
Abstract

In the beginning
Everything begins somewhere, and in the case of diseases, two key questions for researchers to identify are precisely what goes wrong and, equally importantly, when does this typically happen? The logic is that by understanding the processes that lead to pathology, the primary problems that cause diseases can be understood and a solution to fix them can be found. In theory, this seems simple, but in practice, it is not. Part of the difficulty is to have some initial inkling of where to look and what to look for. Un-fortunately, research has shown that most illnesses are not straightforward, and that single gene disorders and identifiable pathogens are the exception rather than the rule. Instead, the pathology of most chronic illnesses appears to be extremely sophisticated, with either many intertwined causal factors contributing to multiple illness pathways or many diverse aetiologies converging upon a common phenotype. This is especially the case for psychiatric illnesses where the quest for mechanisms underpinning the phenomenology of severe mental disorders has proven to be beguilingly challenging.
Nevertheless, even a complex, heterogeneous illness such as schizophrenia must have a beginning. After all, it is manifestly at variance from the experience of most healthy individuals, and so, there must be a point at which it first emerges and indeed diverges from normality. It is this belief that there is a prelude to the disorder commencing with an underlying pathological process that has kindled the concept of a prodrome. But concurrently, the lack of a neurobiological substrate has limited conceptualisation of the prodrome to phenomenology, and hence why prodromal models are centred on clinical symptomatology.
Schizophrenia
Regarding symptoms, schizophrenia typically features delusions, hallucinations and aberrant thought patterns that are then reflected in disorganised speech, but fundamentally it is characterised by functional decline. The active phase of the illness which comprises positive psychotic symptoms typically manifests during the third decade of life, and it is at this time that a diagnosis is usually conferred. However, onset can occur both much earlier (e.g. in adolescence) and much later in life (late-onset schizophrenia), and cases that present in youth are presumably foreshadowed by brain changes in childhood. But in practice, defining onset is difficult because although the symptoms of the illness are distinctive, their source remains obscure and the point at which they become established is often unclear. Thus, in the absence of known detectable pathology, the diagnosis remains dependent on functional parameters such as social withdrawal and decline in performance in daily activities, formal education and work.
Clinically, success in managing schizophrenia (an arguably low bar to begin with) is modest at best, especially once the illness becomes entrenched. And so, understandably, there is a growing urgency to identify the illness early with the expectation that timely intervention may improve outcomes, and it is this intent that has fuelled interest in the concept of a prodrome. Technically, the prodrome is the period that precedes an established psychotic illness, and typically, it consists of symptoms that represent a change from the individual’s premorbid functioning. But the concept is necessarily retrospective, that is to say it can only be defined in hindsight – once a diagnosis of a psychotic illness, such as schizophrenia, has been made. This is because, as yet, we have no reliable means of anticipating psychosis.
Prodrome
Retrospectively, up to 90% of patients with symptoms of schizophrenia describe emotional changes, and changes in perception and beliefs that have preceded the onset of their first psychotic episode (Yung and McGorry, 1996). However, it is important to note that 10–20% manifest psychotic symptoms precipitously without any identifiable prodromal period. In those that do have a prodrome, negative and non-specific symptoms emerge first and gradually give way to mild positive (attenuated) symptoms alongside a decrease in functioning and an increase in distress (McGlashan et al., 2010). In other words, nearly all patients with schizophrenia experience a prodrome – and this is significant. But the key question, and one of greater importance, is what proportion of those individuals that experience prodromal symptoms subsequently experience a psychotic episode and/or develop schizophrenia? This progression from prodrome to psychosis has been referred to as conversion, and to ascertain how often this occurs, and indeed how and why it occurs, researchers have posited the idea of high-risk syndromes.
In researching individuals that have experienced a conversion to psychosis, it has been demonstrated that the risk of conversion is highest in those that experience an increase in positive attenuated psychotic symptoms and accompanying distress (Yung et al., 2012). These individuals seek help for their distress and have therefore been invariably identified as being at high risk of psychosis. Several overlapping labels have been applied to this population, for instance, ultra-high risk (UHR), clinical high risk (CHR) and at-risk mental state (ARMS) (see Figure 1).

At-risk syndromes. Schizotypal traits (genetically linked to schizophrenia) increase the risk of psychosis as do isolated psychotic symptoms. But usually neither are accompanied by significant distress. In contrast, early and late prodromal and first-episode psychosis at-risk syndromes feature distress, but help-seeking separates those that are early-prodromal from late-prodromal. Hence, the latter form is the group that is of most interest, because it is those that seek help from physicians and mental health professionals that present clinically and undergo further research. This group is variably defined and referred to as ultra-high risk (UHR), clinical high risk (CHR) and at-risk mental state (ARMS). The figure also shows the domains to which attenuated psychosis syndrome is thought to apply.
