little overall impact when ‘rolled out’ more broadly. Various ways in which potential adopters can fall foul of the Iron Law have been proposed (Perla et al., 2015), but evidence suggests that, behind this observation, there are some deeply rooted psychological processes at play.
An indication of the nature of these processes can be found in the IKEA Effect, a cognitive bias in which people place a disproportionately high value on objects or ideas they have created or partially created (Norton et al., 2012). The IKEA Effect is thought to contribute to the related phenomenon of the Not-Invented-Here Syndrome, in which people exhibit a negative attitude towards ideas or knowledge that have to cross a disciplinary, spatial or organisational boundary, resulting in either their suboptimal utilisation or rejection (Antons et al., 2017).
The IKEA Effect is an example of a broader phenomenon encountered in cognitive psychology and the neurosciences, referred to as effort allocation, a multifaceted process driving the decision to choose to engage in high-effort tasks. Cognitive control, the ability to regulate one’s cognition and actions and coordinate their activity in pursuit of specific tasks or goals, has been found to be costly and generally aversive (Shenhav et al., 2017). There is, however, extensive evidence that effort can also add value and even be experienced as valuable and rewarding in its own right (Inzlicht et al., 2018).
Two key questions arise: how (process) and under what circumstances (context) are people prepared to allocate greater effort? Motivation is a multifaceted process that initiates and guides human behaviour towards goal achievement. It is thought to play a significant role in overcoming the cost of effortful action through its enhancing effect on cognitive control (Balmann et al., 2015; Yee and Braver, 2018).
As observed with the IKEA Effect, when people are motivated to invest effort in the creation or partial creation of an object or idea, their positive feelings about the outcome are enhanced. The degree of personal choice in the process appears to be important for building and sustaining a sense of commitment and ownership.
In reflecting on the challenge of improving quality in healthcare, Berwick (2003) observed that we have reached a crossroad. We can either ‘tighten the ropes’ of standardisation and control to achieve small improvements, but at a high human cost, or recognise the centrality of people in re-inventing the system and harness their creativity and their wills. Under what circumstances might staff be motivated to seek to achieve goals that are seen to be externally generated?
Harnessing motivation for change
SDT is a theory of motivation and its role in human development, adaptation and change (Ryan and Deci, 2000). It takes an agentic perspective, starting from the premise that
From birth onward, humans …. are active, inquisitive, curious, and playful creatures, displaying a ubiquitous readiness to learn and explore, and they do not require extraneous incentives to do so. This natural motivational tendency is a critical element in cognitive, social, and physical development …
Motivation may be intrinsic or extrinsic: the former arising from tasks individuals find inherently interesting and satisfying; the latter, mediated by external contingencies, such as approval or tangible rewards or sanctions.
SDT postulates that humans have three innate psychological needs that play a critical role in eliciting, enhancing and sustaining motivation, or diminishing it: autonomy (acting in accordance with abiding values and with a sense of willingness and choice); competence (sense of proficiency and effectiveness); and relatedness (sense of belonging and social connectedness).
The striving for autonomy presents a particular challenge for the implementation of behaviour change within the workplace where the motivation for change is generally externally driven. The critical issue is how externally generated social values, goals and regulations can be experienced as being self-regulated and consistent with personal values.
SDT distinguishes different types or qualities of extrinsic motivation rather than just its strength, recognising that it can vary greatly in the degree to which it is experienced as being personally endorsed or volitional. Extrinsic motivation varies along a continuum from controlled to autonomous motivation based upon the perceived locus of causality. The least autonomous form of extrinsic motivation is external regulation that emerges from feeling pressured to behave in certain ways to satisfy an external demand or obtain an externally imposed reward. At the other end of the continuum is integrated regulation that emerges from acting with a sense of congruence with one’s own values and needs and with a full sense of volition. This motivational continuum is illustrated in Figure 1. Intrinsic motivation and motivation arising from integrated regulation share certain similarities and are collectively known as autonomous motivation (Gagné and Deci, 2005).
