
Abstract

To the Editor
A recent letter criticises a ‘Treatment support and discharge plans inquiry’ (West Australian Mental Health Advocacy Service, 2018) and its ‘recovery-focused’ language reforms, saying they strongly evoke ‘Orwellian doublespeak’ (Stampfer, 2019). The author highlights a disconnect between clinical terms and their proposed recovery-focused ‘translations’.
Stampfer takes the proposed reforms out of context. Viewing them as originally presented (Table 1), it is clear from the asymmetry that these are not intended as direct ‘translations’. Rather, a collection of contentious terms are compared with some suggested alternatives, which encourage the user to understand and describe behaviour in a more recovery-focused way.
Examples of recommended language reforms (West Australian Mental Health Advocacy Service, 2018).
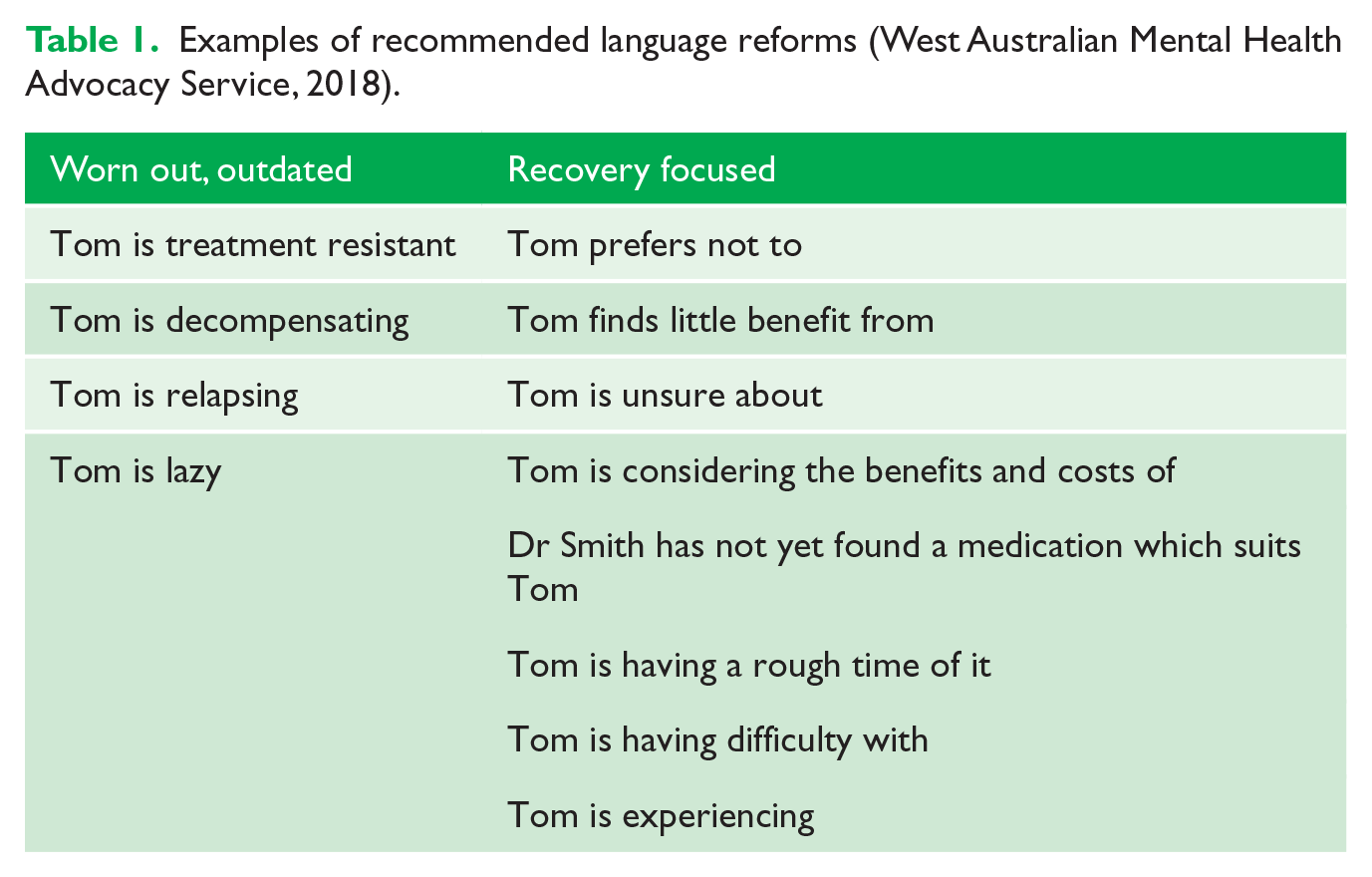
The intention is not simply to replace one term with another – it is to find ways to think and speak more compassionately about consumers, rather than to stigmatise and disempower people with mental illness. The intention is to understand the context of the person – the meaning of behaviour in the context of their life and illness – rather than rely on reductionist or pejorative descriptors.
Furthermore, it is important to understand the context from which these proposals come. The report is authored by an advocacy organisation, not a clinical one. Such organisations in the recovery movement are often catalysed by consumers, stigmatised and traumatised by aspects of the mental health system. It should not surprise, or be viewed as ‘Orwellian’, that their advocacy will include the pursuit of more respectful, recovery-focused language.
I agree that some of the proposed reforms go too far – clinical and phenomenological terms like ‘grandiose’, ‘psychotic’ and ‘relapse’ belong in the clinician’s lexicon. However, the spirit of recovery-focused language is to emphasise personhood and empathy over labelling and dehumanising. The point is to have a person-centred and non-judgemental approach at the centre of our communication, even when clinical terms are used. We have all seen how value-laden and pejorative terms such as ‘lazy’ or ‘manipulative’ can stoke negative attitudes towards consumers; we would do well to reconsider our use of them.
In my registrar role at a recovery-focused community care unit, my own use of language has been challenged. At first, I laughed when, instead of ‘obese’, I was encouraged to a phrase like ‘compromised in weight’. What my colleague helped me to understand was that reframing my language could help me reframe my thinking and to cast less judgement on the consumer and more reflection on, say, my clozapine prescription.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.