
Abstract

In recent years, self-harm has garnered increasing awareness, in both clinical and population contexts, as an important warning sign for potential psychopathology. Studies examining self-injurious behaviour in adolescents found that 1 in 12 reported self-harming, with the peak of prevalence around the age of 15 years (Moran et al., 2012). Indeed, governments and leading mental health organisations have published articles to assist in the detection of self-injurious behaviours and clinical practice guidelines have been developed to assist clinicians in the management of patients who self-harm (Carter et al., 2016). However, despite this increase in interest among both academic and clinical groups to understand and treat self-injury, and the knowledge that the prevalence of self-harm decreases rapidly from mid-adolescents to young adulthood, there is currently no formal diagnosis that can be used to define adolescents who cut, burn, poison, overdose, practice self-battery or use a myriad of methods to cause damage to themselves. Hence, in practice, there is often confusion surrounding suicidal thinking and suicide.
In the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), there is one potential diagnosis on the horizon that is described under ‘conditions for further study’ as non-suicidal self-injury (NSSI). This proposed diagnosis utilises tangible, behavioural outcomes (self-injury) and endeavours to link these behaviours with certain cognitive drivers to form a ‘diagnosis’. However, it raises a key question, namely, the purpose of the diagnosis. Furthermore, a close examination of the criteria for NSSI raises concerns regarding its clinical value. Nevertheless, at the same time, the concept of a diagnosis for self-injury – and especially one which is unrelated to suicide per se – is clearly needed, and hence why in this Make News we undertake a critical examination of the proposed diagnosis of NSSI and consider how it may be adapted for future use.
NSSI
Throughout the literature regarding self-injury and within the proposed criteria for NSSI in DSM, a core feature of the syndrome is that the self-injury is not driven by suicidal ideation. In this way, NSSI cannot be applied to individuals whose self-injurious behaviour is driven by suicidal ideation or impulsive suicidal acts such as those observed in borderline personality disorder (BPD). This means that the diagnosis of NSSI is contingent on the cognition of the individual and is therefore defined more so by absence of suicide as a driver for the behaviour, rather than the behaviours themselves. This neatly separates NSSI from suicide but prompts the question: if suicide (more specifically thinking about suicide) is not the cognitive driver underlying self-injury in NSSI, then what is?
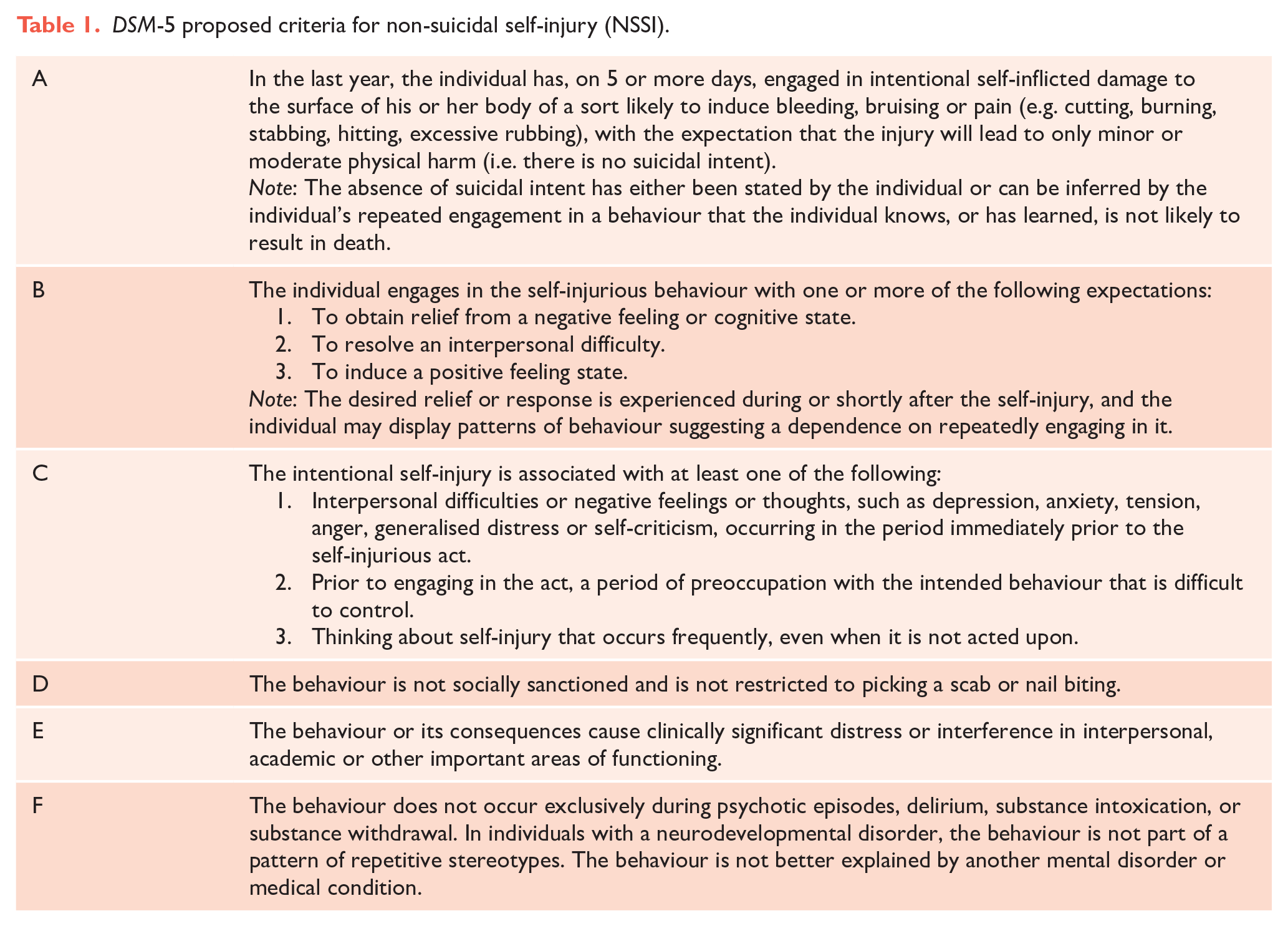
Research examining NSSI suggests that the ‘condition’ is extremely complicated and that at present our understanding is incomplete; however, key motivations underlying and reinforcing self-injurious behaviour seem to be emotional/psychological experiences, and interpersonal factors (Hasking et al., 2017; Zetterqvist et al., 2020). These two drivers appear to reinforce the NSSI, as the behaviour becomes a means of regulating responses to either the emotional or social triggers that are causing distress. This research into the mechanisms of NSSI is ongoing, and certainly more needs to be uncovered to map the development of NSSI and pinpoint the origins of its occurrence as a learned behaviour. However, interestingly, some of what is broadly understood about NSSI at present is not fully captured within the proposed criteria in DSM (see Table 1).