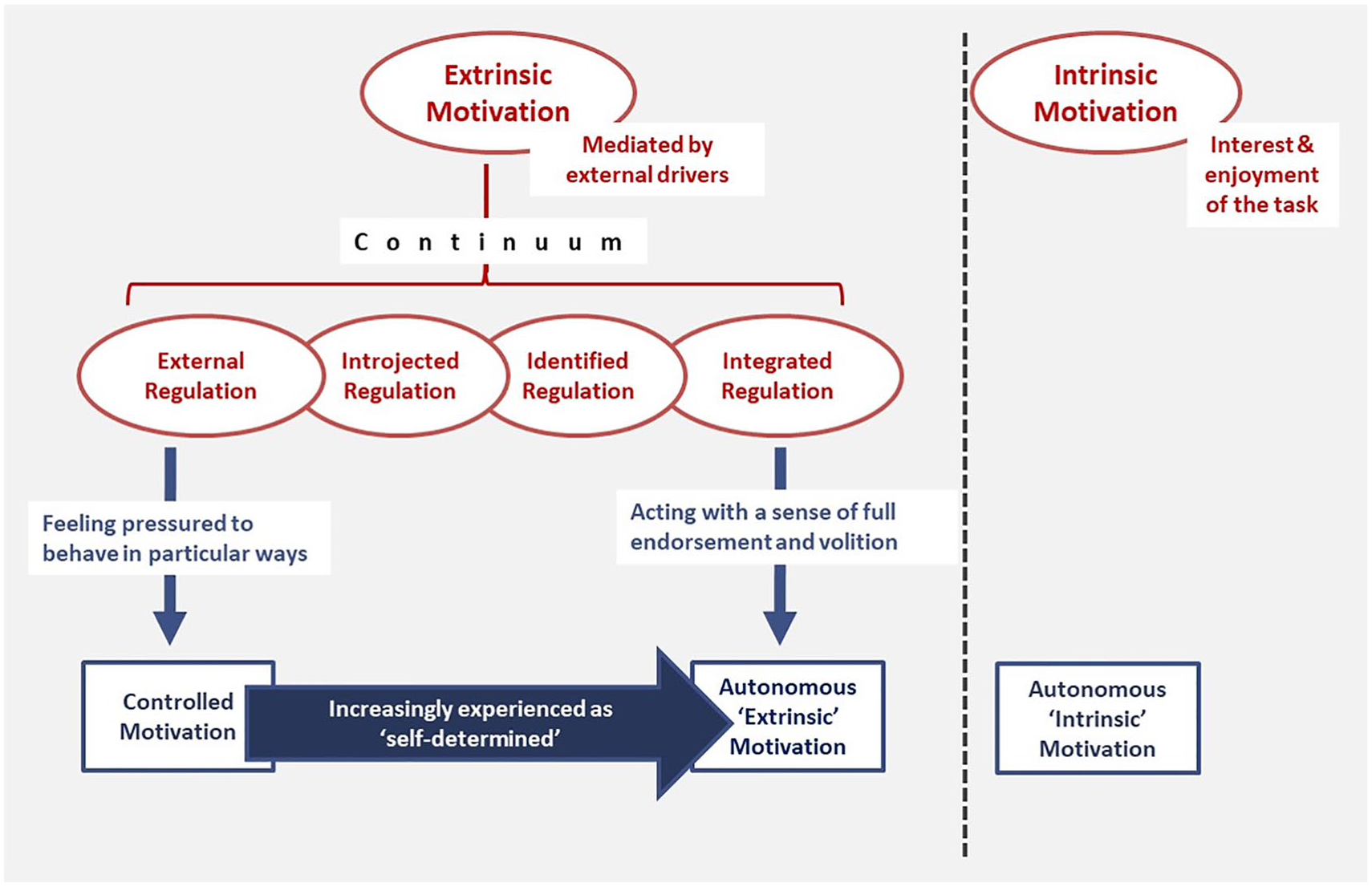
Self-Determination Theory and the motivational continuum.
Work climates that meet workers’ basic psychological needs for autonomy, competence and relatedness foster autonomous motivation, leading to engagement of staff with their workplace. In such autonomy-supportive environments, people internalise previously external sources of motivation and more willingly adopt and assimilate workplace values, goals or regulations as their own. What is critical is how they are presented to, and experienced by, staff.
