
Abstract

Depression comprises heterogeneous syndromes with multifactorial aetiology that result in varied clinical manifestations. This makes its treatment challenging (Malhi and Mann, 2018). In addition to psychological, lifestyle and social interventions, the mainstay of management involves antidepressant pharmacotherapy. Worldwide, nearly 30 antidepressant medications are available that draw on a variety of putative mechanisms of action. However, clinically, relatively modest differences in efficacy separate these agents, and hence prescription choice is usually based on tolerability and clinician experience. In addition, several psychological interventions have replicated efficacy in clinical trials but again this is insufficient to differentiate individual therapies.
In practice, approximately a third of depressed patients achieve remission in response to their first antidepressant treatment, and combining, augmenting or switching to another antidepressant is usually necessary to eventually attain remission in half of the remaining patients (Rush et al., 2006). This means that, overall, at least two-thirds of patients require several antidepressant trials to achieve remission, and, even then, many will need alternative treatments, such as psychosocial interventions or electroconvulsive therapy (ECT). In other words, despite the wide range of treatments available, poor response to antidepressants is common, and is once again attracting increasing attention.
Treatment-resistant depression
Although ‘treatment-resistant depression’ (TRD) is a widely recognised term, it is variably defined, and because of this it is a multifarious condition (Malhi et al., 2019). In research, its definition is usually predicated on sequential pharmacotherapy, but no clear consensus exists regarding how best to capture true treatment resistance in clinical practice. Recently, alternative approaches have been proposed in an attempt to broaden the scope of the term, such as ‘difficult-to-treat depression’ (DTD), but even here the focus remains much the same, i.e., non-response (McAllister-Williams et al., 2020). Curiously, even though response refers to clinical improvement in the context of treatment, and a ‘failure to respond’ is clearly not a characteristic of the illness per se, the term is still often used to refer to the disorder as if it were a property of the underlying ‘disease’. In rare instances, this may indeed be the case, such as selective responsivity to ECT where there has been a failure to respond to pharmacotherapy and psychological interventions. However, the focus of this article is not to better define TRD, nor to find a more suitable substitute based on non-response, but rather to alter the focus that this term (non-response) creates – namely, the ‘non-response perspective’, in which discussion gravitates towards negative outcomes and a failure to improve.
Instead, we argue that the term ‘treatment-resistant depression’ is also problematic and nihilistic because it skews the management of mood disorders towards not responding to treatment. Indeed, its definition is predicated on enumerating antidepressant response failures—a rather arbitrary means of delineating a condition, and this attaches undue importance to what does not work rather than what might work.
Therefore, we propose an alternative perspective, one in which the ‘illness’, namely depression, is regarded as an aggregation of components that will eventually respond to treatment, but do so differentially, and in response to specific treatments. This allows for very many components of the overall depressive presentation, including psychosocial factors and features of personality, to be addressed in formulation, management and treatment planning. Furthermore, this alternative perspective allows for these various overlapping components to co-exist and work alongside each other, both in sequence and in parallel. Fundamentally, it changes the perspective to one of treatment response. And this approach is superior because it places greater emphasis on a potential positive outcome while maintaining a realistic perspective of the complexity of depression. It also acts as a constant reminder that there are many potential pathways to achieving a response.
Focusing attention on response also obviates the need for having a threshold for non-response. Instead, it is implicitly understood that if one treatment pathway is insufficient, an alternative will need to be trialled. This may be an incremental change, or it may entail a paradigm change; for example, moving from a selective serotonin reuptake inhibitor (SSRI) to its augmentation with lithium, or switching entirely to a dual-acting agent or another mode of treatment, such as ECT. All of these options are viable possibilities, provided they are suited to the patient, their individual circumstances and the nature of their illness.
Changing perspective
To illustrate our proposed paradigm in which we switch the primary focus to treatment response, we provide a schematic in which response to treatment is envisaged as a journey through a channel from a state of depression to that of recovery. In order to traverse the channel, a treatment (pathway) that successfully facilitates the ‘journey’ to recovery has to be identified.
