
Abstract

Schizoaffective disorder, nay the ‘illness’ SAD, is seemingly ubiquitous. Hospital-based public psychiatric services and associated community care programmes across the country are positively brimming with patients that are supposedly ‘schizoaffective’. Of patients diagnosed with a psychotic illness that had contact with public specialised mental health services, 17.5% were diagnosed with SAD using the International Classification of Diseases – 10th Revision (ICD-10), the same prevalence as bipolar disorder (Australian Government Department of Health, 2011). Many of these patients have been assigned this label as a differential diagnosis, but, remarkably, many have SAD as their primary ‘illness’. This is of critical importance because one of the key functions of any diagnosis is to inform treatment, but, as we shall see, although the diagnosis of SAD seemingly serves many purposes, meaningfully informing management is arguably not one of them.
Why is the diagnosis made?
Clinically, the diagnosis comes about because of two sets of factors. The first is a function of time and the second concerns phenomenology.
Severe mood disorders at either pole (depression and mania) can, and do, feature definitive psychotic symptoms. And conversely, psychotic syndromes often manifest in significant and sustained changes of mood, in particular depression. Furthermore, the processes by which these disorders (depression, mania, schizophrenia) develop are unpredictable and, because of this, the clinical picture early in the course of these disorders is often highly variable. In other words, most diagnoses at this time are indeterminate, and although symptoms can be condensed into a variety of syndromes, these are often ephemeral groupings that are prone to change over time (Santelmann et al., 2015). It is usually at this juncture, in a milieu of diagnostic nebulousness, that the term schizoaffective is introduced. Part of the reason is to provide an interim ‘working diagnosis’, one which can be revised when more information comes to light. However, in practice, once the diagnosis of SAD is conferred, it is seldom supplanted – partly because of the hierarchy within our taxonomies and partly because once a criterion of psychosis has been met it is difficult to revert to a diagnosis of mood disorder only. Hence, diagnoses such as schizophrenia or bipolar disorder may later be added, but the label of schizoaffective remains firmly ensconced.
Other reasons for the use of SAD include a desire to avoid more stigmatising labels. SAD is seemingly more acceptable than schizophrenia, which has dire connotations akin to the diagnosis of cancer (Malaspina et al., 2013). This is particularly relevant early in the course of the illness or in young individuals where it is felt that acceptance of the diagnosis, either by the individual or by their family, is likely to be poor. Cloaking an emerging psychotic syndrome in a ‘schizoaffective cape’ allows the true diagnosis (e.g. schizophrenia) to be revealed gradually, giving everyone time to adjust to the reality of a severe and disabling chronic mental illness.
A diagnosis of SAD is also sometimes made at the point of prescribing medication, and this expedient practice is especially prevalent in the United States, where some medications can only be prescribed if the individual has a diagnosis that is specified in the Diagnostic and Statistical Manual of Mental Disorders (DSM). For example, diagnosing SAD allows the prescription and cost of antipsychotics to be paid for through medical insurance. The problem with this, apart from the obvious clinical and ethical issues of knowingly misdiagnosing an illness, is that SAD epidemiological and treatment data derived from insurance company databases is likely to be inaccurate and potentially misleading.
What are the criteria for SAD?
The lack of a clear consensus on the core features of SAD is evident in the stark differences between ICD-10 and the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5). Both classification manuals stipulate that, in SAD, schizophrenia symptoms and those of a mood episode occur coterminously; however, this is where the similarities more or less end. The duration of the dysfunction, the degree to which the mood and psychotic symptoms co-occur, and even which symptoms are necessary to satisfy the requirements for the diagnosis differ between the two manuals (see Table 1).
Timeline of diagnostic criteria for SAD.
