
Abstract
Objective:
The number of refugees worldwide is unprecedented in recent history. Little is known, however, about profiles of psychological symptoms following persecution and displacement.
Methods:
This study reports on a latent class analysis that identified profiles of posttraumatic stress disorder (PTSD), depression and anxiety symptoms in a nationally representative sample of 1625 refugees in Australia. The association between specific symptom profiles, exposure to potentially traumatic events and post-migration stressors, and overall health and help-seeking was examined.
Results:
Latent class analysis yielded an optimal five-class solution. These classes comprised the Pervasive Symptom class (19.2%), the High PTSD Symptom class (17.1%), the High Depression/Anxiety Symptom class (16.4%), the Moderate PTSD Symptom class (16.2%) and the Low Symptom class (31.1%). Participants in the symptomatic classes were more likely to be female, older and report greater post-migration stressors than those in the Low Symptom class. In addition, individuals in classes characterized by PTSD symptoms had been exposed to more types of potentially traumatic events. Membership in symptomatic classes was associated with poorer overall heath and greater help-seeking.
Conclusion:
Qualitatively distinct symptom profiles were observed in a nationally representative sample of refugees. In addition to a group of people who reported high symptoms across psychological disorders and may warrant clinical intervention, we identified two subclinical classes who may be missed by existing diagnostic classification systems. Post-migration stressors play an important role in influencing refugee symptom profiles over and above exposure to potentially traumatic events. Clinicians should consider specific symptom profiles and contextual factors when planning interventions with refugees.
The number of individuals forcibly displaced across the globe is unprecedented since the end of World War II (UNHCR, 2018). The mental health consequences of persecution and displacement present an enormous challenge for the health systems of host countries. Elevated rates of psychological disorders including posttraumatic stress disorder (PTSD) and depression have been documented in refugees and asylum-seekers (Bogic et al., 2015; Steel et al., 2009). High levels of comorbidity in these groups lead to pervasive and complex symptom presentations that are associated with substantial disability (Marshall et al., 2005; Mollica et al., 1999; Momartin et al., 2004; Nickerson et al., 2017).
Current diagnostic systems offer limited opportunities to identify distinctive symptom profiles among refugees, rather reducing symptom presentation to a binary diagnostic status classification. Furthermore, such approaches risk individuals with significant levels of symptomatology and associated disability being missed when identification is conducted on the basis of diagnosis (Marshall et al., 2001; Zlotnick et al., 2002). While binary diagnostic taxonomies have important benefits for the identification of individuals with debilitating psychiatric diagnoses, it may be useful to combine these frameworks with approaches that identify common symptom profiles and consider how these relate to other important predictive and outcome factors.
Person-centred approaches such as latent class analysis (LCA) represent a promising example of such an approach as they classify individuals according to profiles of psychological symptoms and examine the association between key experiences, sociodemographic variables and symptom presentation. This is critically important in the case of refugees where the heterogeneity of trauma exposure and post-migration stressors may give rise to a variety of symptom presentations, the nuances of which may not be captured by a diagnostic classification system. In addition, this approach affords the opportunity to identify specific risk markers for different functional outcomes, with important treatment implications. To date, no study has investigated the profiles of psychological symptoms in a nationally representative sample of resettled refugees. To our knowledge, there have been two studies that have implemented LCA with resettled refugees. The first investigated the profiles of PTSD and prolonged grief symptoms in a convenience sample of Iraqi refugees living in Australia (Nickerson et al., 2014). This study yielded a four-class solution, namely, a high symptoms class (16%), a PTSD class (25%), a prolonged grief disorder class (16%) and a resilient class (43%). In addition, this study found that class membership was differentially predicted by pre- and post-migration experiences, with traumatic loss being associated with membership in the high symptoms class, while adaptation difficulties and loss of culture and support were associated with membership in the prolonged grief disorder and PTSD classes, respectively. The second study investigated the profiles of PTSD symptoms in a sample of refugees from Arabic-, Farsi-, Tamil- and English-speaking backgrounds. This study yielded a four-class solution, comprising a high PTSD class (21%), a high re-experiencing/avoidance class (15%), a moderate PTSD class (23%) and a no PTSD class (40%). Exposure to traumatic events and post-migration stressors again significantly predicted membership in the more symptomatic classes. Findings from both of these studies are consistent with a broad body of literature that highlights the role of pre-migration trauma and post-migration living difficulties in contributing to psychopathology among refugees (Li et al., 2016; Mollica et al., 1998; Porter and Haslam, 2005; Steel et al., 2009); however, relatively little is known regarding the differential impact of refugee experiences on subsequent symptom presentation.
This study proposes to conduct the first latent investigation of classes of a nationally representative sample of resettled refugees according to profiles on core psychological symptoms including posttraumatic stress, depression and anxiety symptoms. We predict that four classes will be identified in this sample, namely, a High Symptom class, a Predominantly PTSD class, a Predominantly Depression and Anxiety Symptom class and a Low Symptom class. This prediction is based on the finding from Nickerson et al. (2014) that distinctive classes characterized by PTSD symptoms and other types of symptomatology (in this case prolonged grief symptoms) were identified alongside High and Low Symptom classes in a sample of resettled refugees. We thus tentatively hypothesize that a Predominantly PTSD class would emerge, in addition to a class that evidenced more general distress that was not characteristic of PTSD symptoms. Furthermore, we predict that membership of these classes will be differentially predicted by refugee experiences. Specifically, we hypothesize that membership in the classes characterized by PTSD symptoms will be predicted by greater exposure to pre-migration trauma, while membership in the classes characterized by depression/anxiety symptoms will be predicted by greater exposure to post-migration living difficulties. We also predict that membership in the symptomatic classes will be associated with poorer overall health and higher levels of treatment-seeking compared to the Low Symptom class.
