
Abstract
To the Editor
Clozapine can cause gastrointestinal hypomotility, including severe constipation and ileus, which can lead to intestinal perforation (Every-Palmer and Ellis, 2017). These side effects are less well recognized than other clozapine-associated side effects, such as agranulocytosis (Every-Palmer and Ellis, 2017). Thus, we performed a systematic chart review to identify cases of intestinal perforation associated with clozapine treatment.
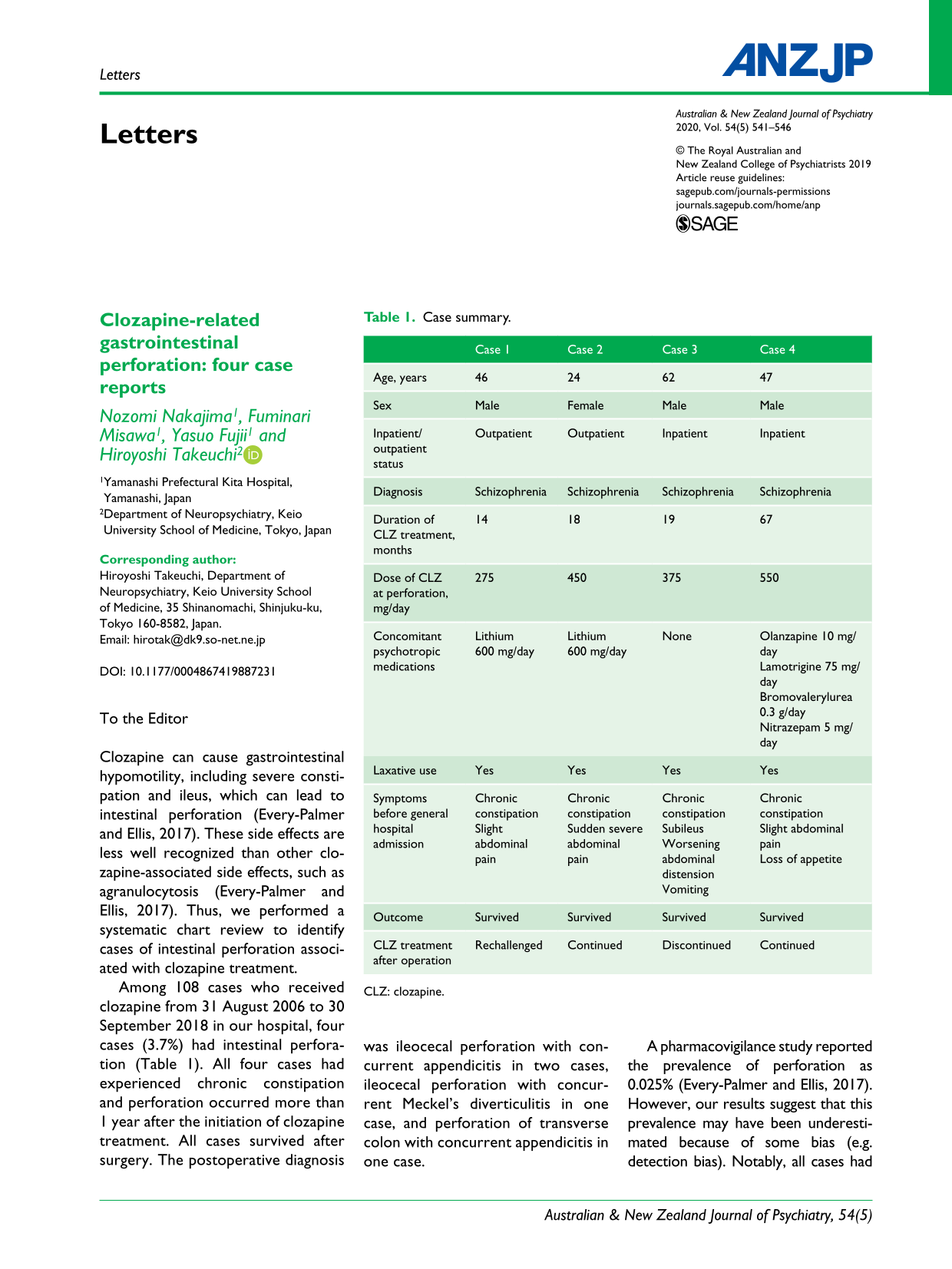
Among 108 cases who received clozapine from 31 August 2006 to 30 September 2018 in our hospital, four cases (3.7%) had intestinal perforation (Table 1). All four cases had experienced chronic constipation and perforation occurred more than 1 year after the initiation of clozapine treatment. All cases survived after surgery. The postoperative diagnosis was ileocecal perforation with concurrent appendicitis in two cases, ileocecal perforation with concurrent Meckel’s diverticulitis in one case, and perforation of transverse colon with concurrent appendicitis in one case.
Case summary.
