
Abstract
Introduction
The National Mental Health Service Planning Framework (NMHSPF) aims to translate evidence into policy (Whiteford et al., 2013). Based on this apparently solid foundation, the NMHSPF is used to allocate resources in Australia’s public hospital and community mental health sectors, affecting the working lives of public sector psychiatrists around the country. Some State/Territory Governments are relying on the NMHSPF to solve major problems such as emergency department (ED) access block (Allison et al., 2020)—where patients experience extended stays in EDs while awaiting admission, and may be discharged early to free up beds before receiving adequate inpatient treatment. Premature discharge can be associated with heightened risks of suicide, aggression, incarceration and homelessness.
However, the NMHSPF’s planning targets are questionable because they are based not only on empirical evidence, but also on opinion. While the Commonwealth has not, to date, agreed to release full details of the NMHSPF’s algorithms, there is sufficient information in the public domain to be certain that key targets are decided by working groups (NMHSPF Planning Materials: https://nmhspf.org.au/). Thus, the NMHSPF is hybrid model based on opinion as well as data-based science.
The first step in epidemiologically -based planning models like the NMHSPF is determining the burden of mental illness in the population, followed by identifying interventions that might reduce this burden, and finally organising interventions into service delivery frameworks (Whiteford et al., 2013: 703). Using this approach, the NMHSPF utilises prevalence and severity data to derive 155 need groups of differing complexity and disability, and then brings together cost-effective interventions to estimate the required activity (e.g. service contacts and hours) and resources (e.g. beds, staff and dollars).
However, epidemiologically based models face difficulties estimating the required numbers of psychiatric beds for a given population, because there are few studies on optimal inpatient care for mental illness (O’Reilly et al., 2019). Therefore, these models use expert opinion to assign for instance lengths of stay, readmission rates, and the critical ratio of hospital to community beds. Given that expert opinion has this role in the NMHSPF, we can inquire how the opinions of those who determined Australia’s desirable service levels compare with other expert consensus targets, and with psychiatric bed numbers reported by high-income countries.
Benchmarking the NMHSPF
While Australia’s per capita supply of public sector acute psychiatric beds has been approximately constant since the early 1990s, the recent Productiv-ity Commission Mental Health Draft Report noted a significant decline in the per capita supply of public sector non-acute beds (Productivity Commission, 2019: 311–312, vol. 1). As a result, the NMHSPF model indicates a 60% shortfall in Australia’s public sector non-acute beds (Productivity Commission, 2019: 286–287).
Based on expert opinion, the NMHSPF allocates most of this shortfall to the community residential care sector. The NMHSPF’s ratio of community to hospital non-acute beds was set at 80%/20% ‘to reflect the Expert Working Groups’ views of the preferred service model, but it can be varied by jurisdictions because currently there is wide variation’ (NMHSPF Care Profiles, p. 95: https://nmhspf.org.au/). In view of this wide variation between States/Territories, The Adult Psychiatry Imperative (TAPI) submission from 48 psychiatrists to the Royal Commission into Victoria’s Mental Health System recommended a benchmark of at least 15 public sector hospital non-acute beds per 100,000 for general adults with newly commissioned beds to be located in research-intensive university-linked rehabilitation centres (Allison et al., 2020).
As shown in Table 1, Australia reported to the 2017 World Health Organization (WHO) Mental Health Atlas Project that the nation had considerably fewer beds per capita in stand-alone hospitals and community residential care units, and more beds per capita in general hospitals than the WHO medians for high-income countries and Europe. As a result of this divergent bed base, Australia is relatively more reliant on short admissions to general hospitals, adding to the pressure in the EDs, and has less capacity in standalone hospitals for longer admissions for the stabilisation and rehabilitation of severe mental illness. The WHO median for admissions to standalone hospitals was under 12 months for most patients (81%), but a minority (14%) stay 1–5 years, and small percentage (5%) stay over 5 years in high-income countries.
World Health Organisation – hospital and community beds for all ages per 100,000 population.
