
Abstract

Why staging?
In medicine, staging generally refers to the specification of a disease as having reached a particular ‘stage’ in its anticipated progression, and, clinically, it usually serves two main purposes. First, by establishing an understanding of the progression of an illness and by identifying discrete phases, diseases may be detected and treated earlier; and, second, by staging according to factors that determine progression, more targeted treatments can be developed and administered. These potential benefits, among others, have encouraged the concept of staging to be transposed from general medicine to mental disorders. But can staging be meaningfully applied to psychiatric disorders? It is this question that this Make News piece considers.
Staging cancer
In oncology, staging usually refers to the process of determining the size of a tumour, identifying its position and gauging whether it has spread. And, typically, it is undertaken after a diagnosis of cancer has already been made. For many types of cancer, staging involves a whole battery of tests and procedures (including the surgical removal of the cancer itself i.e. biopsy and/or complete excision), all of which aim to gauge the degree to which the cancer has spread.
For example, when staging bowel cancer, a colonoscopy is performed as part of the diagnostic process and blood tests can be used to screen for oncological markers such as carcinoembryonic antigen (CEA). Adjoining tissue and lymph nodes can be examined using an ultrasound, and radiological investigations (e.g. x-rays, CT scans and MRI scans) can be used to determine whether the cancer has spread to other tissues within the body. This information then forms the basis of a detailed staging system (referred to as TNM: tumour, node, metastasis) that is used to ‘quantify’ the disease (Compton and Greene, 2004). Such detailed assessment and classification of the cancer is important, because it provides an indication of prognosis, guides decisions concerning management and allows for the evaluation of therapeutic effectiveness. And thus, in oncology, it is evident that staging provides a very useful framework for both diagnosis and treatment. But can the same approach be usefully applied to psychiatry? Indeed, can psychiatric disorders be staged at all?
Are psychiatric disorders stageable?
Although self-evident, it is worth pointing out that psychiatric disorders are syndromes (i.e. collections of symptoms), and that they are not illnesses in the same way as bowel cancer is a disease. That is not to say that psychiatric disorders do not have an underlying pathophysiology that drives their clinical manifestation, but that, as yet, the exact nature of this is unclear. This is exemplified by the fact that the diagnosis and classification of psychiatric disorders, and the measurement of treatment response, are wholly dependent on clinical symptomatology.
The difficulties this poses for the staging of psychiatric disorders can be considered as three separate but overlapping problems (see Figure 1): (1) the phenomenal problem – that of having to rely solely on phenomenology, (2) the coupling problem – that of linking phenomenology and underlying pathophysiology and (3) the trajectory of change problem – that of determining the nature and direction of change in terms of both phenomenology and pathophysiology.

Staging problems.
A phenomenal problem: Our reliance on phenomenology for diagnosis is a significant barrier to staging because the definitions of most psychiatric disorders are imprecise, and, as a consequence, the clinical diagnoses they generate lack consistency. Critically, this means that psychiatric disorders cannot be regarded as diseases per se – even though they have been reified as such by taxonomic obdurateness, and their lack of diagnostic specificity and stability poses a major problem for staging as it makes extrapolation to the underlying pathophysiology of psychiatric presentations extremely difficult.
The coupling problem: The intrinsic nebulousness of psychiatric phenomenology is compounded by our limited understanding of how mental phenomena are coupled to underlying pathophysiology. The notion that clinical symptoms can be used to map the neural basis of a psychiatric disorder is an assumption that may not reflect reality. This is because for associations between the two domains (phenomenological and pathophysiological) to be useful, the nature of any coupling has to be reliable and bidirectional such that diagnoses connote specific pathology and pathological changes lead to a predictable clinical picture. However, as yet, no such connections (pathways) are known, and even with syndromes that have distinctive clinical features, such as mania, we lack any definitive biomarkers to which the syndrome can be tethered.
The trajectory of change problem: The third staging difficulty is that of mapping the progression of a clinical syndrome in terms of its underlying pathophysiology so that its course can be determined and its outcome anticipated. In other words, to gauge change and map the course of an illness, a reasonably predictable trajectory needs to be established. However, this is difficult as even marked psychiatric signs and symptoms may not signify pathology or provide any information as regards the direction in which a disease is progressing.
It is important to note that although these three problems have been described separately, they are very much linked, and this becomes evident when considering what is needed to stage psychiatric disorders meaningfully.