Method
Participants
Participants in this study were 1647 refugees who had arrived in Australia via the humanitarian entrants programme. They represented a subset of those who took part in the larger Building a New Life in Australia (BNLA) study. This study was conducted by the Australian Department of Social Services (DSS) and the Australian Institute of Family Studies (Edwards et al., 2018). It is a population-based cohort study that investigates factors relating to the settlement of refugees in Australia over five waves annually from the time at which they are granted a visa. This study reports on data collected in wave 3 (collected between October 2015 and March 2016, 2 years after baseline assessment), after participants had been in Australia for a minimum of 2 years.
Measures
Exposure to potentially traumatic events
At wave 3, a 10-item scale was implemented to index types of potentially traumatic events to which refugees are commonly exposed. Participants responded yes or no to each trauma type. A total count score of the numbers of types of traumatic events to which an individual had been exposed was calculated, excluding the final ‘other’ item. This score ranged from 0 to 9.
Exposure to post-migration living difficulties
Participants responded to a 12-item scale to indicate current sources of stress in his or her life. A total count score of the number of significant stressors endorsed by participants was calculated. This score ranged from 0 to 12.
PTSD-8
PTSD symptoms were assessed using the PTSD-8 scale (Hansen et al., 2010). This scale comprises eight items assessing core symptoms of PTSD, including re-experiencing symptoms (intrusive memories, flashbacks, nightmares and psychological/physiological reactivity to reminders), avoidance symptoms (avoiding thoughts or feelings associated with the trauma and avoiding activities that remind the individual of the trauma) and hyperarousal symptoms (startle response, hypervigilance). Participants rated each item in terms of how much it bothered them over the past week on a four-point scale ranging from Not at All (1) to Most of the time (4). Items on the PTSD-8 were dichotomized to represent symptom present (Sometimes and Most of the time) and symptom absent (Not at all and Rarely). Items were dichotomized to map onto clinically used diagnostic approaches which operate according to symptom present/absent dichotomies. Internal consistency for this measure was 0.96.
Kessler-6
Symptoms of anxiety and depression were assessed using the Kessler-6 scale (K6; Kessler et al., 2010). This scale comprises two anxiety symptoms (feeling nervous, feeling restless or fidgety) and four depression symptoms (feeling hopeless, feeling that everything was an effort, feeling so sad nothing could cheer you up and feeling worthless). Participants indicated how often they experienced each symptom over the past previous 4 weeks. Items were rated on a five-point scale ranging from None of the time (1) to All of the time (5). Items on the K6 were dichotomized to represent symptom present (Some of the time, Most of the time or All of the time) or symptom absent (None of the time; A little of the time). Internal consistency for this measure was 0.91.
Help-seeking
Participants were asked if they had sought help for emotional problems since arriving in Australia, with responses being binary (yes/no).
Overall health
Participants were asked about the state of their overall health in the past 4 weeks. Responses were recorded on a six-point scale ranging from 1 (excellent) to 6 (very poor).
Procedure
The BNLA study data collection was conducted in 11 major cities and regional areas across Australia. Sites were selected to optimize (1) adequate sample size (according to the number of refugees living in a particular area), (2) geographic diversity and (3) representation of types of humanitarian visas. Inclusion criteria included (1) being the ‘principal’ applicant for a humanitarian visa granted in May to December 2013 and (2) aged 18 years or older. Participants recruited in the initial phase then provided permission for other members of their family to be contacted: these represented ‘secondary applicants’ and comprised spouses, co-parents, children and other relatives. Secondary applicants were invited to take part in the study if they were older than 15 years of age and residing with the primary applicant.
In wave 3, data were collected using computer-assisted self-interview (CASI) software during home visits. Participants were given the option of completing self-report questionnaires using a computer interface, or undertaking a computer-assisted personal interview (CAPI) where BNLA field workers entered the participants’ responses into the computer. Interviews lasted approximately 45 minutes to 1 hour. Survey materials were available in Arabic, Burmese/Myanmar, Chin Haka, Dari, Hazaragi, Nepali, Persian, Swahili and Tamil. Questionnaires were subjected to a translation and multi-stage quality assurance process. Participants were usually matched with an interviewer who was fluent in their native language; otherwise, participants could choose to access an accredited interpreter to complete the survey. Ethics approval for this study was obtained from the Australian Institute of Family Studies Human Research Ethics Committee.
Data analysis
A multi-level LCA was conducted to identify symptom profiles based on items assessing PTSD, depression and anxiety symptoms using Mplus version 7 (Muthen and Muthen, 1998–2013). Survey weights were incorporated into the model to account for initial non-response and attrition, as well as to ensure that results were representative of the larger population of refugees who had received a humanitarian visa in this time period. LCA uses categorical symptom indicators to identify response patterns, with individuals being assigned to classes on the basis of these patterns. LCA (with dichotomous indicators) was implemented in this study instead of latent profile analysis (with continuous indicators) to map onto diagnostic procedures which use symptom-present/absent dichotomies to characterize psychological symptoms.
Single-level LCA assumes independence of observations. As individuals in this study were clustered in family groups, we conducted a multi-level LCA in this study. This analytic procedure accounts for the two-level structure of the data by estimating a model at the family level as well as the individual level. In our case, we used the parametric approach which fitted a between-level factor for random latent class intercepts (Henry and Muthen, 2010). We implemented full information maximum likelihood estimation to account for missing data on indicator variables.