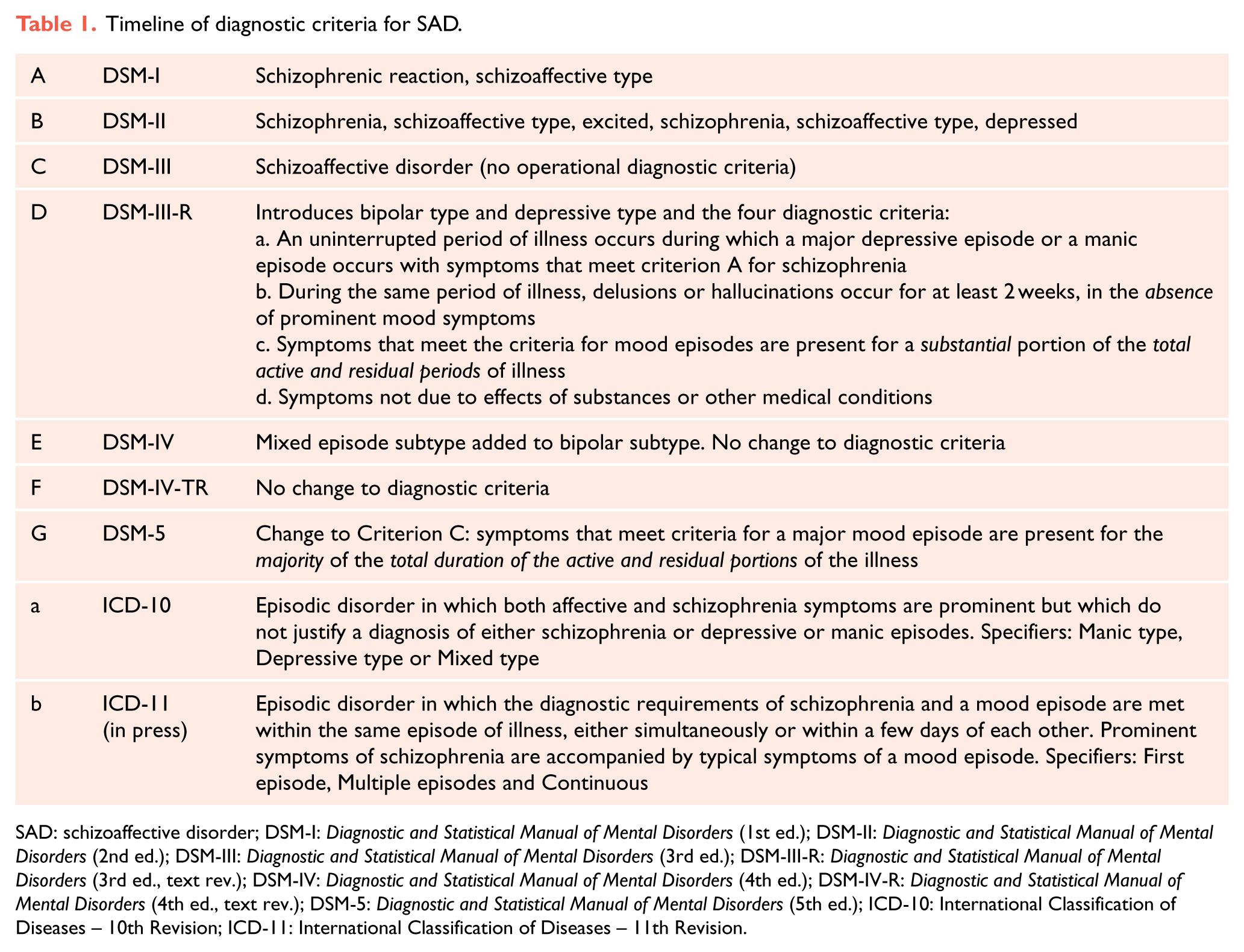
SAD: schizoaffective disorder; DSM-I: Diagnostic and Statistical Manual of Mental Disorders (1st ed.); DSM-II: Diagnostic and Statistical Manual of Mental Disorders (2nd ed.); DSM-III: Diagnostic and Statistical Manual of Mental Disorders (3rd ed.); DSM-III-R: Diagnostic and Statistical Manual of Mental Disorders (3rd ed., text rev.); DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); DSM-IV-R: Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.); DSM-5: Diagnostic and Statistical Manual of Mental Disorders (5th ed.); ICD-10: International Classification of Diseases – 10th Revision; ICD-11: International Classification of Diseases – 11th Revision.
The general diagnostic criteria for SAD have remained almost identical for over 30 years (Diagnostic and Statistical Manual of Mental Disorders [3rd ed., text rev.; DSM-III-R], 1987; see Figure 1). After initially being described as a subtype of schizophrenia, to then being considered an additional psychotic disorder, the criteria for SAD have largely remained unchanged thereafter.

Timeline of SAD diagnostic criteria in DSM and ICD. Dates and letters for each edition of DSM (red) and ICD (blue) correspond to letters shown in Table 1.
What is needed for a diagnosis?
The diagnostic criteria for SAD detailed in DSM-5 are presented schematically in Figure 2.
