
Abstract

To the Editor,
Creutzfeldt–Jakob disease (CJD) is a rapidly progressive neurodegenerative entity that often challenges neurologists and psychiatrists in clinical practice. Its classic triad involves rapidly progressive dementia, myoclonus and ataxia (Manix et al., 2015). An unusual clinical presentation of CJD occurs in the so-called Heidenhain variant (HvCJD), characterized by visual symptoms at the disease onset, including decreased visual acuity, altered perception of colors or structures and visual hallucinations, in the absence of cognitive impairment and motor symptoms (Baiardi et al., 2015). We discuss a probable case of HvCJD characterized by affective symptoms, apathy and visual hallucinations initially diagnosed as depression and a functional neurological disorder.
A 54-year-old man was referred to the emergency department because of a 4-month history of altered vision and depressive symptoms. He experienced episodes of blurred vision, chromatopsias and complex visual hallucinations, for which he consulted an ophthalmologist. The initial studies including cranial tomography, electroencephalogram (EEG) and campimetry were unremarkable. In light of this situation, he was referred to a psychiatric evaluation. Sad mood, insomnia and feelings of worthlessness were noticed. He was diagnosed with a major depressive episode, for which cognitive behavioral therapy represented no improvement. Moreover, he was apathetic and his vision deteriorated further. Three weeks before admission, cognitive decline became apparent with difficulty remembering names and repetitive conversations.
On admission, the patient was awake and well oriented. He had frequent episodes of joking with prominent laughter. Action tremor and mild dysmetria were evidenced. In addition, his ophthalmological examination was considered ‘inconsistent’, and a functional neurological disorder was diagnosed. A second EEG showed periodic sharp wave complexes, which were most prominent over the parieto-occipital regions (Figure 1). An 18-fluorodeoxyglucose positron emission tomography (FDG-PET) showed global hypometabolism, marked on the occipital lobes (Figure 2). Neuronal degeneration markers were positive, and the diagnosis of probable HvCJD was integrated. The patient died 5 months after his initial presentation.

EEG recording showing typical generalized periodic sharp wave complexes, prominent over the parieto-occipital regions.
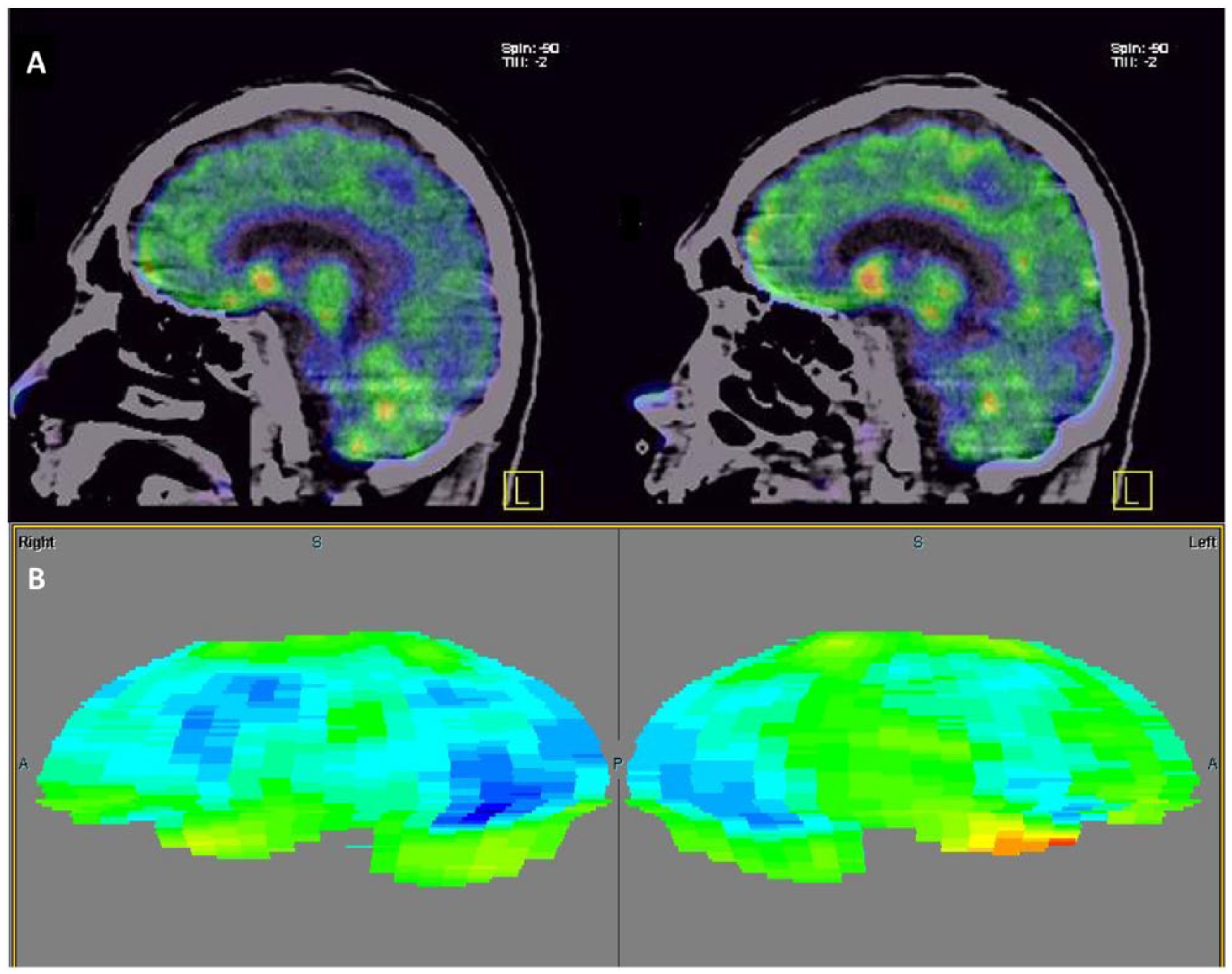
Hybrid study of F-18 FDG PET/CT: (A) decreased overall metabolism, more prominent in the precuneus and the primary visual area. (B) Scenium® cortical analysis in which affected areas are evident on blue scales.
Even though neuropsychiatric symptoms constitute an early and prominent manifestation of CJD, clinicians typically ignore these symptoms in its diagnostic approach (Abudy et al., 2014). The presence of late-onset unspecific visual symptoms in conjunction with affective or psychotic symptoms should include CJD in the differential diagnosis (Abudy et al., 2014). Repeated EEG and imaging examinations may be performed at different time points, as they might be normal initially (Abudy et al., 2014). This report provides further evidence on the importance of psychiatric symptoms in the assessment of CJD. Timely diagnosis can allow patients to make life decisions and receive prompt palliative care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.