In this paper, we implemented a two-step process by which the optimal unconditional model is first identified, and then covariates are added to the conditional model to test for predictors of class membership. In determining the best unconditional model, the most parsimonious model (i.e. a one-class solution) was first fitted, followed by successive models with increasing numbers of classes. Comparative model fit indices were used to determine the minimum number of classes that can account for associations between symptoms in the data. We used the following information criteria, with a smaller value on these representing better model fit: Bayesian information criterion (BIC), sample size–adjusted Bayesian information criterion (SS-BIC) and the Akaike information criterion (AIC). We also used entropy, with higher values indicating better model fit. We also considered the Vuong–Lo–Mendell–Rubin likelihood ratio test (VLMR-LRT) and the Lo–Mendell–Rubin adjusted likelihood ratio test (LMR-LRT). A non-significant value on these tests indicated that the current model (k) did not exhibit better fit than a model with one fewer classes (k – 1). Finally, interpretability and parsimony were considered in selecting the optimal model. The following values were used to interpret symptom probabilities within classes: ⩾0.60 were considered to represent a high probability of symptom endorsement in a specific class, values ⩽ 0.59 and ⩾0.16 were considered to represent a moderate probability of symptom endorsement in a specific class and values ⩽ 0.15 were considered to represent a low probability of symptom endorsement in this class (Galatzer-Levy et al., 2013).
To investigate predictors of class membership, a conditional model was constructed. Covariates entered into the model included gender, age, time in Australia, number of traumatic events experienced in the home country and number of living difficulties experienced as a significant problem in Australia. As our interest in this study was primarily at the level of the individual, all covariates were specified as Level 1 predictors of class membership. All covariates were entered into the model simultaneously, and a multinomial logistic regression was used to determine how these variables related to class membership. Multiple imputation (10 datasets) was used to account for missing data in covariates. Variables used for multiple imputation included gender, age, living difficulties, time in Australia and exposure to traumatic events. Previous investigations of the validity of employing multiple imputation for missing data on demographics and life experiences (including trauma exposure) have suggested that this results in robust estimates of model parameters with reduced bias (Cattle et al., 2011; Kim et al., 2018; Newgard et al., 2012; Oyetunji et al., 2011). As multiple imputation cannot be used simultaneously with survey weights in Mplus, data were first imputed and then the imputed datasets were used to estimate the conditional model, rather than data imputation taking place in the conditional model itself.
Multinomial logistic regression was also used to investigate the association between class membership and overall health and help-seeking behaviour; these were conceptualized as distal outcomes of class membership rather than model covariates.
Results
Participant characteristics