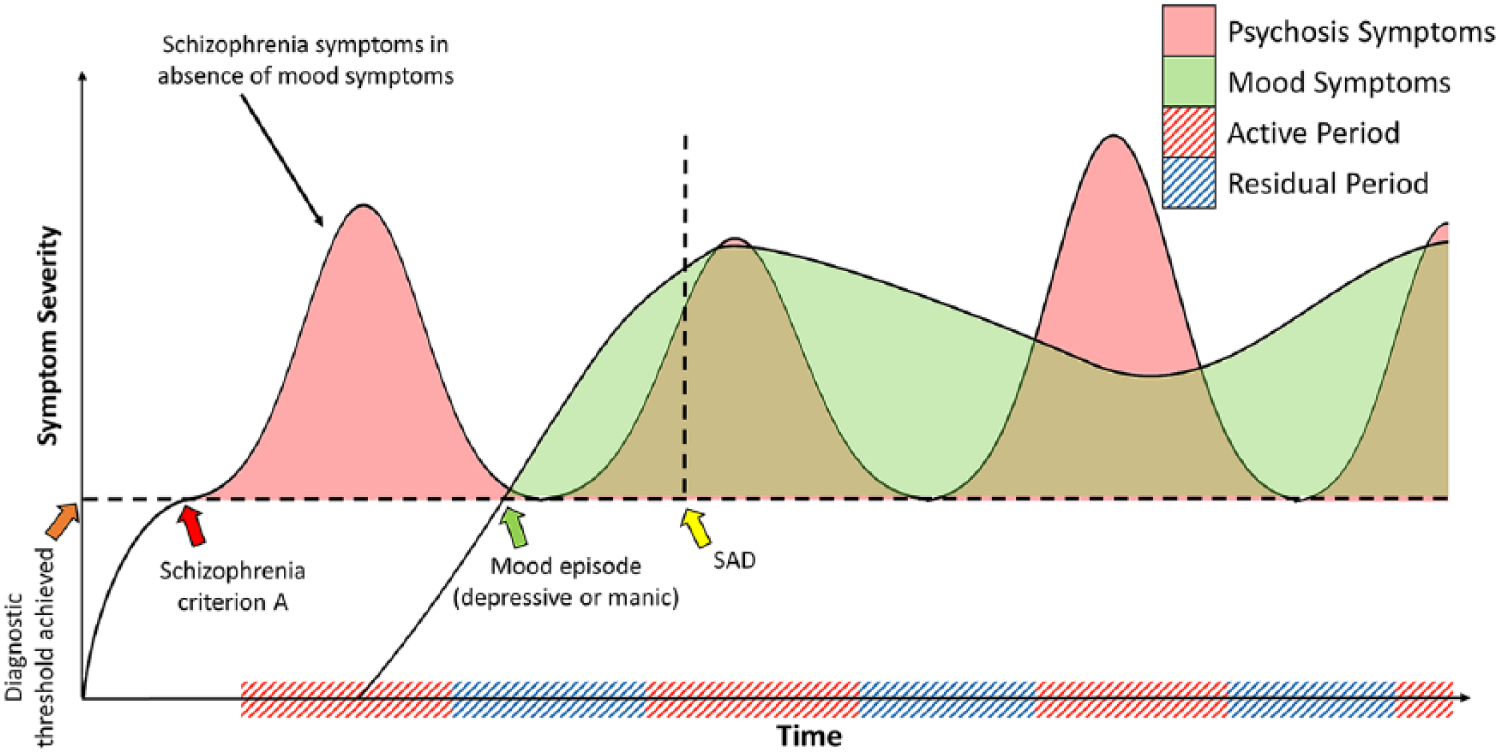
Development of SAD: specifying the diagnostic criteria as per DSM. Active and residual periods refer to schizophrenia symptoms. And active periods of schizophrenia symptoms must last at least 4 weeks (1 month). Mood episodes can be either depression or mania (lasting at least 2 weeks and 1 week, respectively). Once both the criterion A schizophrenia threshold and mood episode threshold have been achieved, SAD can be diagnosed once there is sufficient co-occurrence of the two sets of symptoms.
Criterion C (see Table 1, DSM-III-R) can be especially problematic for clinicians, because attempting to retroactively map a patient’s illness is difficult and subject to recall inaccuracy. Furthermore, this criterion requires that mood symptoms be present for the majority of the illness, meaning that, technically, a patient who has had a decade of psychotic symptoms (active and residual) but co-occurring mood symptoms for only the last 2 years of this period would not qualify for the diagnosis of SAD. In addition, the criterion fails to assign sufficient weighting to recent symptoms – all of which make it unnecessarily complicated; and coupled with the vagueness of the remaining SAD criteria, diagnostic decision-making becomes needlessly difficult.