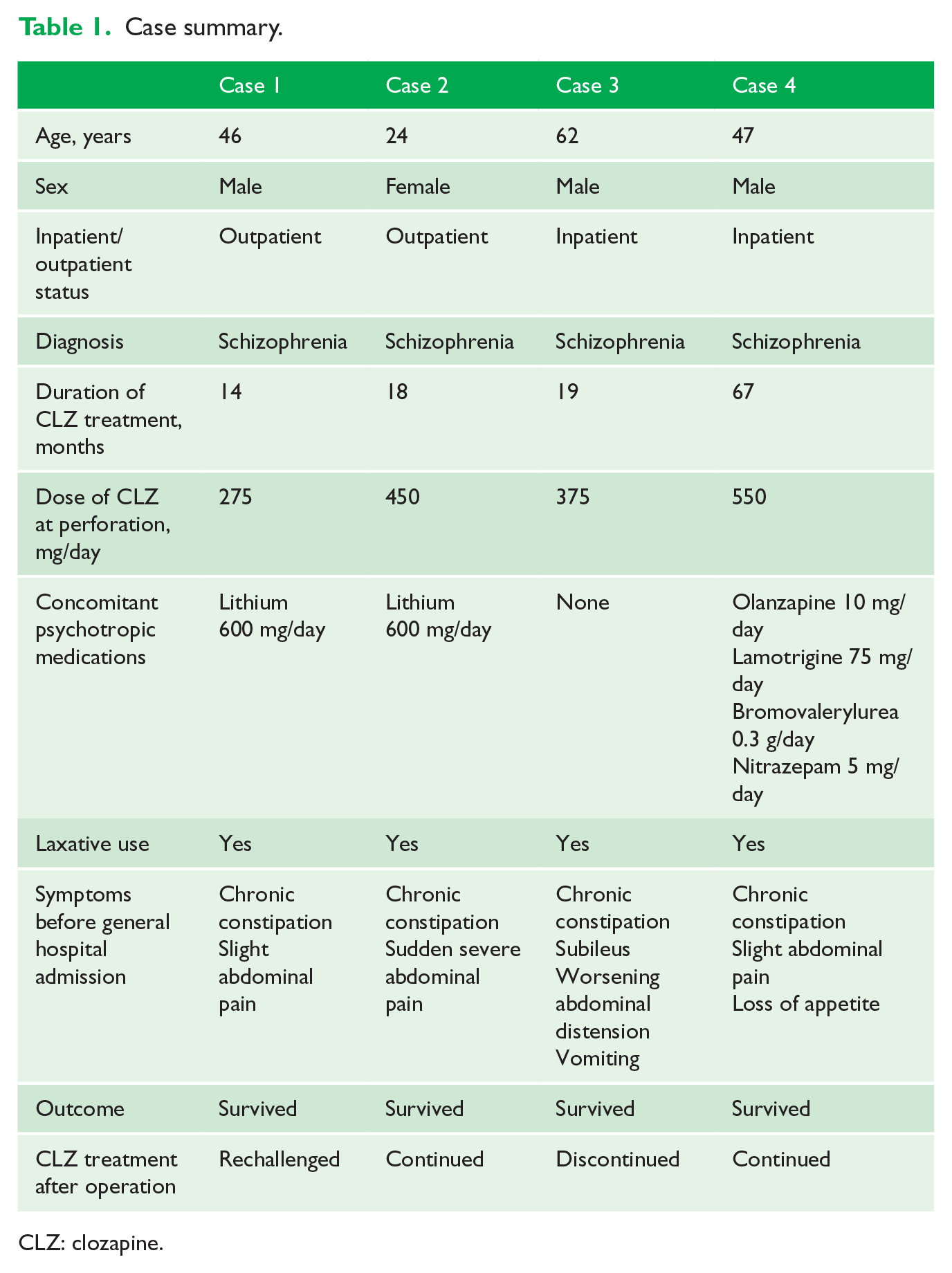
CLZ: clozapine.
A pharmacovigilance study reported the prevalence of perforation as 0.025% (Every-Palmer and Ellis, 2017). However, our results suggest that this prevalence may have been underestimated because of some bias (e.g. detection bias). Notably, all cases had inflammation in a blind-ending tubular structure such as the appendix or Meckel’s diverticulum, and three cases had perforation near the structure. We speculate that these cases indicate the underlying relationship among clozapine treatment, structural inflammation and intestinal perforation, although it remains unclear. Constipation due to clozapine can lead to fecal impaction (Every-Palmer and Ellis, 2017), which can result in increased colonic intraluminal pressure (Rodrigues et al., 2018). The increased pressure can cause structural inflammation such as appendicitis and cause mucosal ischemia and necrosis, which may induce intestinal perforation (Rodrigues et al., 2018). Moreover, inflammation can elevate serum clozapine levels (Haack et al., 2003) and may contribute to two vicious circles that accelerate the pathway to perforation: (a) clozapine has direct proinflammatory effects, further increasing serum clozapine levels and promoting structural inflammation; and (b) increased serum clozapine levels worsen intestinal hypomotility, a dose-dependent side effect of clozapine (Haack et al., 2003) leading to progression of inflammation, ischemia and necrosis via increased intraluminal pressure.
This is the first report suggesting that intestinal inflammation, including appendicitis, during clozapine treatment can be a serious side effect ultimately resulting in perforation. Clinicians should pay more attention to perforation after appendicitis during clozapine treatment, and further research is warranted to examine the relationship among clozapine treatment, intestinal inflammation and perforation.
Footnotes
Declaration of Conflicting Interests
Dr N.N. has no competing interests to disclose. Dr F.M. has received speaker’s honoraria from Eli Lilly, Janssen, Novartis Pharma, Otsuka, Pfizer and Sumitomo Dainippon Pharma. Dr Y.F. has received speaker’s honoraria from Janssen and Otsuka. Dr H.T. has received fellowship grants from the Canadian Institutes of Health Research (CIHR), Centre for Addiction and Mental Health (CAMH) Foundation, the Japanese Society of Clinical Neuropsychopharmacology and Astellas Foundation for Research on Metabolic Disorders; speaker’s honoraria from Meiji Seika Pharma, Mochida, Otsuka, Sumitomo Dainippon Pharma and Yoshitomiyakuhin; and manuscript fees from Sumitomo Dainippon Pharma.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.