Attenuated psychosis syndrome
A presumptive diagnosis?
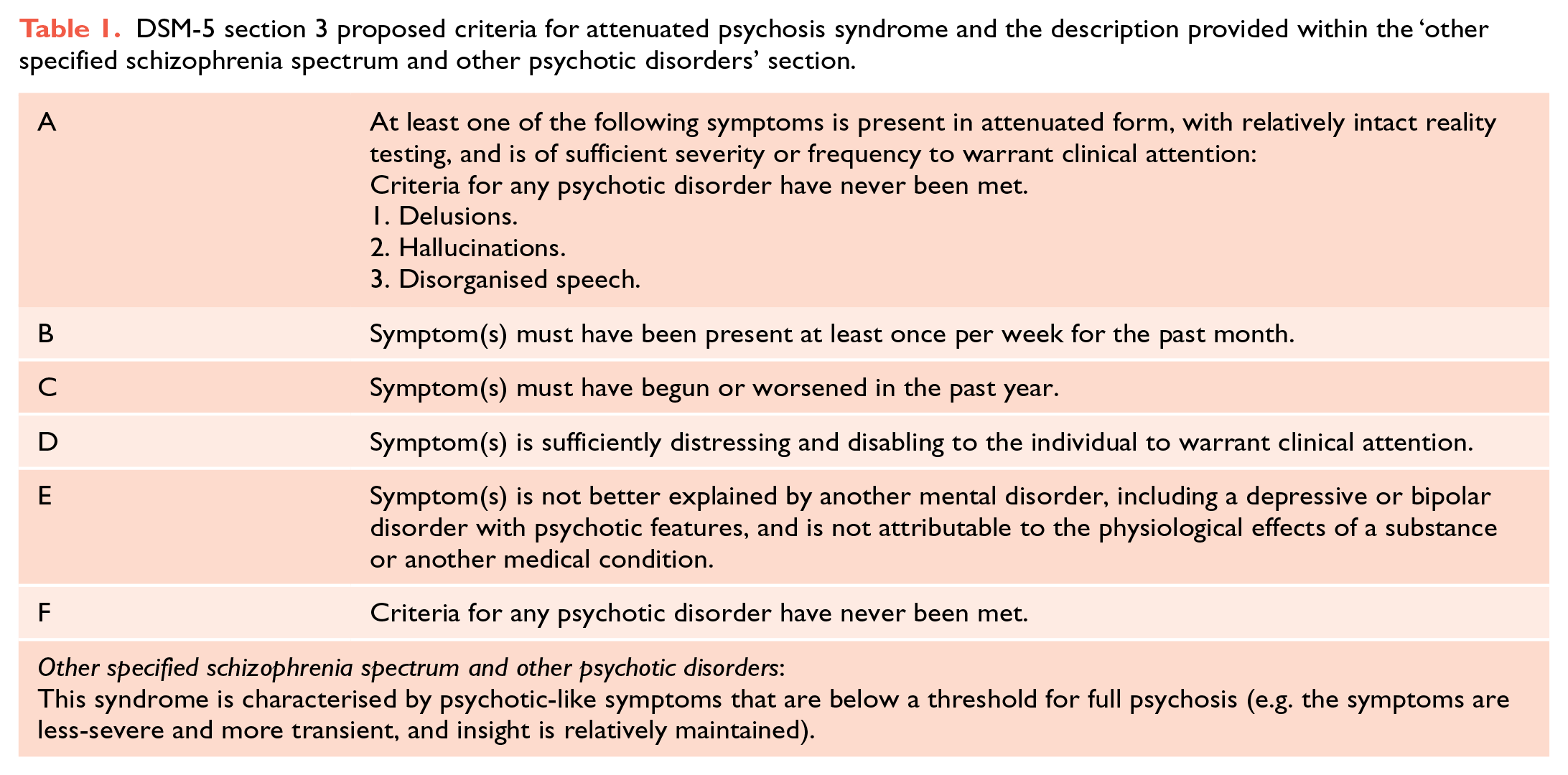
Some years ago, prior to the final publication of Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5), there was a concerted effort to include ‘psychosis-risk syndrome’ as a codable diagnosis. Fortunately, this did not happen and instead, attenuated psychosis syndrome (APS) was added to the section within DSM-5 termed ‘conditions for further study’ (see Table 1). As an aside, it is interesting to note that APS also appears within ‘other specified schizophrenia spectrum and other psychotic disorders’, although its description in this section is comparatively brief.