By contrast, work environments characterised by greater external control, including an emphasis on standardisation, target setting, surveillance and other control measures, result in controlled motivation, leading to staff disengagement, constrained performance and undermined well-being. Although controlled motivation may produce a level of compliance, it fails to build commitment to sustainable change.
There is evidence that autonomous motivation is associated with a wide range of positive workplace outcomes including increased persistence on a task and maintenance of behaviour change; enhanced performance, particularly on tasks requiring creativity; higher productivity; and high levels of engagement of staff with their workplace (Gagné and Deci, 2005).
Combining extrinsic and intrinsic motives does not necessarily boost motivation. Rather, the former can undermine the latter, leading to a drop in overall motivation, with an associated reduction in performance and persistence (over-justification effect). A 10-year study assessing the impact of intrinsic and extrinsic motives on the careers of 10,000 West Point cadets found extrinsic motives undermined the positive effects of intrinsic motives, and this effect persisted over many years, negatively affecting long-term career outcomes (Wrzesniewski et al., 2014).
Evidence suggests people place a high value on interactions with others and that the level of trust and cooperation between them is dependent on a sense of ‘social closeness’. Research has shown that people are powerfully motivated by the need for maximising self-esteem and a positive self-image and that social contexts that enable them to feel good about themselves and to look good in the eyes of others increase prosocial behaviour (Tamir and Hughes, 2018). This is consistent with findings from SDT that a sense of connectedness with a work group provides the groundwork for people showing a willingness to consider adopting values or goals generated by others.
Leadership for organisational change
Leaders have an enormously important role to play in the implementation of organisational change (Walshe and Freeman, 2002). However, there is growing recognition of the need for collaboration between leaders and frontline staff, with a more distributed form of leadership, referred to as ‘collective leadership’. This is envisaged as a property shared by multiple individuals and not simply a product of positional authority (McKee et al., 2013; West et al., 2014).
This calls for a shift in the mindset of leaders from seeing staff as ‘passive receivers’ to ‘active co-creators’ of change. Senge (1990) argues that leaders need to build a ‘shared’ vision of the future they seek to create to foster genuine commitment rather than compliance.