DSM-5 proposed criteria for non-suicidal self-injury (NSSI).
The proposed criteria
As alluded to, the key features of NSSI are that the cognitive drivers are non-suicidal in nature and that the drivers that do motivate the self-injury are generally intrapersonal (emotional, psychological) and/or interpersonal experiences. Arguably, these two components define NSSI, and yet, they are poorly represented, if at all, in the proposed DSM criteria.
Criterion A (see Table 1) attempts to establish some form of threshold for diagnosis on the basis of the frequency with which the self-injurious behaviour occurs. The criterion of ‘5 or more days’ (over the last year) seems to have little empirical support and apart from being difficult to determine seems to imply that an individual must intentionally harm themselves a minimum number of times before the harm can be regarded as pathological. Therefore, clinically, the criterion is problematic both because it is hard to measure and because the threshold is arbitrary. In addition, this component of criterion A distracts from the second condition, namely, that self-injury must not be within the context of suicidal intent.
This requirement for the individual to not be motivated by suicidal intent at the time of self-injury raises several issues. The first of these is that in clinical practice it may be difficult to ascertain in retrospect whether the individual was self-harming with suicidal intent, and this is likely to be even more difficult if it occurs during adolescence where there are developmental factors and there is often additional comorbid psychopathology. The second issue is that this stipulation leaves NSSI prone to diagnostic overshadowing if the individual has demonstrated suicidality in the past but is now (in the present) self-injuring for reasons distinct to suicidal intent. This is possible, given that the cognitive drivers underlying NSSI are believed to be distinct from those that may drive suicidality, and hence, both processes may be concurrently present in the one individual and disentangling the specific motivations underlying each incident of self-injury is likely to be extremely challenging.
Criterion A also includes a note that determining whether suicidal intent was a contributory factor in the self-injury can be done via the patient retrospectively reporting motivations for self-injury or can be inferred by the patient knowing or learning that the method would not result in death. This last point is confusing and in some ways can contradict the assumption that NSSI must be conducted without suicidal intent, because it implies that an individual could have engaged in the injurious behaviour experimentally (not knowing that it would not lead to death). Thus, the individual may not have made a conscious assessment of potential lethality in the first instance and therefore the lack of suicidal intent is difficult to ascertain.