DSM-5 section 3 proposed criteria for attenuated psychosis syndrome and the description provided within the ‘other specified schizophrenia spectrum and other psychotic disorders’ section.
At first glance, the positioning of APS as a condition for further study seems to be a reasonable proposal, given that further research is most certainly needed in order to fully understand how schizophrenia and psychosis occur. In particular, what mechanistic and information processing dysfunctions produce psychotic illnesses, and to this end, delineating a clinical subgroup that is more prone to develop psychosis and schizophrenia seems logical.
However, the clinical application of APS has some obvious limitations, and for the purposes of advancing knowledge, we argue that it does not meaningfully improve upon exist-ing definitions of at-risk populations. Furthermore, there is significant po-tential for misdiagnosis, and this is particularly concerning because even a tentative diagnosis attracts stigma and can trigger the prescription of unnecessary treatment. However, it has been argued that assigning the APS descriptor prevents the application of non-specific psychotic labels, and in fact, this may diminish the likelihood of antipsychotic medication being prescribed. However, regardless of which of these scenarios is true, a more fundamental problem is the poor clinical specificity and reliability of APS.
In practice, the fact remains that not everyone who experiences subthreshold psychotic symptoms and seeks help goes on to develop psychosis per se. Furthermore, not all individuals that experience a psychotic episode develop schizophrenia. Indeed, only a third of individuals experiencing psychotic symptoms and seeking help go on to develop psychosis within the following 3 years, and of these, only three-quarters go on to develop schizophrenia (Fusar-Poli et al., 2012). In other words, overall, only a quarter of individuals that initially have psychotic symptoms (subthreshold APS symptoms) and seek help will eventually be diagnosed with schizophrenia (see Figure 2). This means that many individuals who over a period of time experience symptoms that can be clinically construed as a prodrome to schizophrenia, do not in fact develop the illness. Therefore, it is necessary to determine these divergent pathways noting that it is important to track and investigate those who do not progress to schizophrenia as they may hold the key to factors that confer resilience.

Schematic highlighting the overall percentage of help-seeking individuals that will eventuate in a diagnosis of schizophrenia. (a) Of the general population (Green), 8–13% will experience APS symptoms (Yellow) (Van Os et al., 2009). (b) Of this subgroup (Yellow), 36% (approximately one-third) will experience a psychotic episode (Orange) within 3 years. (c) And finally, of these individuals (Orange), approximately three-quarters will be diagnosed with schizophrenia (Red) (Fusar-Poli et al., 2012). (d) In other words, of all individuals with APS symptoms seeking help, only a quarter (Red) will eventually progress to a diagnosis of schizophrenia.
Defining a threshold
To differentiate those that will progress to a psychotic episode/disorder, and those that will not, requires a clinical threshold – ideally, one that discriminates robustly and is easily applied. However, what this threshold should constitute and how APS may assist in its identification remains unclear. Furthermore, although the concept of a psychotic prodrome is a useful one, whether APS can meaningfully capture this, seems improbable. This is because APS is ambiguously defined.
For most psychiatric disorders, the distinction between syndromal and subsyndromal is based on severity, and broadly speaking, this is judged on the basis of how many symptoms the individual is experiencing. For example, in DSM-5 Major Depression, although a ‘main’ symptom is required to make the diagnosis, e.g., either depressed mood or loss of interest/pleasure, it is the total number of symptoms (five or more) that is usually used as a diagnostic threshold. This approach cannot be applied to APS because only one symptom, e.g., a single delusion, is needed to make the diagnosis in the first place. Therefore, the threshold for APS lies within the nature of its symptom(s), and although symptom severity and frequency are rated, it is the degree of insight that is central to diagnosis.
Potential APS symptoms include delusions and hallucinations, and by definition, a delusion requires complete conviction and a hallucination requires the individual to regard the percept as absolutely real. However, the APS criteria suggest that for the purposes of attenuation, delusional symptoms do not have to possess the fixed nature necessary for the diagnosis of a psychotic disorder, and as regards hallucinations, individuals can have ‘scepticism about one’s reality’. But in practice, psychotic symptoms presenting for the first time are often reported in a guarded manner and so reality testing is necessarily challenging and often incomplete. Thus, evaluating the nature of phenomenology is far more complicated than simply determining whether a symptom is present or not. Furthermore, in addition to being extremely sophisticated, reality testing is also somewhat subjective, especially when abnormal ideas and percepts are at the cusp of assuming form.