Of the 1647 refugees who took part in this study, 839 (50.9%) participants were female and participants had a mean age of 38.41 (SD = 14.59, range = 16–76 years). Participants completed the survey in a variety of languages, including Arabic (n = 786, 48%), Persian (n = 374, 23%), English (n = 178, 11%), Dari (n = 98, 6%), Nepali (n = 77, 5%), Burmese/Myanmar (n = 45, 33%), Chin Haka (n = 34, 2%), Hazaragi (n = 30, 2%), Swahili, Tamil, Karen and other (n = 30, 2%). The majority of participants had arrived in Australia between 2 and 3 years previously (n = 1567, 95.1%), with the remainder having arrived 2 years previously (n = 80, 4.9%). A total of 22 participants had data missing on all indicator variables (see below), resulting in a final sample size of 1625.
Trauma exposure and post-migration living difficulties
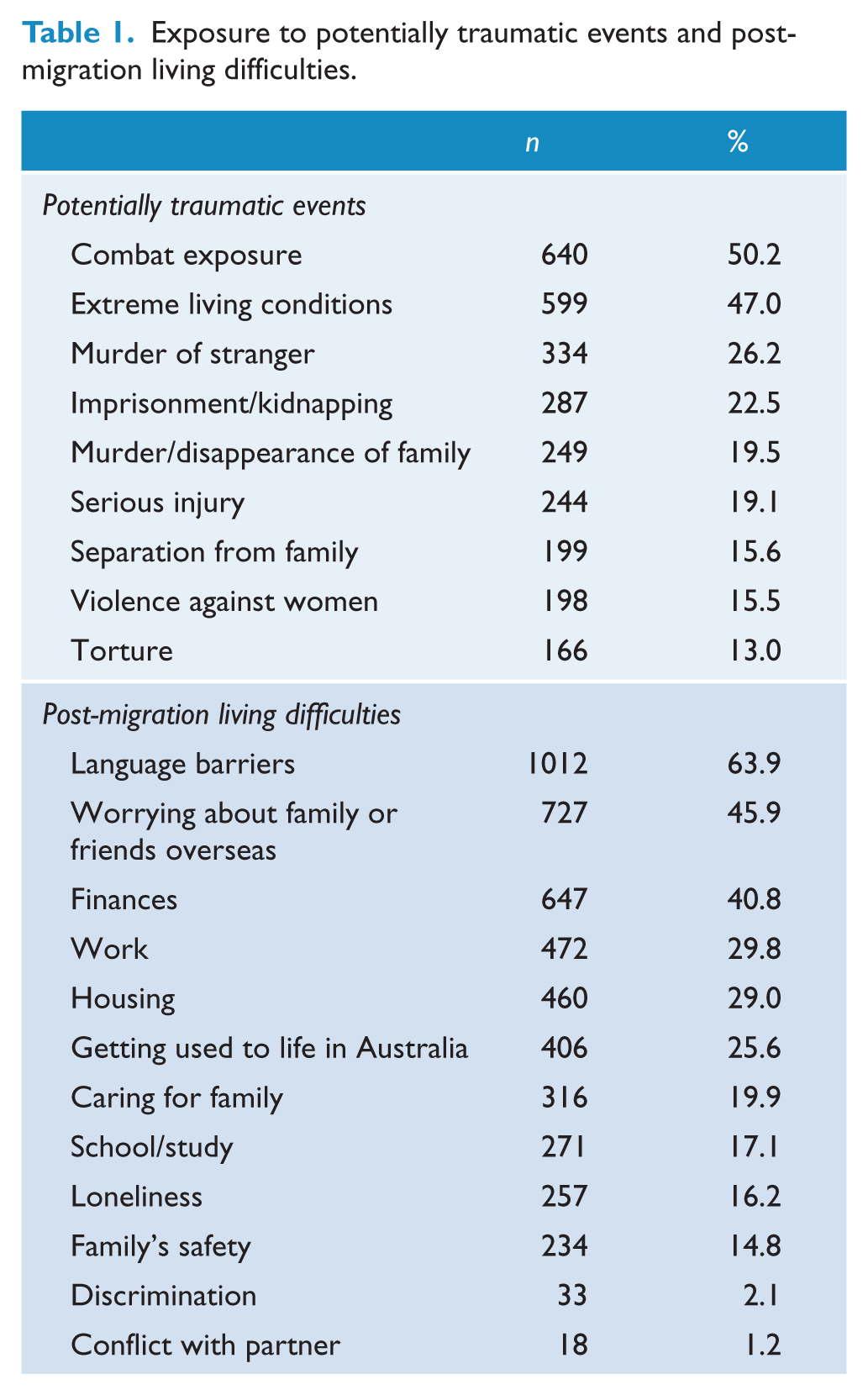
Participants in this study had been exposed to a mean of 2.79 (SD = 2.01) types of potentially traumatic events from a list of 10 events assessed (see Table 1). Of the 1647 refugees who took part in this study, 1275 participants responded to the trauma exposure items. Of these, the most commonly endorsed events (experienced by approximately half of the sample) were combat exposure (n = 640, 50.2%) and extreme living conditions (n = 599, 47.0%). Of the 1647 participants in this study, 1524 responded to most of the living difficulty items, with the exception of the ‘conflict with partner’ item, to which 1483 participants responded. Participants endorsed a mean of 2.68 (SD = 1.99) types of living difficulties (see Table 1). Over 40% of the sample reported language barriers (n = 1012, 63.9%), worry about family or friends overseas (n = 727, 45.9%) and finances (n = 647, 40.8%) to be significant living difficulties. Over a quarter of the sample identified work (n = 472, 29.8%), housing (n = 460, 29.0%) and getting used to life in Australia (n = 406, 25.6%) as being significant stressors.
Exposure to potentially traumatic events and post-migration living difficulties.
LCA
Unconditional models
LCA revealed that a five-class solution best fit the data (see Table 2). All information criteria (AIC, BIC and SS-BIC) showed substantial reductions until the five-class solution, which then demonstrated relatively smaller reductions from the five- to six-class and six- to seven-class solutions. Entropy was strong for all solutions (>0.83) demonstrating good class differentiation. The VLMR-LRT and LMR-LRT indicated that the three-class solution did not fit the data better than the two-class solution; however, there were substantial reductions in information criteria from the two- to three-class solution, and thus four- to seven-class solutions were tested. The VLMR-LRT and LMR-LRT revealed that the five-class solution fit the data better than the four-class solution; however, the six- and seven-class solutions did not yield significantly better fit compared to the five-class solution. Furthermore, inspection of the class plots revealed that the five-class solution comprised five distinct classes with membership of greater than 16% of the sample for all classes. Accordingly, the five-class solution was retained.
Fit indices for unconditional models in latent class analysis of PTSD, depression and anxiety in humanitarian entrants in Australia.
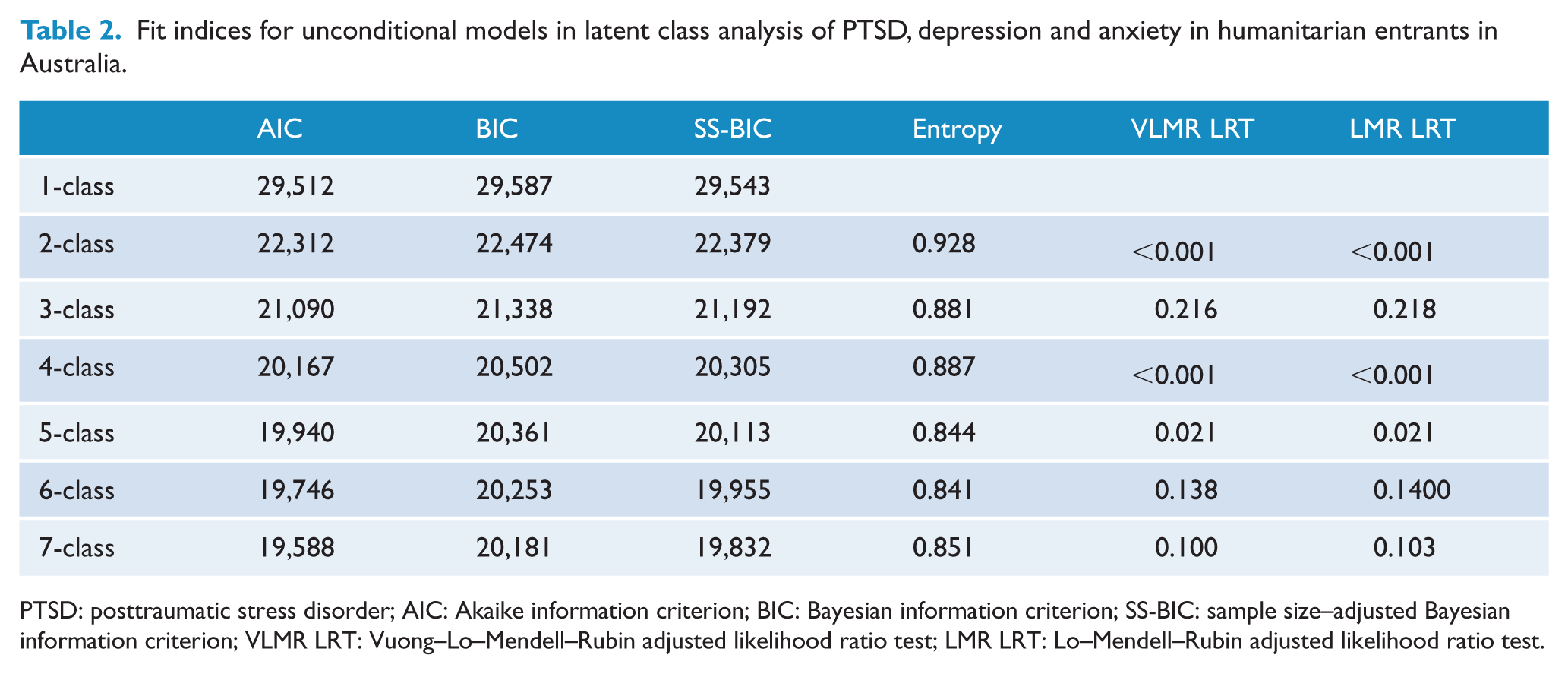
PTSD: posttraumatic stress disorder; AIC: Akaike information criterion; BIC: Bayesian information criterion; SS-BIC: sample size–adjusted Bayesian information criterion; VLMR LRT: Vuong–Lo–Mendell–Rubin adjusted likelihood ratio test; LMR LRT: Lo–Mendell–Rubin adjusted likelihood ratio test.
