
Abstract

To the Editor
Marchiafava–Bignami disease (MBD) is a rare neuropsychiatric disorder characterized by demyelination and necrosis of the corpus callosum commonly associated with chronic alcoholism or malnutrition (Sera and Ichiba, 2019). A case of a 32-year-old male presenting with acute psychosis preceding the diagnosis of MBD has been recently reported (Naaz et al., 2018). MBD presenting with depression has been rarely reported in the literature.
We present the case of a 29-year-old man with major depressive disorder (MDD), with a 3-month history of extremely poor oral intake. Written consent for publication was provided by the patient’s mother. The patient had been suffering from MDD for a year after marital disharmony and had attempted suicide. He had no history of an alcohol-use disorder. Despite regular intake of antidepressants, no improvements were observed in his depressive symptoms. Upon admission, the patient appeared cachectic with minimal verbal output and was blind. He continued to take little food or fluid and needed to be coaxed regularly. Neurological examination revealed generalized muscle atrophy and hyporeflexia; thus, an initial working diagnosis of MDD with catatonia was made. He was recommended electroconvulsive therapy (ECT) after pharmacological intervention failed to provide an adequate response. Minimal response to ECT and pharmacotherapy was observed; therefore, a secondary cause for his condition was explored, and neuroimaging was performed. Brain magnetic resonance imaging (MRI) (Figure 1) showed an atrophic corpus callosum with relative sparing of the splenium, which was consistent with the radiographic features of MBD. Despite aggressive treatment with vitamin B complex for 2 months, the patient did not improve and later passed away at home.
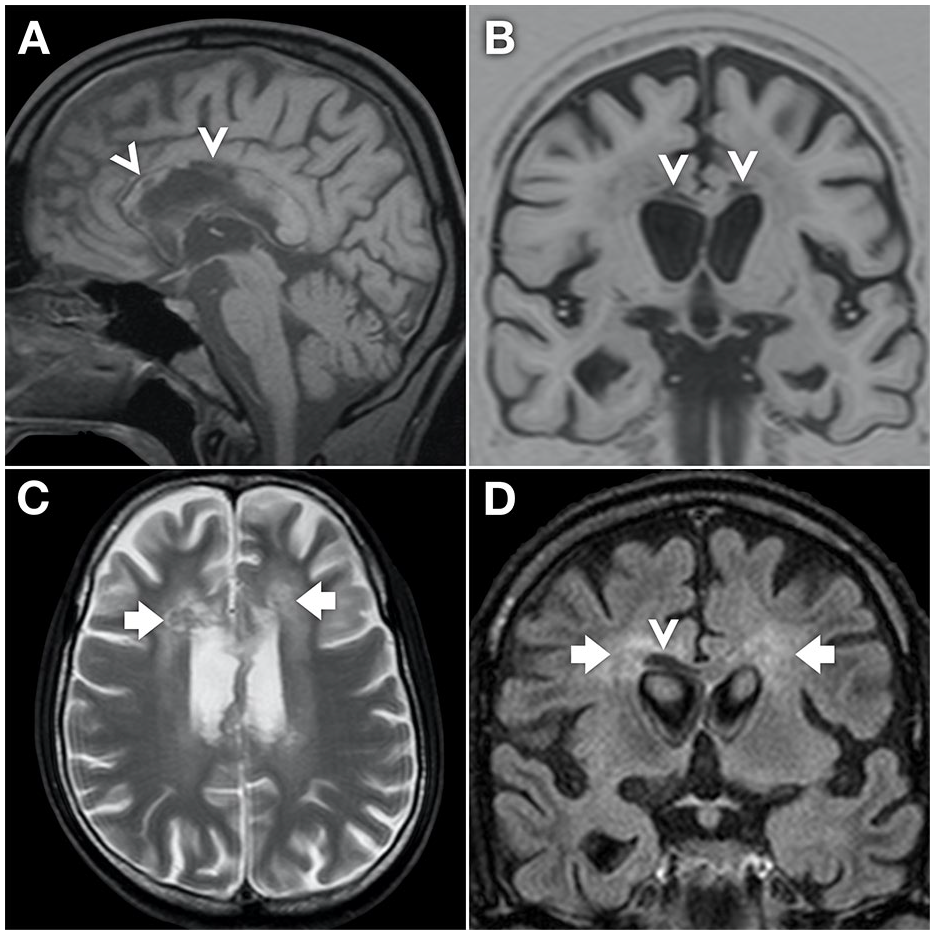
Non-contrast magnetic resonance images (A, sagittal T1; B, coronal inversion recovery; C, axial T2; D, coronal FLAIR) demonstrate central involvement of the corpus callosum (arrowheads), but relatively sparing the splenium. An increase in T2 signal also extends laterally into the white matter of the centrum semiovale bilaterally (arrows).
The etiology and pathophysiology of MBD remain indefinite, with sparse evidence of medical intervention strategies; hence, guarded clinical outcomes and prognosis are not uncommon. The advent and evolution of MRI have helped in early diagnosis, identifying associated pathophysiological mechanisms, and making the prognosis of MBD feasible (Dong et al., 2018). We highlight the importance of a high index of suspicion for MBD with atypical clinical presentation and cases with an inconsistent therapeutic response to depression. Timely MRI is imperative in such cases, especially those with an underlying history of malnutrition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.