
Abstract

To the Editor
Billig (1982) described the role of a liaison psychiatrist integrated in an intensive care unit (ICU) in Georgetown, United States, as psychopharmacological consultant, patient ombudsman, staff support consultant and teacher.
The conventional model for providing psychiatric clinical services to an ICU is through referral to a centralised hospital-wide consultant-liaison (C-L) service. Reasons for referral of 122 ICU patients to such an Australian general hospital C-L service included depression (16.4%), suicide risk (11.5%), psychosis (10.7%), ‘psychological component’ (9.8%), coping problems (9%) and behaviour management (5%). Of those referred, 64.7% had been admitted for overdose. Interventions included medication review (63%), suicide risk evaluation (59%), behaviour management (7.4%) and end of life or competence assessment (4.9%) (Devasagayam and Clarke, 2016).
Since Billig (1982) one study compared the latter conventional C-L model with a psychiatrist embedded in daily ICU rounds (Bui et al., 2019). For the intervention (embedded) group, consultation rates were higher (p < 0.001) and time to psychiatric consultation shorter (3.19 days embedded group; 7.48 days controls; p = 0.004). There was a non-significant trend for shorter hospital length of stay in the embedded group, reaching significance in a respiratory failure subgroup. Embedded model advantages included immediate availability of a psychiatrist to weigh in with and implement in real time, treatment recommendations for a range of conditions including delirium, anxiety, substance use, adjustment disorders, depression, bipolar illness and psychosis.
In this letter, we report our experience with the embedded model. In April 2019, a liaison psychiatrist employed 0.4 Full Time was appointed to our 46-bed ICU, employed by the ICU, embedded within ward rounds and working inside the unit during working hours. The role, dynamic and responsive to service needs, has evolved to that described by Billig (1982) that is, as clinician, staff support/welfare psychiatrist and teacher. With regard to the clinical role, we describe 50 consecutive referrals between April 2019 and January 2020 (Table 1). Time from referral to patient assessment was 15–120 minutes, the variation attributable to the fact that not all referrals were made during ward rounds. Transfer from ICU post assessment for self-harm ranged from 4 to 18 hours, and length of stay considered an important outcome measure potentially related to proactive psychiatric consultation (Bui et al., 2019).
Description of 50 consultations to an ICU liaison psychiatrist.
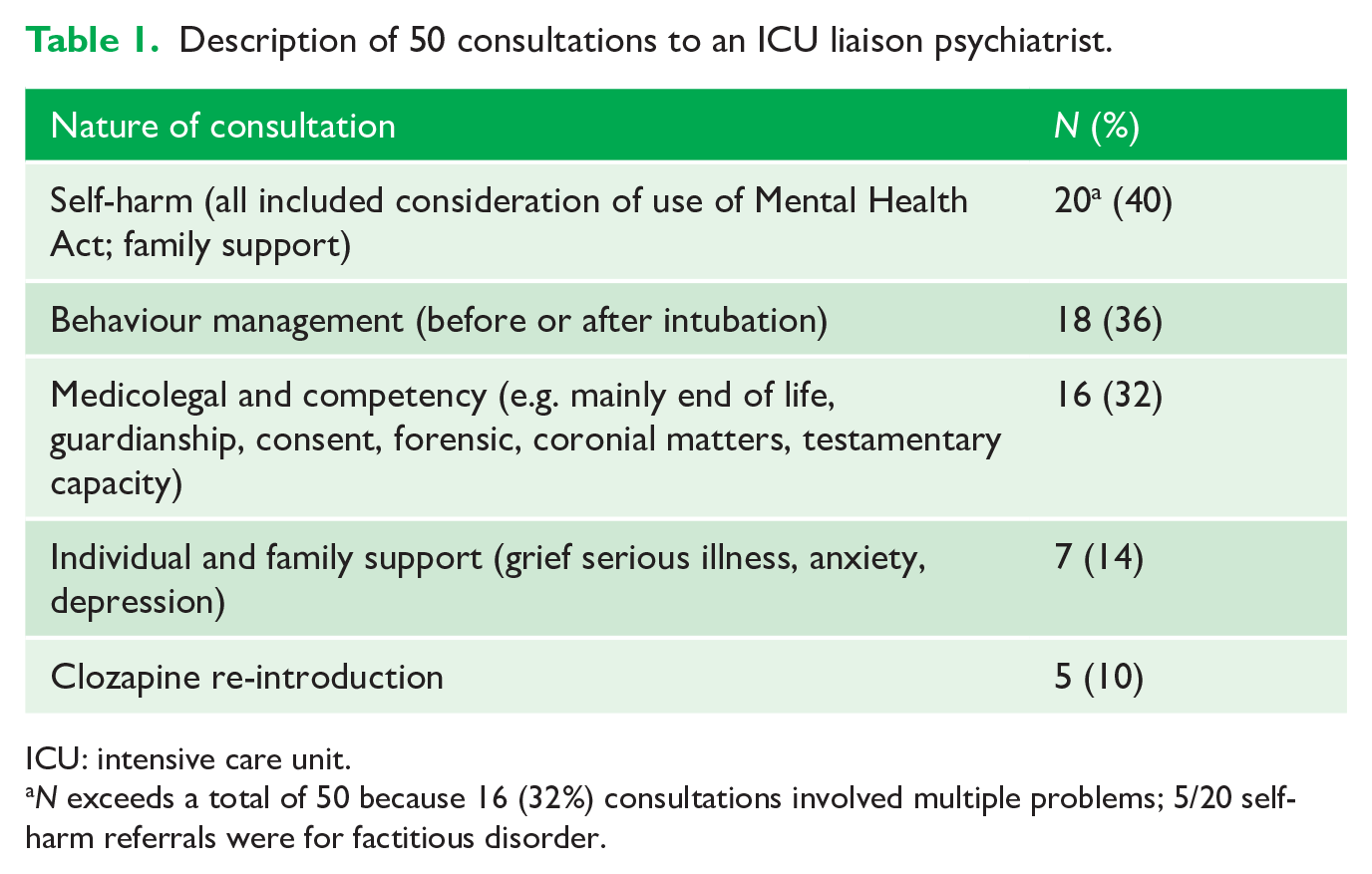
ICU: intensive care unit.