The conditional probabilities for symptom endorsement according to class membership are presented in Figure 1 (see Supplementary Table 1 for values). Participants in the Pervasive Symptom class (19.2%) had a high probability of endorsing all anxiety, depression and PTSD symptoms.
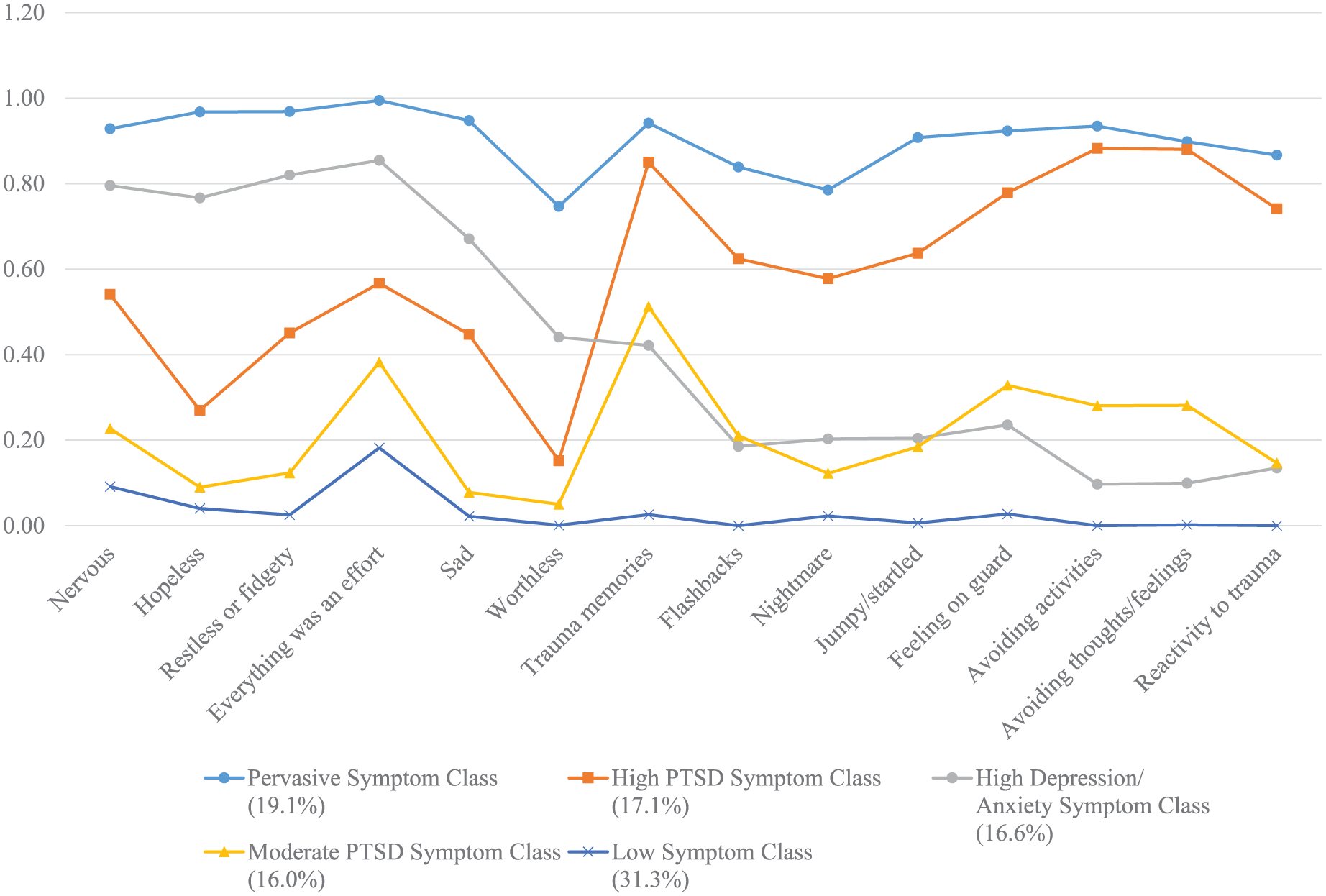
Profiles of PTSD and Depression/ Anxiety Symptoms amongst Resettled Refugees
Participants in the High PTSD Symptom class (17.1%) had a high probability of endorsing all PTSD symptoms with the exception of nightmares which evidenced a near-high probability (0.58) and a moderate probability of endorsing all depression and anxiety symptoms.
Participants in the High Depression/Anxiety class (16.4%) had a high probability of endorsing all anxiety and depression symptoms, with the exception of worthlessness which had moderate endorsement. This class also had a moderate probability of endorsing a range of PTSD symptoms including thoughts of the trauma, flashbacks, nightmares, being jumpy and being on guard. Participants in this class had a low probability of endorsing avoidance of trauma thoughts or activities relating to the trauma and reactivity to trauma reminders, most with conditional probabilities below 0.3.