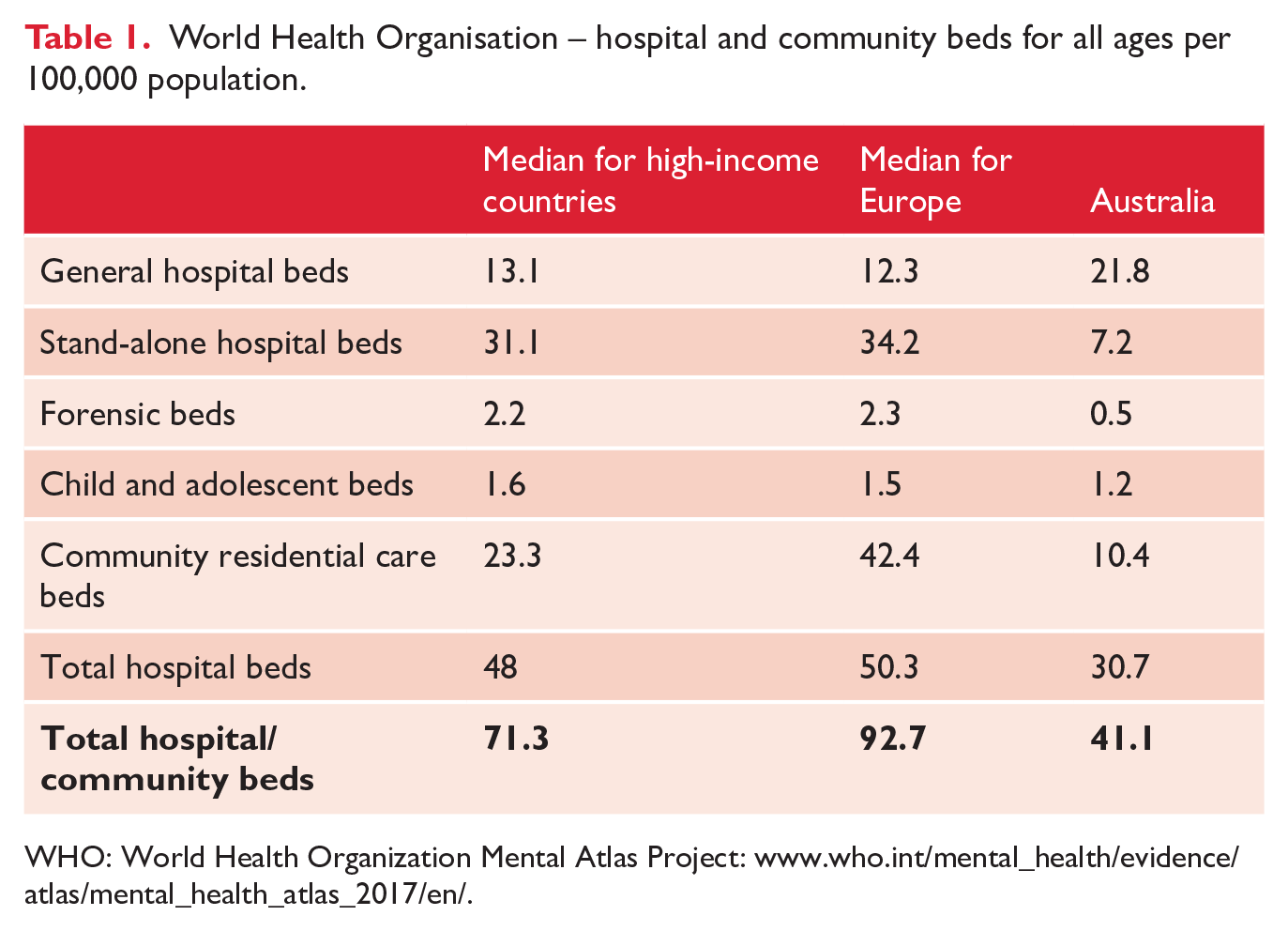
WHO: World Health Organization Mental Atlas Project: www.who.int/mental_health/evidence/atlas/mental_health_atlas_2017/en/.
As highlighted in Table 2, the NMHSPF target for total per capita hospital and community beds is higher than Australia’s current provision with the major difference being a doubling of community beds (Productivity Commission, 2019). However, NMHSPF’s targets for hospital beds are lower than those in an expert consensus statement from the Sainsbury Centre for Mental Health in England, now the Centre for Mental Health, which has been used as a comparator for Australian planning estimates. The Sainsbury Centre’s higher target for acute beds was partly to compensate for the lower access to private sector beds in England (Harris et al., 2012).
Public sector hospital and community beds per 100,000 population for all ages excluding high secure and forensic beds.
