
Abstract

A young disorder of the very young
Historically, bipolar disorder (BD), which is defined by mania, was thought to emerge during late adolescence or early adulthood. However, over the last twenty years, the diagnosis has increasingly been applied to children who have presented with various degrees of elated mood, increased irritability and energy, mood lability, decreased need for sleep and constant engagement in goal-directed activity. These putative ‘manic manifestations’, when occurring in children, have been labelled as paediatric bipolar disorder (PBD) – a diagnosis that has long been a topic of controversy among researchers and clinicians alike.
Initially, this ‘early onset’ variant was regarded as relatively uncommon. However, in the 1990s, after gaining favour amongst clinicians, the prevalence of PBD increased considerably, especially in the United States (Moreno et al., 2007). Therefore, this Make News article examines this contentious diagnosis and considers its consequences when applied to children.
Rationale
Interest in the onset of bipolar disorder in children and adolescents is logical given that many adults with BD report experiencing symptoms in their younger years, and if prevention is to be achieved then understanding the inception of the illness is likely to be of benefit. Furthermore, research has shown that in those that have an early onset of BD, the illness is more chronic and more severe as compared to those in whom the symptoms emerge much later in life. Therefore, early and accurate detection and diagnosis of mania, and timely intervention, are likely to reduce the prevalence of BD and improve outcome.
Hence, interest in identifying earlier phenotypes of BD is justified. But the rapid upsurgeance in the prevalence rates of PBD raises questions as to, firstly, whether this diagnostic label is truly being applied appropriately, and, secondly, what might be the potential clinical costs of the current approach.
Shifting sands
While clinically it seems plausible that BD manifests at an early age, the diagnosis of a mental illness that is equivalent to adult BD in children remains highly controversial. In addition, interpretations of what precisely characterises PBD have repeatedly shifted over the years, adding to the confusion surrounding the use of this diagnostic label.
For example, some research groups emphasise ‘severe irritability’ and ‘outbursts’ – nominating these as the defining features, while others posit that PBD is characterised primarily by ‘ultra-cycling’ affective episodes, similar to the concept of ‘mixed states’ in adult BD. Contradicting this, some longitudinal research has found that chronic irritability and continuous mood cycling do not reliably predict the subsequent emergence of BD (Shaw et al., 2005). Thus, at present, the DSM-5 criteria for the diagnosis of PBD in children, adolescents and adults are the same.
In order to longitudinally track a disorder (disease), having one definition with consistent criteria is ideal; however, whether the criteria that define adult BD accurately capture its paediatric form is debatable given that few experiences, if any, remain the same as an individual undergoes growth and development from childhood through to adulthood. Furthermore, it is evident that, when aiming to make a diagnosis of PBD, the symptoms used to describe mania are not meaningfully transposable onto the experiences and feelings of children and young adolescents. Indeed, many of the core symptoms that define mania in adults (e.g., being excessively cheerful, grandiose and having diminished insight) are, in fact, age-appropriate expressions and behaviours in children.
Another problem with the diagnosis of PBD is that is hinges on ‘irritability’ as a defining symptom. This poses difficulties because, in practice, irritability is a common feature of many childhood psychiatric disorders (e.g., oppositional defiant disorder, major depressive disorder) and is also readily influenced by attachment and environmental factors, such as sleep. Therefore, by resting the diagnosis of BD on developmentally inappropriate and transdiagnostic symptoms, the clinical assignment of PBD is inevitably non-specific. Added to this is the complexity of differentiating any ‘early symptoms of BD’ from normative development and common childhood comorbidities such as oppositional defiant disorder (ODD) and attention deficit hyperactivity disorder (ADHD).
A growing problem, at a time of growth
A meta-analysis of epidemiological studies that included both broad and more stringent criteria for PBD (Van Meter et al., 2011) suggested a prevalence of 1.8%, but a more recent examination of these epidemiological studies by Parry et al. (2018) that took into account methodological differences, concluded that the prevalence estimate of PBD was significantly lower than this in both the USA and non-USA countries. However, in practice, the rates of children presenting to inpatient and outpatient settings with PBD have continued to grow (Moreno et al., 2007) and the widespread uptake of the diagnosis casts doubt on previous research that has suggested that childhood BD is relatively uncommon. So, what is the reason for the proliferation of this diagnosis?