Participants in the Moderate PTSD Symptom class (16.2%) had a moderate probability of endorsing the PTSD symptoms trauma-related thoughts, flashbacks, feeling jumpy, feeling on guard, avoidance of trauma-related thoughts and activities and reactivity to reminders. Participants in this class had a moderate probability of endorsing depression and anxiety symptoms relating to nervousness and feeling everything is an effort. These participants had a low probability of endorsing hopelessness, restlessness, feelings of worthlessness and feeling jumpy.
Participants in the Low Symptom class (31.1%) had a moderate probability of endorsing feeling everything is an effort and a low probability of endorsing all other symptoms.
Conditional models
Covariates of class membership are presented in Table 3. Compared to those in the Low Symptom class, individuals in all the symptomatic classes were more likely to be female, older and have experienced more post-migration living difficulty stressors. Those in the Pervasive Symptom and High PTSD Symptom classes had been exposed to more types of traumatic events.
Covariates of class membership for five-class solution.
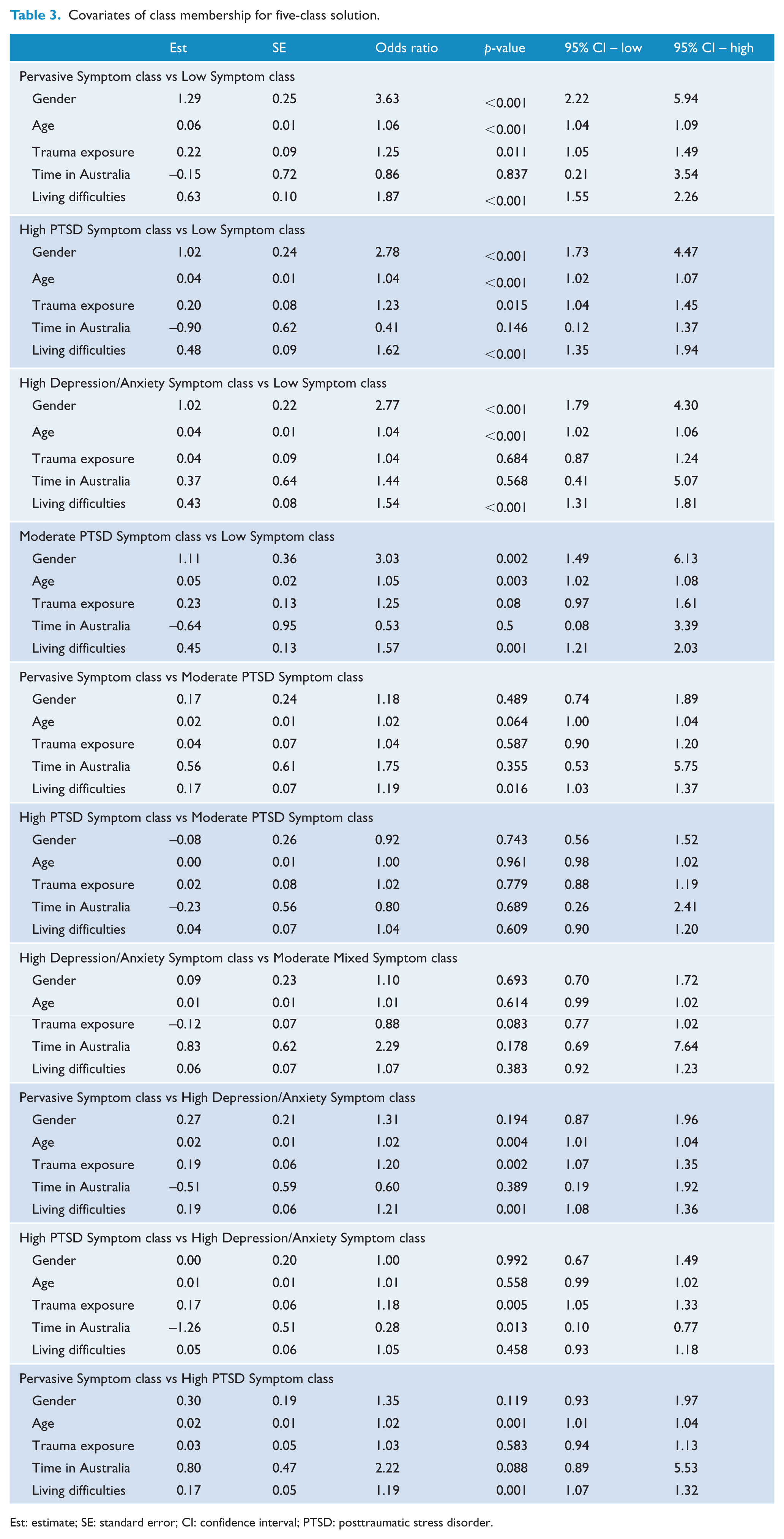
Est: estimate; SE: standard error; CI: confidence interval; PTSD: posttraumatic stress disorder.
Compared to those in the Moderate PTSD class, individuals in the Pervasive Symptom class were more likely to have been exposed to more living difficulties.
Compared to those in the High Depression/Anxiety Symptom class, those in the Pervasive Symptom and High PTSD Symptom classes had experienced more types of traumatic events. Those in the Pervasive Symptom class were also older and had experienced more living difficulties. Those in the High PTSD Symptom class had been in Australia for a shorter period of time. Compared to those in the High PTSD Symptom class, participants in the Pervasive Symptom class were more likely to be older and have experienced more living difficulties. There were no differences between those in the High PTSD Symptom or the Moderate PTSD Symptom classes in terms of covariates.
Association between class membership and overall health
See Supplementary Table 2 for the results of multinomial logistic regression analyses investigating the association between class membership, overall health and help-seeking. Participants in the Pervasive Symptom class had significantly poorer overall health than those in all other classes. Participants in the High PTSD Symptom class had significantly poorer overall health than those in the Low Symptom class but not High Depression/Anxiety Symptom class.