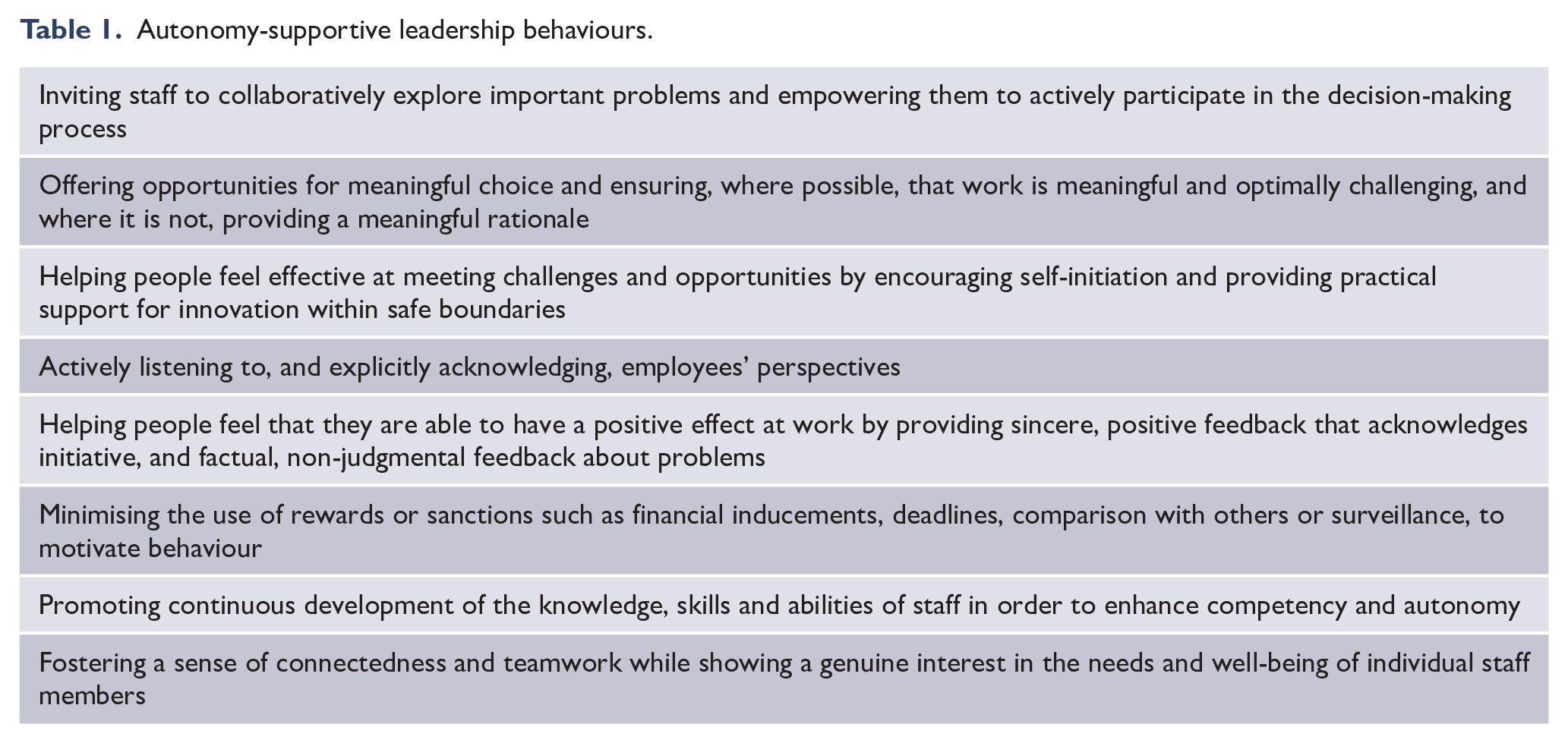
SDT offers a plausible explanation of how leadership shapes staff motivation and engagement (Gagné and Panaccio, 2014). From an SDT perspective, the critical determinant in staff buy-in to organisational change is not in the nature of interventions, specific tools or activities, but in the degree to which staff experience their work environment as satisfying their psychological needs (autonomy-supportive). Outlined in Table 1 are a cluster of leadership behaviours that have collectively been found to promote autonomous motivation and provide a path to sustainable change (Fowler, 2018; Stone et al., 2009).
Autonomy-supportive leadership behaviours.
The motivational continuum and implementation outcome
Implementation strategies can be aligned along the motivational continuum based upon the degree to which the process is experienced by staff as autonomy-supportive – ranging from feeling pressured to act (controlled motivation) at one end, to acting with a sense of full endorsement and volition (autonomous motivation) at the other.
Three mental health implementation studies, derived from an extensive review of the literature, are briefly outlined below to illustrate this concept.
Study 1: introducing Joint Crisis Plans for people with psychosis
Thornicroft et al. (2013) undertook a randomised controlled trial to compare the effectiveness of Joint Crisis Plans (JCPs) in reducing compulsory treatment for people with severe mental illness. JCPs are plans developed with patients of their treatment preferences for any future psychiatric emergency. Sixty-four community mental health teams from four health provider organisations participated. Two previous studies had suggested that JCPs might reduce compulsory treatment.
Five senior mental health nurses were employed as facilitators to deliver the intervention. Each participant in the intervention group was invited to two meetings: the first (preparatory) introduced the patient and their care coordinator to the principles and process of JCPs, and the second (planning), at which the JCP was finalised, was attended by the patient, their care coordinator, their psychiatrist and the JCP facilitator.
No difference was found between the intervention and control groups for the primary outcome of reduced compulsory admissions. Fidelity to the intervention and quality of the JCPs were assessed as high. In an attempt to explain this outcome, the researchers highlighted two important factors: (a) previous efficacy trials involved clinicians who had expressed an interest in the intervention (compared with assertively recruited clinicians with more variable buy-in), and (b) JCP interventions were introduced without specific attention to local staff or organisational context and readiness.