The proposed criteria for APS (see Table 1) stipulate that one symptom alone in attenuated form is sufficient, but that it still has to be of sufficient severity or frequency to warrant clinical attention, and, at the same time, reality testing must remain relatively intact. Given these nuances, the accurate diagnosis of APS clearly requires careful and meticulous examination, and this is particularly difficult to achieve early in the course of illness.
Put simply, DSM-5 uses rather vague terminology to define the edges of APS, and this makes defining APS in clinical practice much more difficult. For example, ‘psychosis-like’ is used to insinuate that the symptoms of APS fall below the threshold for a full psychotic disorder, primarily because they are less-severe and more transient, and insight is relatively maintained. But what does psychosis-like mean? At the same time, even though the symptoms of APS are meant to be ‘less-severe’ than those of a psychotic disorder, within APS, they are deemed to exist on a spectrum that ranges from mild, moderate to severe. This is confusing because it means symptoms (within APS) may be severe, and yet they are not severe enough to meet a psychosis threshold.
In addition to the conceptual mire created by criterion A, the proposed APS criteria add further confusion by utilising arbitrary frequency and duration criteria. For instance, criterion B stipulates symptoms must be present at least once per week for the past month. It is unclear how this figure has been derived, and curiously, no further explanation is provided in the discussion of ‘diagnostic features’. In addition, criterion B does not characterise the symptoms temporally – specifying, for example, how long an episode lasts. Regarding this, criterion C appears to provide a threshold for the recency of symptom onset, but it too complicates matters by stating that symptoms must have ‘begun or worsened in the past year’. This means that symptoms may have begun in the past year, but could also have begun before this time and are now (in the past year) simply worsening? Such lack of clarity within the various criteria perhaps explains why progress in generating a specific and predictable model for individuals at risk of psychosis has been slow.
Reification as a disorder
Arguably, the most damaging consequence of the proposed criteria for APS is not that they have thwarted research, but rather that APS is increasingly being regarded in practice as a disorder, and one with definable features. Although the criteria are clearly proposed and not codable, the functional impairment, and distress associated with APS, has led to these poorly defined symptoms of a syndrome being held in the same regard as diagnoses, even though they are of little predictive or prognostic value. In our view, the insidious graduation of APS to the status of a disorder is not only premature and damaging for reasons already outlined but also potentially dangerous as it will likely divert the focus of research. And so, while we fully appreciate the need to define a prodrome so as to investigate the precursors to psychosis and schizophrenia, and support this approach where feasible, we argue that APS is not the answer and that the concept is fundamentally flawed because of the threshold upon which it is predicated.
If not APS, then what?
Clearly, efforts to identify a psychosis prodrome are urgently needed. However, thus far, we have been unable to identify any biomarkers that can reliably predict which individuals of those that are at risk will go on to experience a psychotic episode and/or progress to a diagnosis of schizophrenia. Part of the problem is that many recent efforts have been relatively non-specific and have tried to capture all individuals potentially at risk. This strategy has produced interventions that essentially lack a target, and as a consequence, they have yielded limited results. We argue that meaningful insights are more likely to emerge from more targeted approaches that are centred on individuals more proximal to psychosis – i.e., those that have experienced a psychotic episode. This is because it is now increasingly evident that significant, permanent neurobiological changes occur once the boundary into psychosis has been crossed. By subjecting these individuals to the same scrutiny as that being used to examine APS symptoms, useful indicators of psychosis are perhaps more likely to be identified. Of course, any such ‘biomarkers’ are still very distal with respect to unveiling the true aetiology of psychosis, but at least they are likely to enhance the reliability and validity of diagnosis.
In conclusion, the desires that have driven the creation of APS are well-intentioned, but the risk of unnecessarily stigmatising individuals by prematurely labelling them and the risk of inappropriately medicating these individuals needs to be recognised. Instead, greater emphasis needs to be given to further research into the aetiology and pathogenesis of severe psychiatric conditions such as psychosis and schizophrenia. And, at the same time, the examination of groups of symptoms that are yet to crystallise into psychosis needs to be undertaken speculatively.
Make News
In an age where good news and good ideas are difficult to find, this series offers constructive criticism of promising concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with re-spect to the research, authorship and/or publication of this article: G.S.M. has re-ceived grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier; and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.