While it is possible that the increase in PBD may be a result of reduced stigma and increased awareness of psychiatric problems in childhood, the suggestion that diagnostic inflation may be partly driven by economic and accessibility considerations is particularly concerning. In the USA, for example, a diagnosis of BD facilitates access to treatment and is therefore more ‘attractive’ to families compared to formulations such as child-parent relational problems, or externalising disorders. Clearly, if children are being ‘diagnosed’ with PBD in order to access treatment, this is a grave concern – not only for the individuals involved who are being incorrectly managed, but also for the field as a whole, as it distorts the statistics of the problem and creates meaningless data as regards prevalence, trajectory and treatment response.
Treating well
Regarding treatment, PBD is often managed using medications that have been developed for the management of established bipolar disorder. In other words, these medications that target symptoms in adults as part of the mature form of the illness have not been designed for use in children, and both their effects, acute and long term, in this age group are unknown. Furthermore, there is no evidence that these medications have any preventative effects, especially on the developing brain, and instead they may in fact cause significant harm – both at the time of administration and later on in life. For instance, despite some evidence for the efficacy of olanzapine and fluoxetine in combination for the treatment of acute depressive symptoms in PBD, and for quetiapine in the treatment of acute manic symptoms (Atkin et al., 2017), the longer term use of these medications causes substantial weight gain, hormonal changes and increases in cholesterol levels. These are significant side effects. Furthermore, given that the critical process of synaptic pruning occurs throughout childhood and adolescence, the potential deleterious consequences that psychotropic medications have on the developing brain are also a major concern. Thus, overall, given the lack of diagnostic clarity around PBD and the increased likelihood of false positives when diagnosis is based on cross-sectional and non-specific symptoms, there is a risk that many children may undergo unnecessary treatment and suffer significant side effects.
The importance of being earnest
Diagnoses in psychiatry are important for guiding clinical management and informing research. However, because of the difficulties associated with the diagnosis of PBD, the threshold for making this diagnosis should be high. Furthermore, because BD usually requires long term pharmacological management, it is even more important that the diagnostic label be applied with caution in children and adolescents. But, how then should we conceptualise suspected bipolar disorder in young people?
i.Clinical practice
Given the nebulous nature of PBD, we advocate for vigilance and a practical ‘wait and see’ approach to diagnosing children with suspected bipolar disorder. While we recognise the importance of providing clarity to children and families in distress, it is critical that clinicians first have clarity themselves about what constitutes PBD prior to issuing a diagnostic label that is likely to prompt the prescription of medications; especially as these are likely to produce more harm than benefit. Instead, it is perhaps more useful to monitor the specific symptoms the child is experiencing – many of which will not reach the diagnostic threshold for mania or depression until adulthood – and, where possible, consider non-pharmacological means of management instead (see Figure 1).