Study 2: evaluating the introduction of JCPs into routine clinical practice
Williams et al. (2014) undertook the evaluation of 1-year pilot programme to field-test the introduction of a standardised crisis planning tool into routine practice in four community mental health services; two metropolitan and two country-based. The aim of the programme was to empower consumers and reduce relapse through early detection and treatment based on consumer preferences. Services were invited to participate, and each site agreed to a target of 40 completed JCPs.
Governance of the project consisted of a small project management group (a full-time senior clinical planning officer and a psychiatrist one session per week) which reported to a steering committee. A mix of interventional strategies were used, including a representative of each of the sites on the steering committee; regular teleconferences and site visits by the project management group to provide ongoing support; audit and feedback; and the provision of training (multi-modal delivery) for staff on the JCP process and the use of the standardised tool.
An independent evaluation of the project found that JCPs enhance consumer’s sense of empowerment, but the short time-frame prevented an analysis of the effects of JCPs on the prevention and management of crises. The most conspicuous finding was the marked difference in the number of completed JCPs at the four sites (38, 28, 17 and 0). The study reflected on the critical importance of addressing context and culture in each individual service and the need to tailor the implementation strategy to take account of variations in organisational readiness between services.
Study 3: implementing clinical guidelines in psychiatry
Forsner et al. (2010b) undertook a study of the local implementation of clinical guidelines for the assessment and treatment of depression and of suicidal behaviour in outpatient psychiatric clinics in Stockholm. Of the six clinics which were invited to participate in the study, four accepted while two declined. Implementation started with analysis of the gap between clinical guidelines and current local practice at each clinic.