The conceptualisation of SAD and barriers for clinicians
The importance placed on psychotic symptoms within SAD in both ICD-10 and DSM-5 has meant that affective symptoms are regarded as appurtenances. This hierarchy is completely arbitrary, in no way reflects clinical presentations (e.g. psychotic mania and depression) and does not enhance diagnostic clarity for clinicians. This is exemplified in the test–retest reliability of SAD being consistently lower than that of schizophrenia, bipolar disorder and unipolar depression (Santelmann et al., 2015).
These problems concerning the conceptualisation of SAD can be illustrated by portraying psychotic symptoms and mood symptoms as two peaks reflecting separate aetiologies, which happen to co-occur at times because of overlap temporally, which gives rise to the diagnosis of SAD (Figure 3(a), yellow triangle). However, the current diagnostic criteria for SAD could also reflect the full complement of mood symptoms nesting within a broader umbrella of psychotic symptoms (Figure 3(b), dashed outline). Importantly, under the current conceptualisation of SAD, we have no way of determining which of these models, if any, best capture the clinical manifestations of SAD and whether they are of research value as regards the underlying mechanisms of SAD.
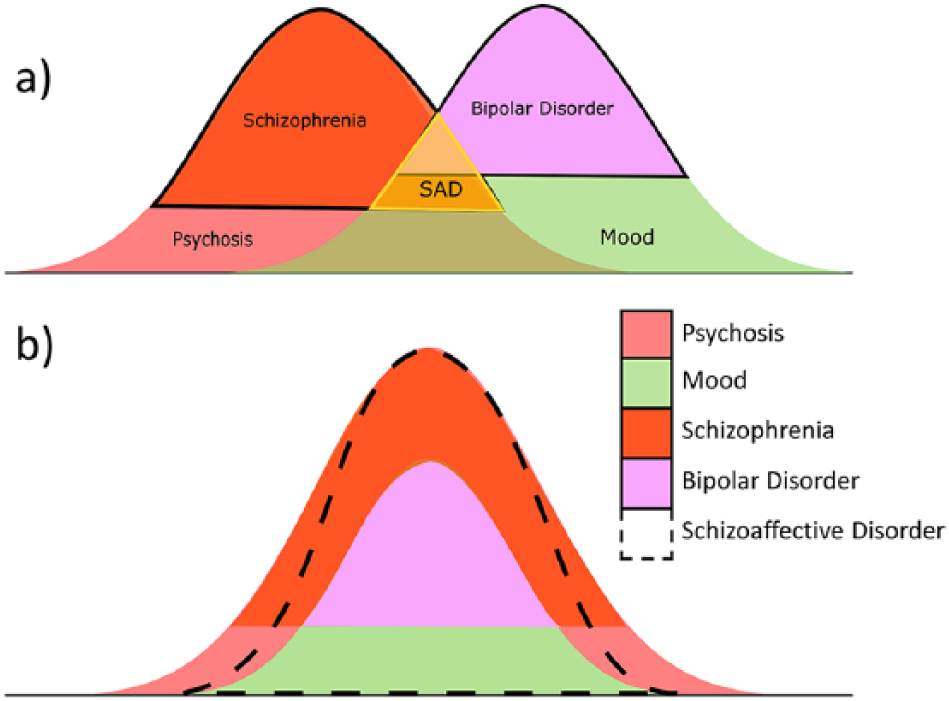
Schematic conceptualisations of SAD according to current diagnostic criteria: (a) the significant overlap of SAD with the psychosis peak, reflecting the emphasis on psychotic symptoms in the absence of mood symptoms; (b) SAD within.
What can be improved here and now?
The ideal solution would be to expunge SAD altogether from both the DSM and ICD – as it is not a separate entity and because the clinical diagnosis lacks reliability and validity (Cheniaux et al., 2009). However, until any such revision takes place, it is important to recognise the many shortcomings of the SAD label and attempt to make pragmatic use of it, noting that this does not reflect any deep understanding.