Participants in the High Depression/Anxiety Symptom class had poorer overall health than those in the Low Symptom and Moderate PTSD Symptom classes. Participants in the Moderate PTSD Symptom class had significantly poorer overall health than those in the Low Symptom class.
Association between class membership and help-seeking
Participants in the Pervasive Symptom class were more likely to have sought emotional help than those in all other classes. Participants in the High PTSD Symptom class were more likely to have sought help than those in the Low Symptom class, the Moderate PTSD Symptom class and the High Depression/Anxiety Symptom class. Participants in the High Depression/Anxiety Symptom class were more likely to have sought help than those in the Low Symptom class, but not the Moderate PTSD Symptom class. Participants in the Moderate PTSD Symptom class were more likely to have sought help than those in the Low Symptom class.
Discussion
An LCA of posttraumatic stress, depression and anxiety symptoms was conducted to identify distinctive symptom profiles among a nationally representative sample of resettled refugees who entered Australia via the humanitarian entrants programme between May and December 2013. These analyses revealed five profiles, comprising a Pervasive Symptom class (19%), a High PTSD Symptom class (17%), a High Depression/Anxiety Symptom class (17%), a Moderate PTSD Symptom class (16%) and a Low Symptom class (31%). These findings advance the empirical investigation of psychopathology in refugees which to date have largely focused on the prevalence rates of specific psychiatric disorders. Notably, the current approach facilitates the identification of transdiagnostic symptom profiles that may be missed by a focus on diagnoses, as well as individuals who may have subclinical symptom presentations. This is of critical importance when working with trauma-affected refugees who often present with high levels of psychological distress and comorbidity, as it may provide more nuanced information for treatment planning and service provision, which may supplement that obtained from more broad-brush psychiatric diagnoses. Indeed, the combination of diagnostic and symptom profile approaches may represent a promising avenue for informing intervention by both providing clear diagnostic guidance for the selection of evidence-based interventions, while allowing for the tailoring of these approaches according to specific symptom profiles.
To our knowledge, no study has previously investigated the profiles of PTSD, depression and anxiety symptoms in displaced populations, nor have they investigated this in a nationally representative sample. Only one study has implemented LCA to investigate the profiles of different types of psychopathology in resettled refugees. Nickerson et al. (2014) investigated the profiles of PTSD and prolonged grief symptoms in a convenience sample of resettled Iraqi refugees, identifying four classes, namely, a high symptoms class (16%), a PTSD class (25%), a prolonged grief disorder class (16%) and a resilient class (43%). Similar results were found among internally displaced people in Cambodia by Heeke et al. (2017) who identified four analogous symptom profiles (high symptoms – 28%, PTSD – 23%, prolonged grief – 25% and resilient – 28%). A study investigating patterns of psychiatric disorders, conducted by Silove et al. (2014) in post-conflict Timor-Leste, yielded a minimal symptoms class (86%), a paranoia-anger class (13%) and a comorbid mental disorders class (1.5%). The current findings accord with those of Heeke et al. (2017) and Nickerson et al. (2014) by identifying a Pervasive Symptom class and a distinctive PTSD symptom class. These findings are further consistent with all three studies in that they identified a resilient class as the largest class in each sample. These findings accord with a large body of research evidence that indicates that the modal psychological response to persecution and displacement is resilience (Bogic et al., 2015; Fazel et al., 2005; Steel et al., 2009). In addition to the four hypothesized classes identified in this study (high symptoms, high PTSD symptoms, high depression/anxiety symptoms and low symptoms), an additional class emerged from the data, namely, a moderate PTSD symptoms class. This class was also identified in the LCA conducted by Minihan and colleagues (2018) which found a moderate PTSD class in addition to a high PTSD class, a high re-experiencing/avoidance class and a low symptoms class in resettled refugees in Australia. This is also consistent with the research conducted with other trauma-affected populations, which has consistently found an analogous class, characterized by a moderate probability of endorsing PTSD symptoms (Ayer et al., 2011; Breslau et al., 2005; Elhai et al., 2011; Steenkamp et al., 2012). It may be the case that the representative nature of the sample reported in this study, alongside the relatively large sample size, facilitated identification of this moderate symptoms class that was not afforded by previous investigations with smaller convenience samples (Nickerson et al., 2014).
The symptom classes identified in this cohort of refugees differ in important ways from results of studies among combat veterans and survivors of civilian trauma. In contrast to the findings in this study, these studies have consistently found classes that are characterized by varying levels of symptom severity, rather than distinctive symptom profiles. Studies conducted with war veterans (Armour et al., 2015) and victimized women who were on probation and parole (Golder et al., 2015) have found evidence for low, moderate and high symptoms classes. Studies conducted with sexual assault survivors (Au et al., 2013) and motor vehicle accident victims (Hruska et al., 2014) identified an additional low–moderate symptoms class, and a study conducted with adults exposed to ongoing shelling in Israel found an additional moderate–high symptoms class (Itzhaky et al., 2017). Findings from this and other research conducted with refugee and post-conflict populations indicate that qualitatively distinct symptom profiles are observed in these populations. This provides evidence to support distinctive symptomatic impacts of persecution, war and displacement on mental health outcomes.
This study yielded two classes that have not been previously identified among refugee groups, namely, a High Depression/Anxiety Symptom class and, as discussed above, a Moderate PTSD Symptom class. The identification of a High Depression/Anxiety Symptom class has important implications for the field of refugee mental health research where the vast majority of studies to date have focused on PTSD as the primary psychiatric disorder arising from refugee trauma. This is consistent with findings from both the refugee/post-conflict mental health and general traumatic stress literature suggesting that PTSD is not the only, or even the most common, psychiatric diagnosis following exposure to trauma (O’Donnell et al., 2016; Priebe et al., 2010). In addition, the Moderate PTSD Symptom class represents individuals who, despite reporting some PTSD symptoms, would be unlikely to be identified by diagnostic procedures. These may represent individuals with subclinical PTSD symptoms, a group that has been previously found to evidence increased impairment despite failing to meet diagnostic criteria (Marshall et al., 2001; Zlotnick et al., 2002). This study indicated that over 30% of the sample belonged to either of these two novel classes, highlighting the importance of considering subclinical presentations when working with refugees in both clinical and research settings. Despite reporting relatively poor overall health, participants in these two classes were less likely than those in the other symptomatic classes to be accessing mental health services. This provides evidence that there exist a group of refugees with prominent and disabling psychological symptoms who are not receiving mental health assistance. It may be the case that such a group of refugees are candidates for a low-intensity or brief intervention that can be delivered in community settings (Dawson et al., 2015).