A mix of interventions were used, including the establishment of locally elected multidisciplinary implementation teams to set goals and develop implementation plans based upon local needs in collaboration with all members of staff; training of implementation teams in improvement strategies (e.g. Plan-Do-Study-Act [PDSA]); regular audit and feedback; seminars to introduce guidelines according to local needs; and monthly academic outreach visits to facilitate analysis of, and reflection on, staff attitudes and behaviours.
In each of the participating clinics, the implementation teams were encouraged to engage all staff in adapting the guidelines and protocols for local use. Compliance with the guidelines increased and was sustained over the 2-year follow-up. In a follow-up study (Forsner et al., 2010a), three main differences in attitudes and beliefs were found between clinicians at non-participating and participating clinics: (a) concerns about professional autonomy, (b) beliefs about evidence-based practice and (c) concerns about potential financial motives.
Each of these studies was analysed through the ‘lens’ of SDT based upon whether the implementation process was supportive of the psychological needs of staff. The findings from the studies are set out in Table 2. The fact that studies can only be rated from the content of published journal articles presents a major limitation and ratings should be seen as ‘indicative’ only.
Estimated level of autonomy support for frontline staff.
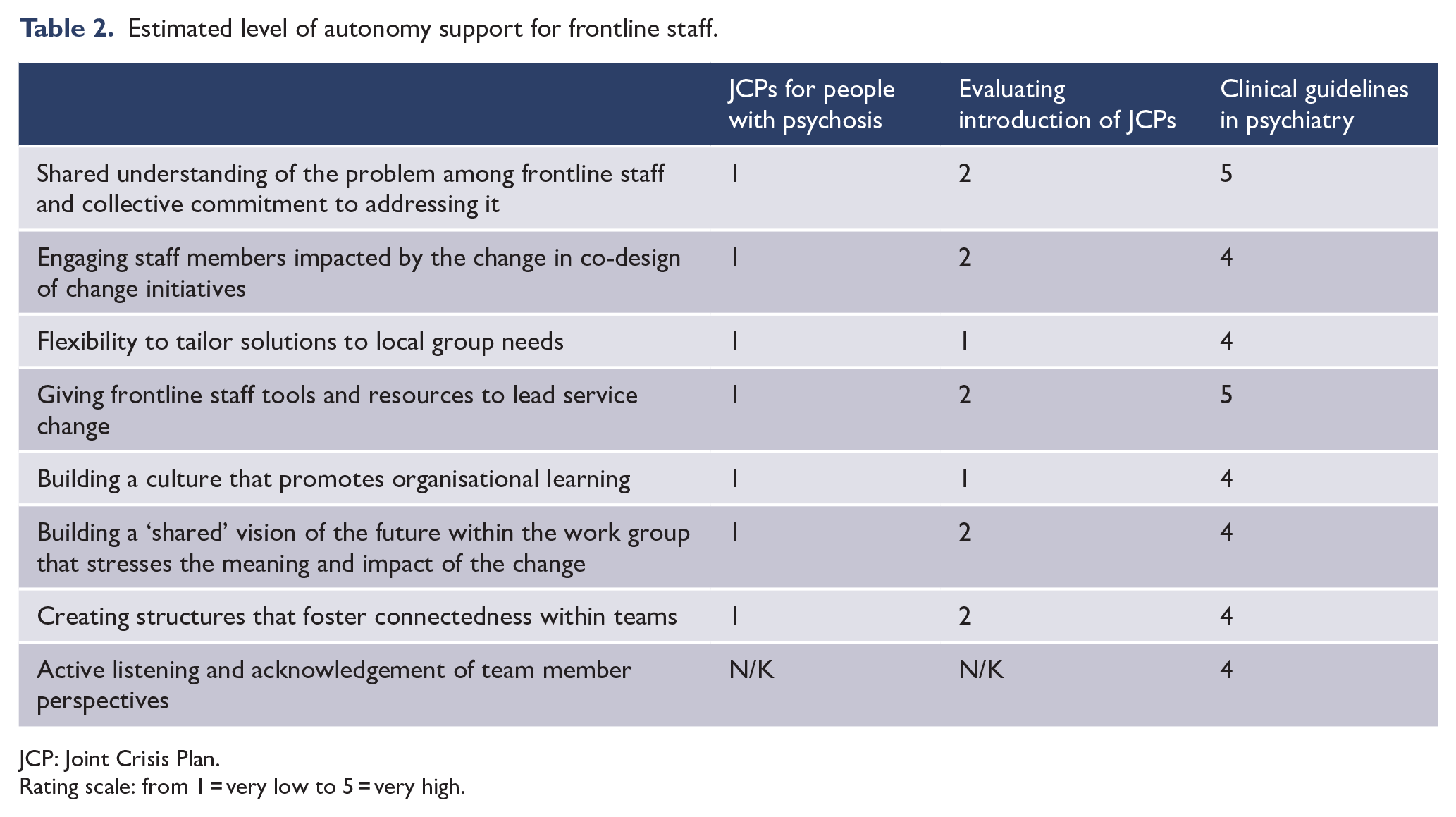
JCP: Joint Crisis Plan.
Rating scale: from 1 = very low to 5 = very high.
The Forsner et al. study differed substantially from the other two studies in three fundamental aspects: (a) implementation was tailored to the needs of each participating clinic; (b) the whole staff group at each site was centrally involved throughout; and (c) it was underpinned by the Theory of Planned Behaviour (Ajzen, 1991), a motivational theory that, like SDT, recognises the critical importance of staff having a sense of choice and control in the change process.