In the beginning, a particular mood state may be amenable to any number, or indeed all types of treatments. Some pathways may be more effective than others, and in some instances, combinations of different treatments may prove to be more successful than singleton measures, either by shortening the journey or accelerating progress. Conceptualising the treatment of depression in this manner and assigning primacy to response allows full and proper consideration of the wide range of available treatment options and shifts the focus towards achieving a positive outcome. It also allows for considering a number of alternatives that can be sequenced accordingly.
In practice, with this perspective in mind, depression can be defined in therapeutic terms. For example, one might consider whether a therapeutic channel that involves psychological interventions is appropriate, and, if so, whether this will also require pharmacotherapy in combination. Within psychological interventions different forms of therapy (e.g. schematic cognitive behavioural therapy [CBT], mindfulness or acceptance and commitment therapy) or different therapists (noting the ‘patient/therapist fit’) might be usefully considered. The same can be applied to pharmacotherapy, where specific treatments can be trialled – either classes of antidepressants, e.g., SSRIs, serotonin and norepinephrine reuptake inhibitors (SNRIs) and tricyclic antidepressants (TCAs), or individual agents within a particular class, noting that the dose of agents can be increased to tackle specific symptom patterns. Certain channels may contain additional strategies such as augmentation with lithium or an atypical antipsychotic and, similar to the manner in which the illness can be tailored to psychological and pharmacological therapies, so too it can be appraised in order to see whether ECT is a suitable option. When viewed in this manner through the perspective of response, depression can be constructed as a composite of overlapping treatment-responsive units. Importantly, these ‘units’ of treatment response are not mutually exclusive. In essence, they reflect the responsivity and sensitivity of aspects of the illness to different treatments. Clinically, this is helpful because it reinforces the idea that the illness will respond to various interventions and that these may facilitate and/or accelerate improvement at different times.
Adoption of this ‘response perspective’ changes the conversation to one of seeking an appropriate treatment (one of several options) and makes it clear that many alternatives are available. The purpose of management thus shifts to opening doors (channels) rather than closing them. This is likely to be enormously beneficial as it alters the dialogue towards one of hope and possibility, as opposed to re-enforcing non-response and reminding everyone that there has been a failure to improve. Changing to a response perspective has the additional advantage of bringing together different treatments within one model. It illustrates that the goal, and the steps that need to be taken to achieve this, are the same, irrespective of which pathway is selected. For example, the ultimate goal of functional clinical improvement is independent of whether a psychological intervention, a medication or a physical treatment is employed. Importantly, adopting this perspective also allows response to be conceptualised as occurring across modalities, for example, CBT facilitating the antidepressant response of medications and vice versa, acting analogous to a catalyst or channel opener. It also suggests that, ultimately, different responses may converge upon the equivalent of second-messenger systems that then produce similar changes within the architecture of the brain.
Channelling response
Figure 1 shows the various available pathways for treating depression. In this depiction, the journey from depression to that of functional recovery can be made through any number of channels, as shown, and it is possible that, in any individual case, all the channels or indeed none of them are available. In other words, a particular depression may or may not be amenable to all types of treatments and this clearly depends upon its specific nature (e.g. its unique aetiology and pathogenesis). Put simply, different kinds of depression have different ‘channels’ available for response.