The nature of psychiatric disorders
Most severe psychiatric disorders are chronic lifelong illnesses in which the surfacing of symptoms is believed to reflect some kind of exacerbation within underlying pathophysiological processes. Presumably this is brought about by environmental stressors and general health factors. For instance, in bipolar disorder, episodes of depression and mania are described as periods of acute illness, whereas the intervening periods, where the individual is seemingly well, are described as euthymia. But even during these periods of ‘wellness’, the illness and its associated neurobiological changes are present throughout, and the illness never disappears per se (Malhi and Bell, 2019). It is important to bear this in mind, because it means that the pathophysiological progression of psychiatric disorders cannot be necessarily inferred by simply tracking clinical symptomatology (see Figures 2 and 3). This is similar to many inflammatory disorders where, for example, the disease process is ever-present, but the presenting symptoms vary considerably.
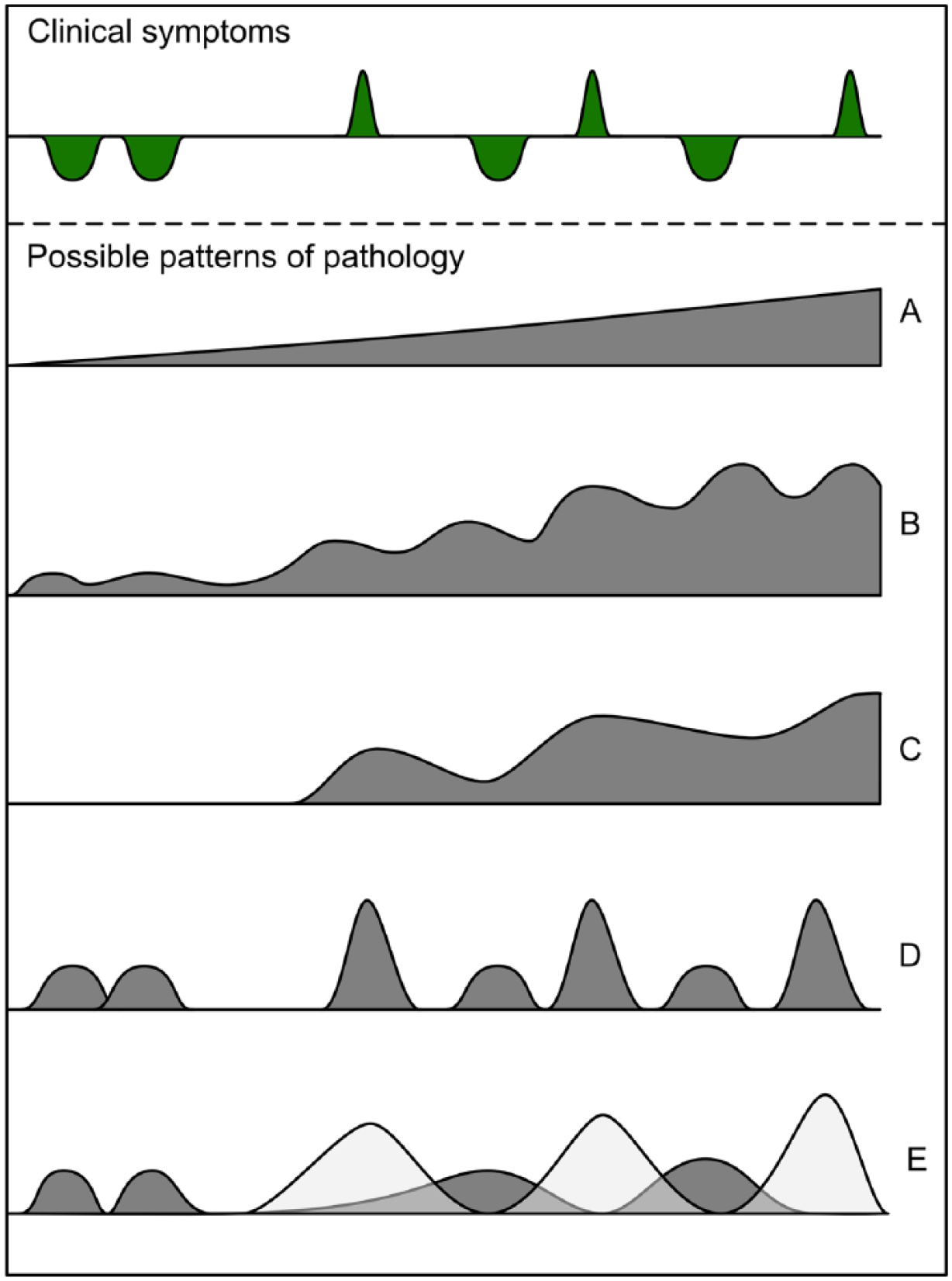
Comparison of clinical symptoms of bipolar disorder to potential patterns of pathology.