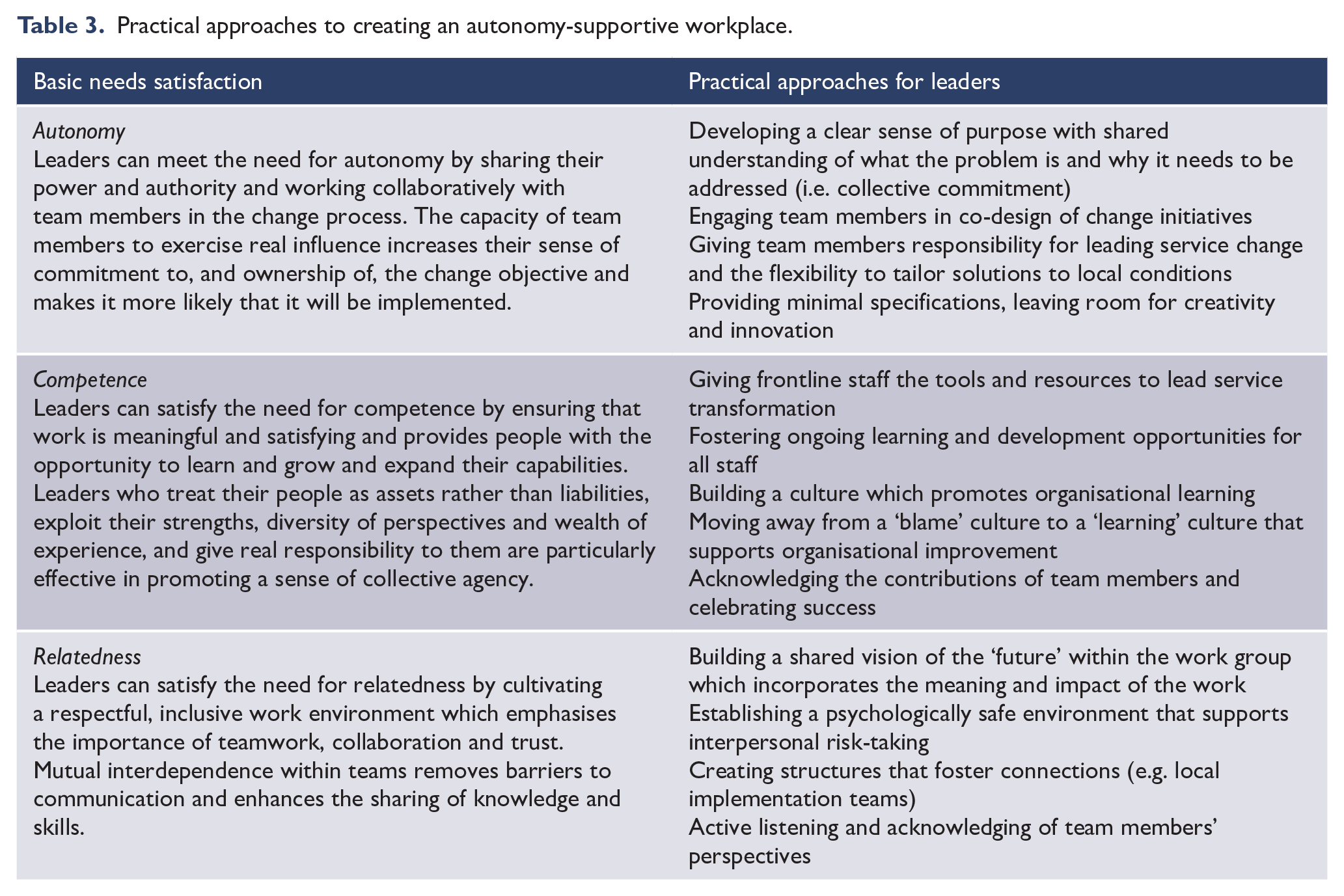
From an SDT perspective, the closer an implementation process is to the autonomous motivation end of the continuum, the greater the willingness of staff to change their behaviour and the greater the likelihood of a successful and sustained outcome. To illustrate this, in Figure 2 each of the studies is positioned on the motivational continuum. Table 3 highlights some practical ways in which healthcare leaders can foster an autonomy-supportive workplace.