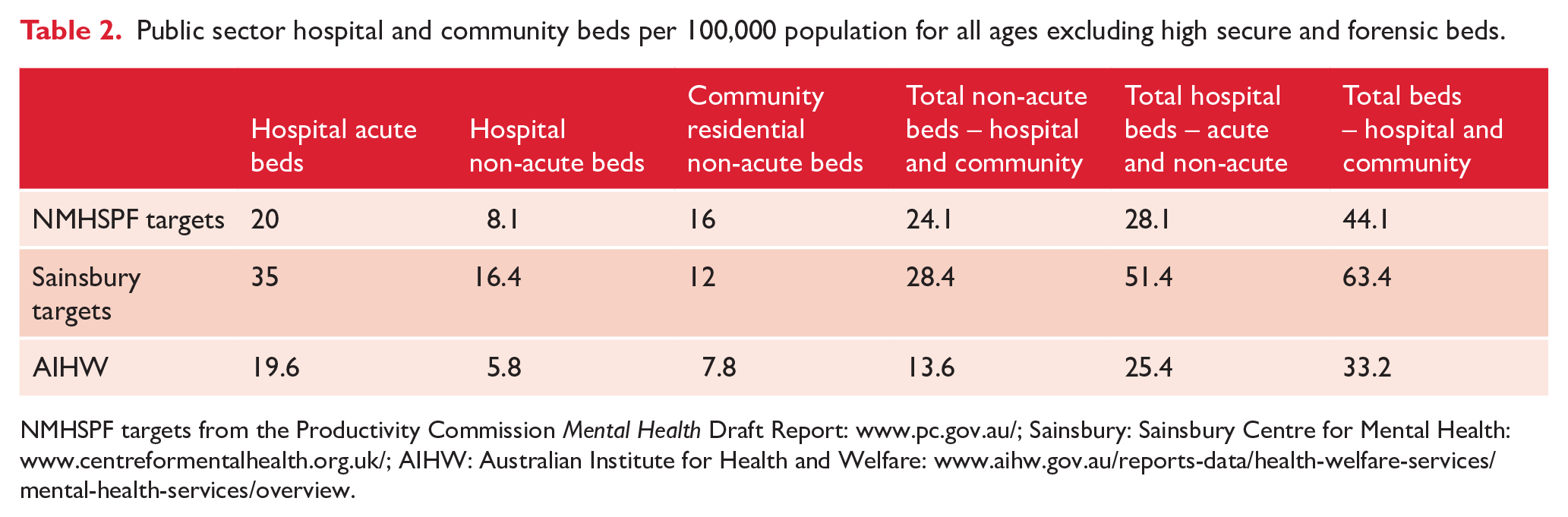
NMHSPF targets from the Productivity Commission Mental Health Draft Report: www.pc.gov.au/; Sainsbury: Sainsbury Centre for Mental Health: www.centreformentalhealth.org.uk/; AIHW: Australian Institute for Health and Welfare: www.aihw.gov.au/reports-data/health-welfare-services/mental-health-services/overview.
The observed outcomes approach for calculating psychiatric bed numbers proposes, ‘varying access to psychiatric beds has observable effects on health systems and populations’ (O’Reilly et al., 2019: 509). On this basis, if implemented, the NMHSPF higher targets for non-acute beds could reduce the cohort of complex long-stay patients on acute units, and thereby improve patient flow in general hospitals (Allison et al., 2020): this would be a major step in the right direction.
Instead of setting national benchmarks based on the NMHSPF targets, the Productivity Commission Mental Health Draft Report recommended regional service planning (Productivity Commission, 2019: 316, vol. 1). If this recommendation is accepted by Australian Governments, we contend that States/Territories should, as part of their mandate, ensure that local services have sufficient access to hospital and community non-acute beds, so they can provide long-term care, and help relieve the pressure on general hospitals by reducing the cohort of long-stay patients on acute units (Allison et al., 2020).
While both WHO data and the NMHSPF modelling strongly suggest that Australia has too few non-acute beds, further study is needed. International comparisons of bed numbers are complex due to differences in private sector capacity, the types of beds funded, and populations admitted. The Productivity Commission also warned against international comparisons, if ‘such a simple calculation overlooks cross-country differences in health systems and data definitions’ (Productivity Commission, 2019: 315, vol. 1). Hence, there is scope for Australian Governments to fund detailed research on cross-country differences in acute and non-acute care.
Conclusion
Australia’s bed modelling has been based on the premise that the nation needs fewer beds per capita than other high-income countries, but real-world ED data suggest otherwise. The NMHSPF’s higher targets for non-acute beds are welcome, but the 80%/20% allocation of community to hospital beds is debatable. The public interest would be well served by greater transparency about the NMHSPF’s algorithms, since they form the basis for major government decisions. Until the Commonwealth makes the NMHSPF materials fully available however, its targets can be benchmarked against other expert consensus recommendations, international medians, and the observed outcomes of low-bedded systems. On this basis, we argue that the NMHSPF’s targets are still too low, so if implemented they may fail to rebalance the system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.