The finding that nearly 20% of the sample was classified as experiencing ‘pervasive symptoms’ is consistent with a growing body of literature documenting the high levels of comorbidity among refugees (Mollica et al., 1999; Momartin et al., 2004; Nickerson et al., 2017). It is possible that this class may map onto the group of individuals who meet criteria for psychological disorders and are in need of clinical intervention. Indeed, a research synthesis of high-quality studies implementing diagnostic assessments with representative samples yielded prevalence rates of 15% for PTSD and 17% for depression in conflict-affected samples (Steel et al., 2009; World Health Organization [WHO], 2013). These rates are similar to the 19% of participants that comprised the pervasive class in this study. This interpretation is supported by the finding that this group reported the poorest overall health and was most likely to have received help for emotional problems, suggesting that they are accessing mental health services at a greater rate than other classes.
A key finding emerging from this study is that class membership was differentially predicted by types of refugee experiences. Notably, individuals in classes characterized by moderate to high levels of PTSD symptoms had been exposed to significantly more types of traumatic events than those in classes which were characterized by high depression/anxiety symptoms, subclinical PTSD or low symptoms. Participants in the Pervasive Symptom class had been exposed to more types of post-migration living difficulties than individuals in all other classes, and individuals in all symptomatic classes had experienced more types of post-migration living difficulties compared to those in the Low Symptom class. Taken together, these findings suggest that exposure to traumatic events confers specific risk for the development of PTSD symptoms, while exposure to post-migration stressors increases the likelihood of experiencing more a broader array of psychological symptoms. This highlights the critical role that post-migration contextual factors play in influencing mental health in refugee groups and is supported by a growing evidence base indicating that post-migration stressors are associated with psychological distress (Porter & Haslam, 2005, Miller and Rasmussen, 2017). It is thus important that clinicians working with refugees and asylum-seekers take into consideration the potentially deleterious impact of daily stressors on mental health, over and above the effects of past trauma exposure.
This study had a number of limitations. First, the study did not comprehensively assess symptoms of PTSD, depression and anxiety disorders, and therefore conclusions cannot be drawn about the applicability of contemporary diagnostic systems for this sample, and probable diagnosis could not be determined. Furthermore, while it would have been interesting to investigate symptom profiles that incorporated grief responses measured in this study, the low proportion of participants who had experienced loss greater than 6 months ago (~25%) led us to focus on the PTSD and depression/anxiety symptom profiles in the broader sample. Second, data in this study were primarily obtained via self-report measures rather than clinical interviews. Third, the timeframes in which PTSD symptoms and depression/anxiety symptoms were measured in this study differed, with PTSD symptoms being measured over the past week, while depression/anxiety symptoms were measured over the past month. It may be the case that, if consistent measurement periods had been applied, other symptom profiles may have been identified. Fourth, participants retrospectively reported on exposure to traumatic events which introduces the possibility of recall bias. Fifth, a count measure of exposure to types of potentially traumatic events was implemented in this study, precluding the investigation of whether dosage of exposure within particular trauma categories was associated with class membership. Finally, measures implemented in this study were not specifically adapted to each of the cultural groups who took part; nevertheless, gold-standard translation methods were implemented.
This study implemented LCA to investigate the associations between PTSD, depression and anxiety symptoms among a representative sample of refugees resettled in Australia. Findings revealed novel and distinctive symptom profiles that mapped onto specific refugee experiences. These results have important clinical implications in terms of identifying nuanced patterns of symptoms among resettled refugees which may assist with treatment planning and service provision. In addition, the finding that specific refugee experiences were linked to particular symptom profiles provides important information for identifying trauma-affected and displaced individuals who are vulnerable to particular types of psychological symptoms and for informing the development and implementation of interventions.
Supplemental Material
Supplementary_material – Supplemental material for Identifying distinctive psychological symptom profiles among a nationally representative sample of refugees resettled in Australia
Supplemental material, Supplementary_material for Identifying distinctive psychological symptom profiles among a nationally representative sample of refugees resettled in Australia by Angela Nickerson, Dusan Hadzi-Pavlovic, Ben Edwards, Meaghan O’Donnell, Mark Creamer, Kim L Felmingham, David Forbes, Alexander C McFarlane, Derrick Silove, Zachary Steel, Miranda van Hoof and Richard A Bryant in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This paper uses unit record data from Building a New Life in Australia: the Longitudinal Study of Humanitarian Migrants (BNLA) conducted by the Australian Government Department of Social Services (DSS). The findings and views reported in this paper, however, are those of the author[s] and should not be attributed to the Australian Government, DSS, or any of DSS’ contractors or partners. doi:10.26193/ZQHBPW. We also acknowledge the Australian Institute of Family Studies (AIFS) who designed, administered and conducted the fieldwork for the BNLA project.
Author Contributions
B.E. contributed to study conception and design; A.N. and D.H.-P. contributed to data analysis; A.N., D.H.-P., B.E., M.O., M.C., K.L.F., D.F., A.C.M., D.S., Z.S., M.v.H. and R.A.B. contributed to the interpretation of data, drafted and revised the article critically for important intellectual content and approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by a National Health and Medical Research Council Programme Grant (#1073041).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.