Within criterion B, the first expectancy potentially driving NSSI describes obtaining relief from a negative feeling or cognitive state. This is problematic, as evidence has suggested that the emotional or psychological states that may drive NSSI are not only those typically perceived as ‘negative’, such as anxiety, anger or frustration, and may also include positive emotional experiences, as individuals who engage in NSSI appear to experience difficulty responding to a broad range of emotional stimuli (Hasking et al., 2017). Furthermore, evidence suggests that, rather than utilising NSSI to obtain relief from these emotional or psychological states, the behaviour is more so a means of regulation. The following two expectations listed in criterion B, namely to ‘resolve an interpersonal difficulty’ and to ‘induce a positive feeling state’, also do not appear to be grounded in research examining NSSI. Although social and interpersonal factors may facilitate NSSI, evidence does not suggest that self-injury is conducted as a means to resolve difficulties but rather as a means to regulate the individual’s response to difficulties. Moreover, the injury is conducted to regulate and modulate emotional and psychological states rather than to induce a positive one as a means of reprieve.
The specificity provided by criterion B is further brought into question when considering criterion C, which details the precipitants of the self-injurious behaviour. Here, each of the listed precipitants conceptually overlaps with the expectations of the behaviour outlined in criterion B, and this significant convergence has been shown empirically, with 80–90% of participants that endorse a component of criterion B also endorsing the corresponding component of criterion C (Buelens et al., 2020). For example, if an individual is engaged in NSSI to obtain relief from a negative cognitive feeling or state (B1), it would be highly likely that negative feelings or thoughts would occur immediately prior to the self-injurious behaviour (C1). It has therefore been debated whether criterion B should be removed altogether as it is subsumed within criterion C, or whether B and C should be amalgamated or altered in some way to provide more specificity to the diagnostic criteria.
Interestingly, NSSI also appears to be somewhat unusual in that criterion E, which stipulates that the disorder should cause distress or impact functioning, has come under scrutiny. Studies have shown that individuals who engage in NSSI do not necessarily view the behaviour as distressing or impairing, indeed it is sometimes regarded (or deemed to be) as helpful, as the behaviour is utilised by individuals as a coping strategy to regulate their responses. However, it has been shown that criterion E successfully distinguishes individuals with and without NSSI disorder, and therefore, it arguably provides clinical utility in screening individuals experiencing distress and impairment. Therefore Criterion E should be researched further, perhaps using a change in the phrasing of the criterion to capture those aspects of the disorder that cause impairment but are not always considered by patients (e.g. the impact of visible scars on functioning).
Finally, criterion F addresses one key aspect of NSSI that has garnered much attention, namely that ‘the behaviour is not better explained by another mental disorder’. This is striking, as self-injurious behaviour has historically been strongly associated with BPD, indeed in the ‘Differential Diagnosis’ subsection for NSSI, DSM notes that ‘... nonsuicidal self-injury was regarded as pathognomonic of borderline personality disorder’. Numerous studies have shown NSSI to be a diagnostic entity that is distinct from BPD and other disorders, and this is where the clinical investigative utility of NSSI is perhaps most evident (Buelens et al., 2020). As NSSI has been shown to exist not only within BPD, but within mood, eating, trauma and substance misuse disorders, as well as on its own without comorbidities, it could hold insights into the underlying cognitive mechanisms that drive self-injury within these many overlapping, but essentially distinct disorders, and the differences that separate them.
A way forward
A way to progress NSSI as a feasible diagnosis with clinical utility would be to expand the diagnosis to include those individuals that demonstrate the cognitive processes for NSSI but have not yet crossed the threshold into self-injurious behaviours (see Figure 1). Currently, the diagnosis is based on the tangible outcome of self-injury and therefore only captures individuals that have crossed the self-injury ‘threshold’. By this time, they have typically learned the behaviour and reinforced the cognitive drivers that led them to self-injure in the first instance (area B, Figure 1). By expanding the diagnostic criteria to capture individuals that demonstrate self-injury ideation (area A, Figure 1), the volitional factors that lead to the individuals crossing the self-injury threshold can be examined more granularly. In addition, broadening of NSSI would facilitate comparisons between those who do self-injure and those that have not (as yet) and provide insights into what factors separate the two groups.

The cognitive processes that precede NSSI.
Finally, an understanding of the cognitive drivers that lead to self-injury could provide a foundation for preventive measures and also inform interventions that can be used once the behaviour has emerged. For instance, determining whether the primary motivator for engaging in NSSI is to regulate internal feelings or states, or to obtain relief from interpersonal difficulties, would point to the primary target for interventions. Therefore, by examining individuals who have not yet engaged in NSSI, but demonstrate the same patterns of cognition as those with NSSI, interventions that address and institute skills in emotion regulation and coping strategies for interpersonal and social stressors may be able to diminish the likelihood of self-injurious behaviour. And so, although the diagnosis of NSSI is predicated on harm it does have the potential to reduce harm if investigated further and suitably refined.
Make News
In an age where good news and good ideas are difficult to find, this series offers constructive criticism of promising concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. The author E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.