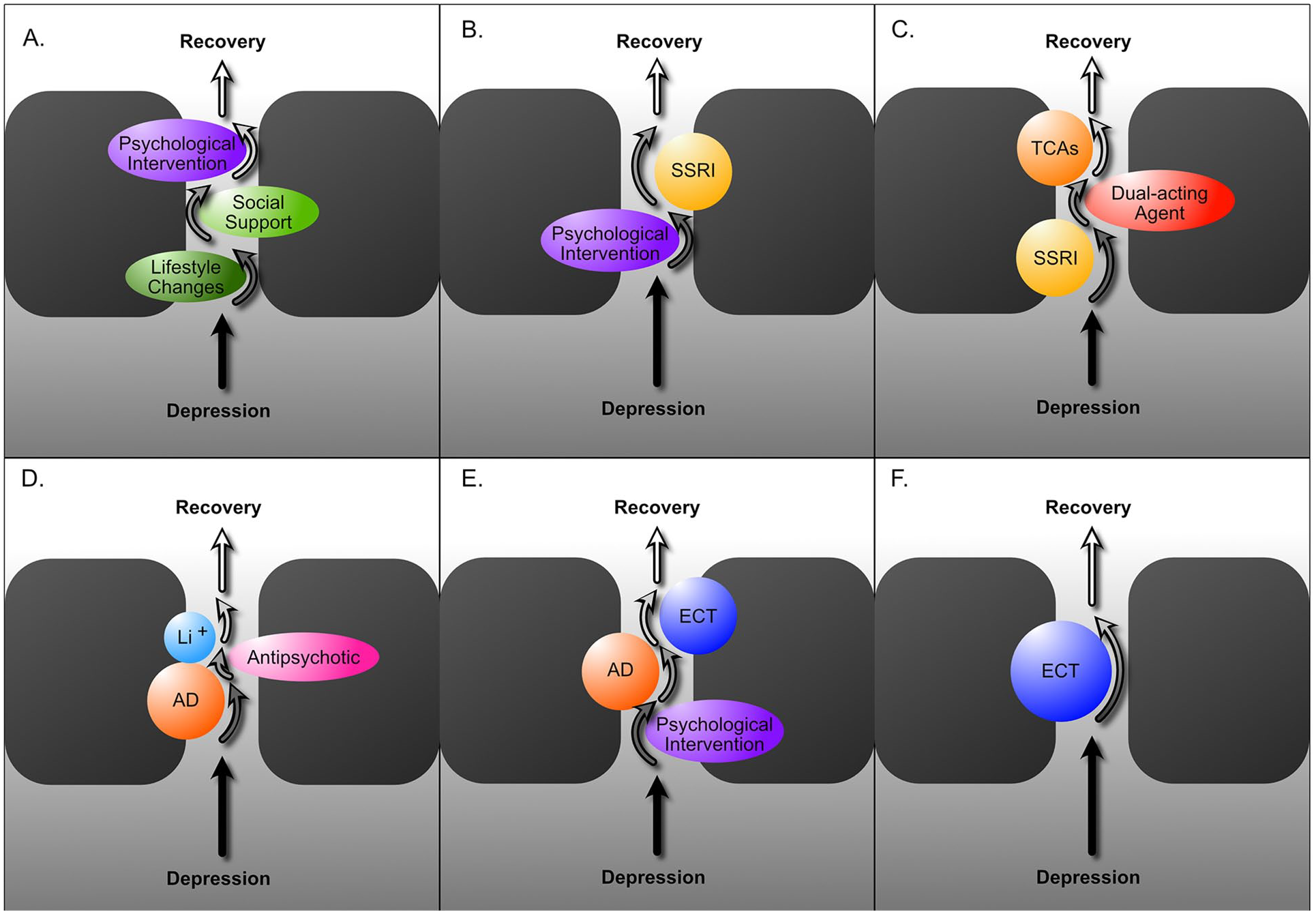
Therapeutic channels of response. This schematic illustrates examples of how different combinations or sequences of treatments may be needed to recover from depression; transitioning from a depressed mood state to one of functional recovery. Various treatments work individually or in combination to facilitate or speed up this transition. The effects of treatments (responses) are depicted as arrows. (A) Illustrates how a combination of instituting lifestyle changes, social support and psychological interventions (such as CBT) can be sufficient to facilitate recovery from depression in some cases. (B) Illustrates how the combination of a psychological intervention and an SSRI may be required for recovery. (C) Illustrates the sequencing of agents; an SSRI may be employed first, but this only achieves a partial response, and therefore this needs to be switched to a dual-acting agent before finally switching to a tricyclic (TCA) antidepressant so as to achieve complete recovery. (D) Illustrates the use of lithium to augment the effects of an antidepressant (AD) in combination with an antipsychotic. The combination of an antidepressant and an antipsychotic may produce a partial response, but the additional augmenting effect of lithium is needed for full recovery. (E) Illustrates a pathway in which a combination of a psychological intervention and an antidepressant achieve a partial response, but ECT is required for full recovery. (F) Shows a response for which ECT is necessary to achieve recovery.