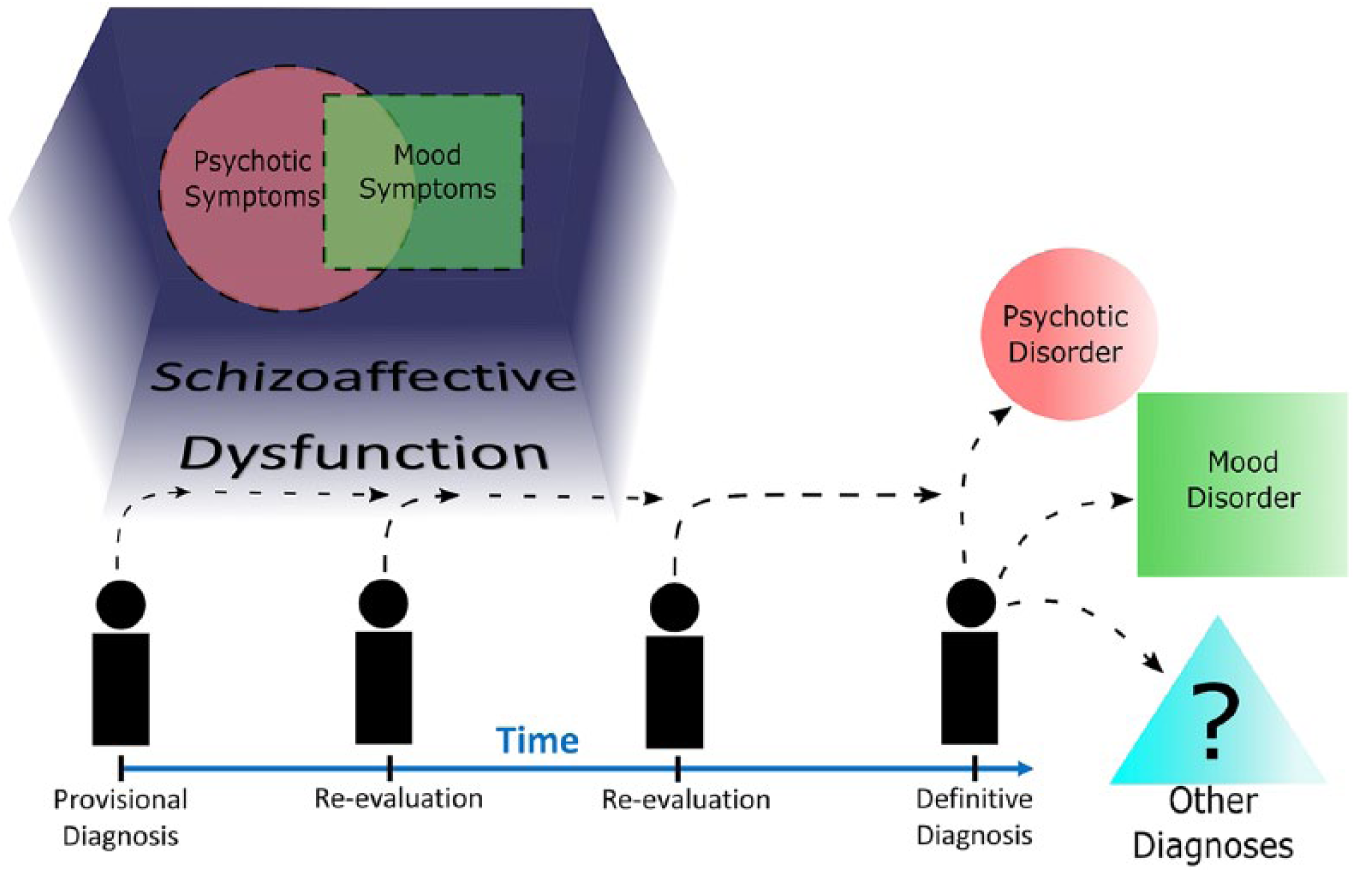
A pragmatic solution that would aid clinicians in navigating prescription legislation would be to replace the term ‘disorder’ with a more accurate specifier – ‘dysfunction’. This would allow the acronym SAD to remain, and the new label of ‘schizoaffective dysfunction’ could continue to fulfil some of its current roles. However, critically, the fact that it is not a disorder would ensure ongoing re-evaluation until a definitive diagnosis can be assigned. Clinically, the key benefit of using schizoaffective dysfunction to describe the overlap of mood and psychotic symptoms is that it does not reify the clinical syndrome as a separate illness or disease. Furthermore, this new label allows for re-evaluation and modification of the label itself and provides clinicians the necessary flexibility to reclassify patients as the illness progresses and evolves (Figure 4).
Schizoaffective dysfunction – a new pragmatic conceptualisation of overlapping symptoms of psychosis and mood.
Research into schizoaffective dysfunction needs to be stepwise. This is because the definition is still partly based on the diagnostic criteria for schizophrenia. Therefore, initially, the underlying neurobiological mechanisms of schizophrenia need to be better understood before schizoaffective dysfunction can be meaningfully explored. But as new developments in the understanding of schizophrenia and mood disorders come to light, the label schizoaffective dysfunction can be refined, and ultimately better defined.
Fake Views
In an age where everything is seemingly fake, this series examines contentious ideas and concepts in psychiatry in search of the truth.
Footnotes
Declaration of Conflicting Interests
G.S.M. has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier, and has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka and Servier. E.B. declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.