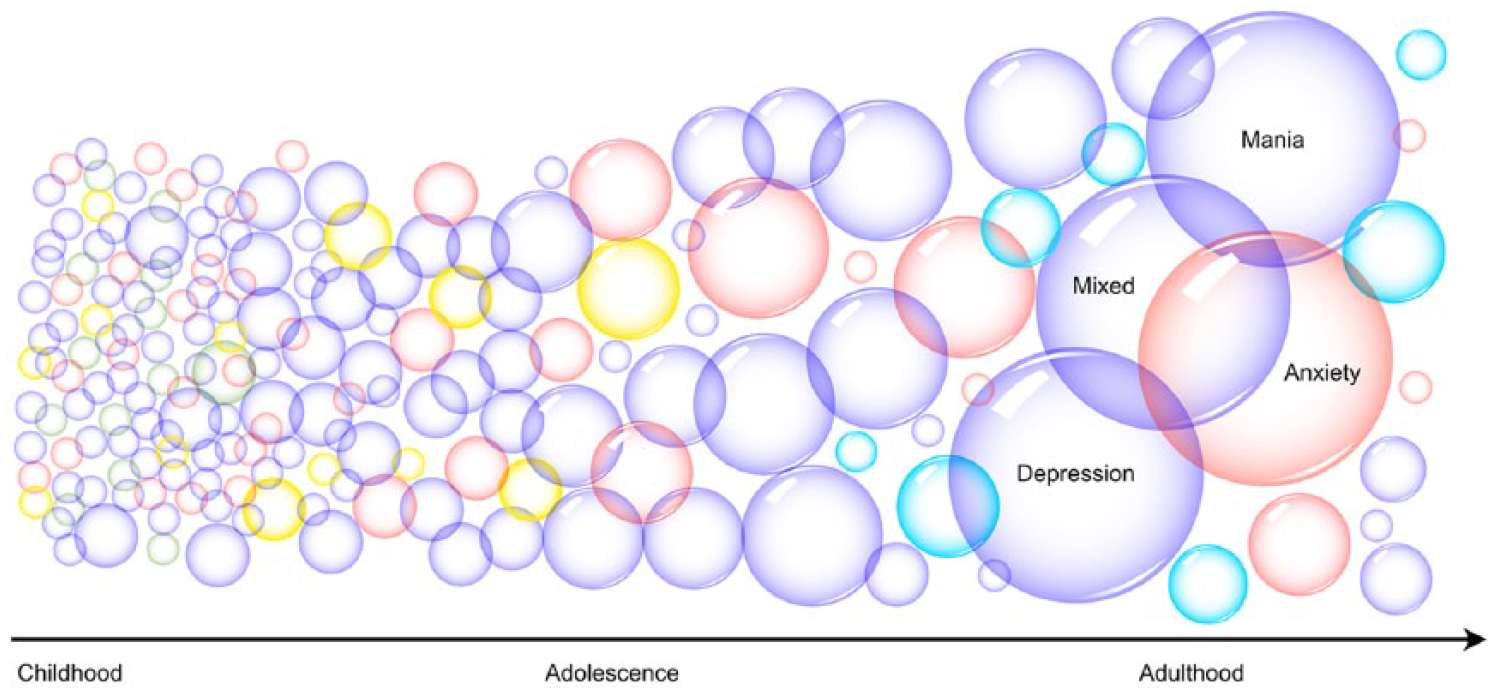
The coalescence of symptoms into syndromes and diagnoses through childhood and adolescent development. An illustration of the potential continuity of symptoms (small bubbles) from childhood through to adolescence and adulthood, shows that, as individuals develop, the grouping of symptoms into syndromes becomes clearer, and eventually diagnoses can be made. However,even in adulthood recognizable syndromes/diagnoses (large bubbles), such as mania, depression, mixed states (shown in purple) and anxiety (red), overlap to some extent and are not completely distinct. The figure also shows that some symptoms exist only in childhood (green) or extend only as far as adolescence (yellow) – meaning that in adulthood there are no equivalents of these symptoms. Conversely, there are symptoms in adults that are not evident in childhood (teal). Thus, it is inherently difficult to identify symptoms in childhood that meaningfully reflect adult symptomatology and equally challenging to track these symptoms through the inevitable changes that occur during adolescence.
ii.Research
Although premature at present, the goal of identifying an early phenotype of BD is an important pursuit. And given the myriad biological and psychological changes that occur from childhood to adulthood, researchers should remain open to the idea that PBD may have a very different clinical appearance to adult BD. Clearly, our initial imperative must be to develop a well-defined diagnosis that accurately captures the presentations encountered in clinical practice, rather than re-purposing an existing diagnostic label. To this end, longitudinal research is needed that tracks children reporting transdiagnostic symptoms from childhood through to adulthood and in so doing maps the emergence of bipolar disorder over this critical period of development. Concurrently, it is critical that research examines the underlying pathophysiology of these early presentations in order to understand the mechanisms that produce BD.
Conclusion
It is evident that bipolar disorder begins early, and that we need to identify its nature at its nascence. But until we know more about bipolar disorder in childhood and have a robust means of diagnosis, use of the term PBD should be abandoned.
Make News
In an age where good news and good ideas are difficult to find, this series offers constructive criticism of promising concepts in psychiatary in search of the truth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publica- tion of this article: G.S.M. has received grant or research support from the National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. EB, AH and GM declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.