In the figure, the first channel illustrates how different types of treatments or different strategies can be used in combination as needed to achieve remission and recovery. The juxtaposition of a psychological therapy alongside an antidepressant (Figure 1(B) and (E)) reinforces evidence-based recommendations, which suggest that a combination of psychological and pharmacological approaches is the most effective strategy. This is because, in practice, patients generally prefer psychological interventions and, when administered alongside pharmacotherapy, they usually enhance treatment adherence. In a similar vein, treatments can be sequenced from psychological plus pharmacotherapy to physical treatments such as ECT (Figure 1(E)). However, depending on the type of depression, its clinical profile, past treatment history and sensitivity, it is possible that some kinds of depression are only responsive to ECT (Figure 1(F)). This is particularly likely when the depressed patient has mood-congruent psychotic symptoms and/or marked melancholic features.
Given the very many antidepressants available, there are of course very many possibilities both for monotherapy and combinations of medications. And therefore there are numerous strategies that hold potential for a response. Commonly, a partial response may be achieved with a course of antidepressant treatment (e.g. an SSRI), but the response then requires augmentation with lithium or an antipsychotic to achieve full remission (see Figure 1(D)).
The key point of having a multitude of possible therapeutic combinations, however, is that the focus of treatment remains on responsivity. And therefore, clinically, it is important to identify and think of the kind of treatment the depressed person is likely to respond to, rather than being concerned about not achieving a response. The narrative, therefore, changes to that of depression being a composite of different therapeutic responses that are psychological, pharmacological and physical. Many of these responses are overlapping and linked such that response in one domain may facilitate and unlock response in another. This is another important concept which may explain why there are synergies between different kinds of treatment that are achieved through mechanistic linkages. The response perspective also assists both patients and clinicians to understand the importance of prescribing treatments in an orderly and deliberate manner with specific purpose. This approach can also help improve communications between clinicians regarding their descriptions of patients, and their shared expectations of how patients may fare with alternative treatments. The implicit impact of communicating that a patient is inherently treatment resistant can have a damaging and lasting effect in shared communications between clinicians, for example, when making and receiving referrals – prematurely labelling them as difficult to treat and refractory to therapy.
Our proposed responsivity model, therefore, removes the need to focus on treatment resistance, or to consider depression as ‘difficult to treat’ (DTD). Both these concepts (TRD and DTD) are clinically unhelpful because of their negative connotations. Instead, in the responsivity model, depression is regarded as having the potential to respond throughout management and is not regarded as being unnecessarily challenging. In fact, it suggests that only if a clear cause for non-response is found, such as an organic illness, is there a need to accept the possibility of a poor outcome. In this frame, only truly refractory depression is regarded as being treatment resistant. However, even in refractory cases of depression where no clear cause for non-response is evident, the adoption of a responsivity perspective can help.
Conclusion
By changing the focus of antidepressant treatment to therapeutic response, we propose a paradigm change in the management of depression. The change in perspective allows the identification of treatment pathways (channels of response) and removes the need to prematurely designate patients as treatment resistant. This change in perspective allows depression to be regarded as a composite of responsivities, and by drawing on receptor channel concepts, we allow for a more logical formulation of treatment strategies that ensure a positive therapeutic focus is maintained throughout management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. P.B. has received research support from the National Health and Medical Research Council, speaker fees from Servier, Janssen and the Australian Medical Forum, educational support from Servier and Lundbeck, has been a consultant for Servier, served on an advisory board for Lundbeck and has served as DSMC Chair for Douglas Pharmaceuticals. M.H. has received grant or research support in the last 5 years from the National Health and Medical Research Council, Medical Research Future Fund, Ramsay Health Research Foundation, Boehringer-Ingleheim, Douglas, Janssen-Cilag, Lundbeck, Lyndra, Otsuka, Praxis and Servier and has been a consultant for Janssen-Cilag, Lundbeck, Otsuka and Servier. R.M. has received support for travel to education meetings from Servier and Lundbeck, speaker fees from Servier and Committee fees from Janssen. R.J.P. has received support for travel to educational meetings from Servier and Lundbeck and uses software for research at no cost from Scientific Brain Training Pro. E.B., D.B., R.A.B., B.L. and A.S. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.