N exceeds a total of 50 because 16 (32%) consultations involved multiple problems; 5/20 self-harm referrals were for factitious disorder.
Similar to Bui et al. (2019), we found that psychiatric presence allowed problems to be dealt with in real time, bridging gaps between the perceived problem and multiple potential psychiatric interventions. Consistent with the conventional service described above, delirium was never identified as a reason for referral. However, behavioural interventions far exceeded (36%) that of the conventional service (7%) suggesting extra opportunities offered by this model for psychiatric intervention for delirium and agitation. Moreover, while more medicolegal and competency referrals (including end-of-life issues) may have reflected the psychiatrist’s expertise, it is long-held that end-of-life disputes frequently play out in ICU settings (CRELS, 2010). Such disputes have been precipitants for several Common Law cases (e.g. Messiha v South East Health [2004] NSWSC 1061).
The staff welfare and support role required engagement and being part of, not a visitor to the team. Multimodal systemic interventions included facilitated communication with 360 degree feedback at individual and group levels with both nursing and medical staff. These were co-led by the Liaison Psychiatrist (Family Systems Therapist), an ICU Advanced Trainee Welfare Champion and the Medical Director (Intensivist). A range of resources were developed including a Code of Conduct developed by staff for staff and informed by the medical impairment and well-being literature, with key themes of communication, respect for self and others, recognising lack of omnipotence and vulnerability to impairment. A Medical Crisis Intervention Help document provided a step-by-step guide for dealing with impairment with resources, contact numbers and information regarding mandatory reporting. Anger and Conflict Management and International Medical Graduate Support programmes were developed in response to identified issues in relation to medical culture. A debriefing model used elsewhere in the District was also identified. These resources have since been disseminated across the District as well as to other services across Australia.
ICU is a unique clinical environment, serving patients with life-threatening illness, at high risk of psychiatric symptomatology, supported by families for whom death and dying is traumatic and conflict-engendering, cared for by staff at risk of distress and burnout. Why wouldn’t a psychiatrist be of assistance, particularly in this new COVID world of which ICUs are at the centre?
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.