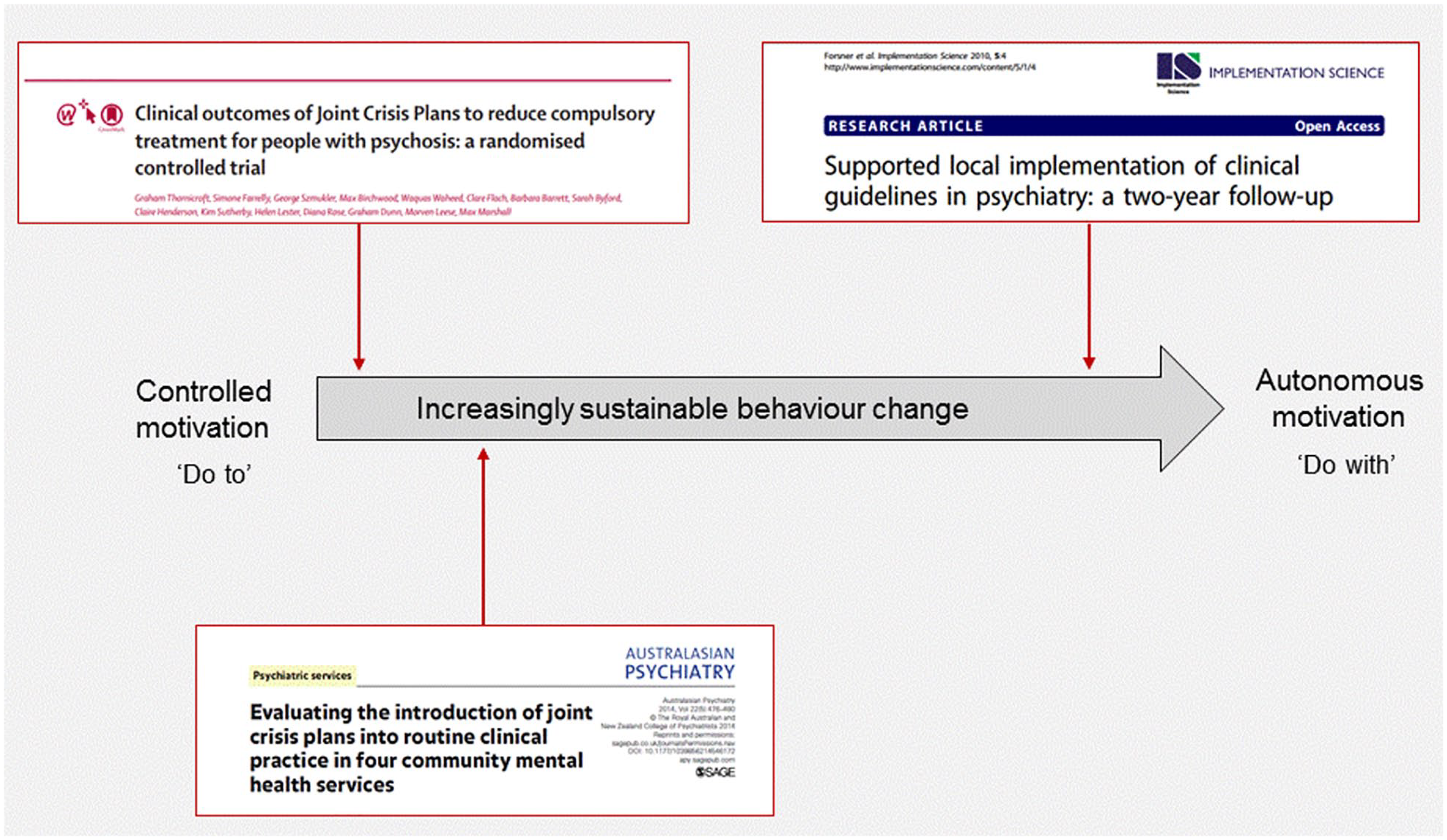
Implementation studies arrayed along the motivational continuum.
Practical approaches to creating an autonomy-supportive workplace.
Conclusion
Unexpected variations in the outcomes of the same improvement interventions are often attributed to incorrect execution of the intervention, and it is generally assumed that better intervention design, quality control and standardisation will reduce potential errors (Jordan et al., 2009). We contend, however, that this variability in outcome is not a transfer problem, but rather a deeply embedded human response to approaches that seek to tighten control.
While improvement methodologies and the use of implementation tools and strategies are important and necessary, experience would suggest that, by themselves, they are not sufficient. From an SDT perspective, the essential ingredient for sustainable change is the creation of a work environment that recognises the centrality of staff and their psychological needs in the change process.
SDT meets the desirable attributes set out by Eccles et al. (2005) for a causal theory: namely, (a) effectiveness in predicting and explaining behaviour change in a range of settings, (b) ability to account for non-volitional aspects of change and (c) providing guidance on how leaders can nurture sustained behavioural change. This article highlights the contribution that behavioural theories, like SDT, could potentially make to our understanding of what drives sustainable practice change.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.