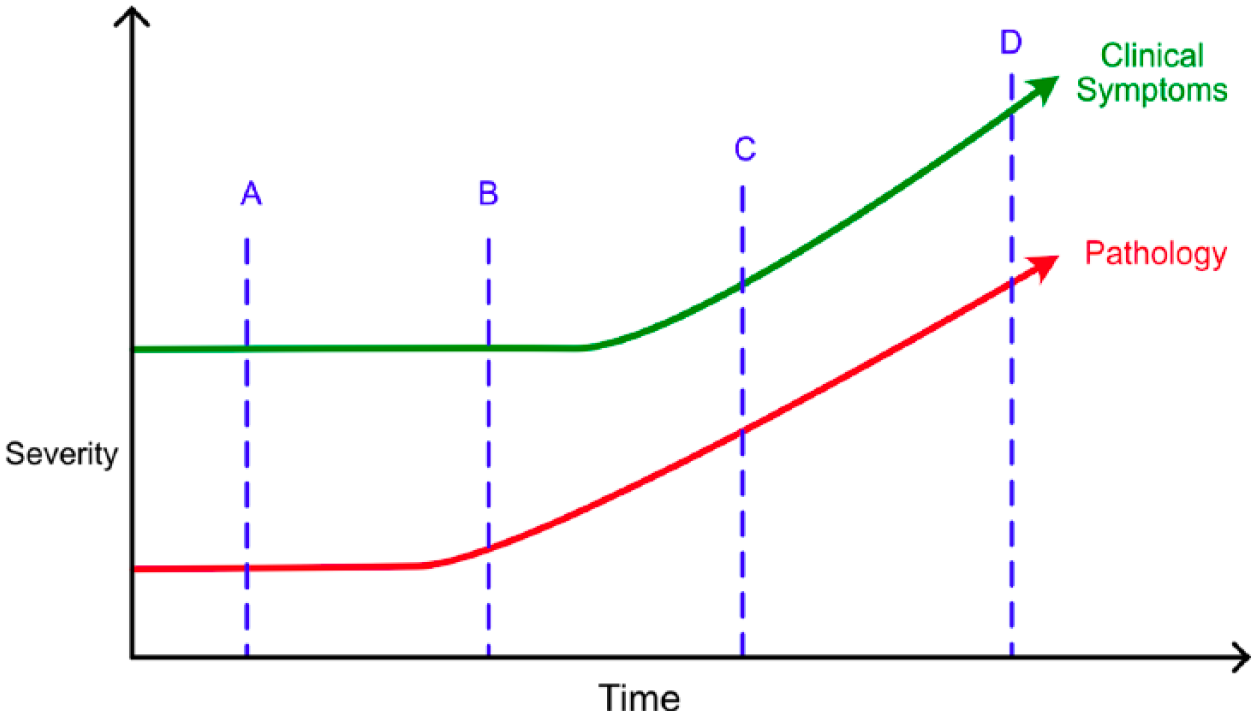
Relating clinical symptoms to underlying pathology.
However, for an illness to be staged, it has to progress along a pathway that can be mapped. And in its course, it needs to have discernible ‘components’ or ‘steps’ that reflect the development of the disease process and, at some level, signify a change in its underlying pathophysiology. However, psychiatric disorders may not have a predictable step-wise trajectory, and, perhaps by their very nature, the processes that drive psychiatric symptoms are devoid of any demarcations that denote the onset or offset of supposed ‘stages’. Indeed clinically, many psychiatric syndromes appear to be dimensional, suggesting that any underlying contributory processes may also be spectral in nature.
Another difference between psychiatric illnesses and medical diseases that further complicates staging is the critical role that psychosocial factors play in the development and maintenance of mental disorders. Trauma, life stressors, relationship and psychosocial difficulties contribute to the aetiology, pathophysiology and clinical outcomes of psychiatric disorders. These factors vary considerably, not only between individuals but even at different times within the one individual (Alloy et al., 2005), prompting once again the question – can psychiatric disorders be staged?
Pseudo-staging: the risks of staging psychiatric disorders
Our understanding of psychiatric illnesses is somewhat rudimentary, and therefore current staging efforts are perhaps more accurately described as ‘pseudo-staging’, especially given that they remain predominantly phenomenology-based, and, as such, lack a significant neurobiological foundation. However, this is not a merely semantic consideration because, in practice, the application of such pseudo-staging to psychiatric disorders poses significant risks.
For example, first, staging implies that psychiatric disorders develop in a step-wise (staged) manner and that the illness begins at some point with subtle but discernible changes. In practice, this runs the risk of elevating individuals who will only ever have short-lived sub-syndromal symptoms to ‘disorder status’ and encourages misdiagnosis. This is potentially stigmatising and may damage the self-efficacy of healthy individuals experiencing transient symptoms that are likely to be of no consequence in the long term. Second, because of the complexity and uniqueness of individual experiences, psychiatric disorders are vastly heterogeneous. As a consequence, grouping individuals with loosely similar psychiatric symptoms and referring to them as having reached a particular ‘stage’ of illness risks overlooking important differences. Furthermore, in this regard, the staging approach does not offer much of an advance over current diagnostic practices, which are also guilty of creating false (pseudo) categories.
With respect to research, the premature introduction of a staging model is likely to hinder future efforts, as it wrongly insinuates that we understand the development and trajectory of psychiatric illnesses. The reality is that, as yet, we do not have a deep understanding of many psychiatric disorders, and adopting an ill-fitting staging perspective runs the risk of failing to uncover the true nature (patterns) of these illnesses.
These considerations are also important for the treatment of psychiatric disorders because, in addition to providing greater diagnostic specificity, staging aims to provide an indication of the trajectory and response to treatment of illnesses. Thus, staging guides management – specifically, which treatment to utilise and what treatment response to expect. However, in psychiatry, we presently use a limited number of treatments throughout the course of a disorder, and many of these treatments are non-specific. Therefore, what therapeutic advantage can staging hope to provide if the management of psychiatric illnesses lacks diversity and remains the same? In other words, and more specifically, there is little point in making a distinction between various supposed ‘stages’ of a disorder if the treatment of the illness remains unchanged no matter what.
Furthermore, there are various factors that impact and shape what treatment may be best suited for a patient, aside from the putative ‘stage’ of their illness. Level of education and psychological literacy, a patient’s access to and quality of family support, and their motivation and willingness to engage and comply with therapy make treatment selection and response invariably more complex and unpredictable for psychiatric disorders as compared to other chronic medical conditions (Crowe et al., 2011).
Before taking the stage
We agree that, if staging were to be available for psychiatric illnesses, it would prove immensely useful for informing the progression and/or treatment of a disorder. However, at present, our limited mechanistic knowledge of psychiatric disorders means that this approach is premature, incomplete and lacks utility in directing treatment. In fact, before we can successfully stage psychiatric disorders, a number of key requirements need to be fulfilled. First, we need consistency and face validity of our diagnoses – that is to say, they have to reflect reality accurately and meaningfully. Second, the clinical course of psychiatric disorders has to be mapped – beginning with inception – such that clinical manifestations of an illness can be recognised at different points in its development, and in different contexts. This would also reveal to what extent psychiatric illnesses lend themselves to being staged, or whether they lie upon a continuum of severity and impairment that makes them more difficult to stage. Finally, treatments that modify symptoms and change underlying pathology with greater specificity have to be identified. In other words, they have to be stage-specific in order to be of benefit.
Only by having such measures in place are we likely to discover biomarkers that can help define both diagnosis and treatment response in terms of underlying pathophysiology and inform the development of a meaningful staging model.
Conclusion: exit stage left …
Before retrofitting a staging model to psychiatric disorders, substantially more research is required to understand exactly what it is that we are attempting to stage. Staging models must reflect the true nature and pathophysiology of a disorder in order to guide decisions concerning management and outcome. We submit that current staging models for psychiatric disorders do not fulfil these aims, and, as such, for the time being at least, are unlikely to provide any meaningful advance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.S.M. has received grant or research support from the National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. GM and EB declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.