
Abstract

Of children and adolescents with mental disorders, only a small fraction will need psychiatric hospitalization (Cotgrove, 2013; James and Worrall-Davies, 2015). The admission decision is not taken lightly as psychiatric hospitalization may be traumatizing through separation from parents and witnessed or experienced violence. Further risks include the adoption of maladaptive behaviours observed in others, regression, dependence and stigmatization. Intensive outpatient treatment, when sufficiently resourced, is preferable to hospitalization as it achieves comparable outcomes at less cost and with less disruption to children and their families (James and Worrall-Davies, 2015). Here, we aim to distil generalizable reasons to admit a child or adolescent to a psychiatric hospital, acknowledging the limited evidence on the topic.
General factors
There are general factors that influence decision-making regarding the psychiatric hospitalization of children and adolescents. There is an expectation that parents take reasonable responsibility for appointment attendance, administering medication, family-based treatment participation and maintaining safety. The trigger for hospitalization, therefore, is when the severity of illness means that family is unable to undertake these tasks despite the application of available community resources. Referral pathways also differ for adults with a mental disorder whereby community mental health workers, ambulance staff or police officers are agents commonly involved in the decision to hospitalize; while for young people, it is more typical for parents, child protection agency and education services to be involved. We are more likely to admit a young person if, for example, both the parents and education staff report severe dysfunction. However, inadequate social support alone is not a reason for admission (see Decision tree in Figure 1).
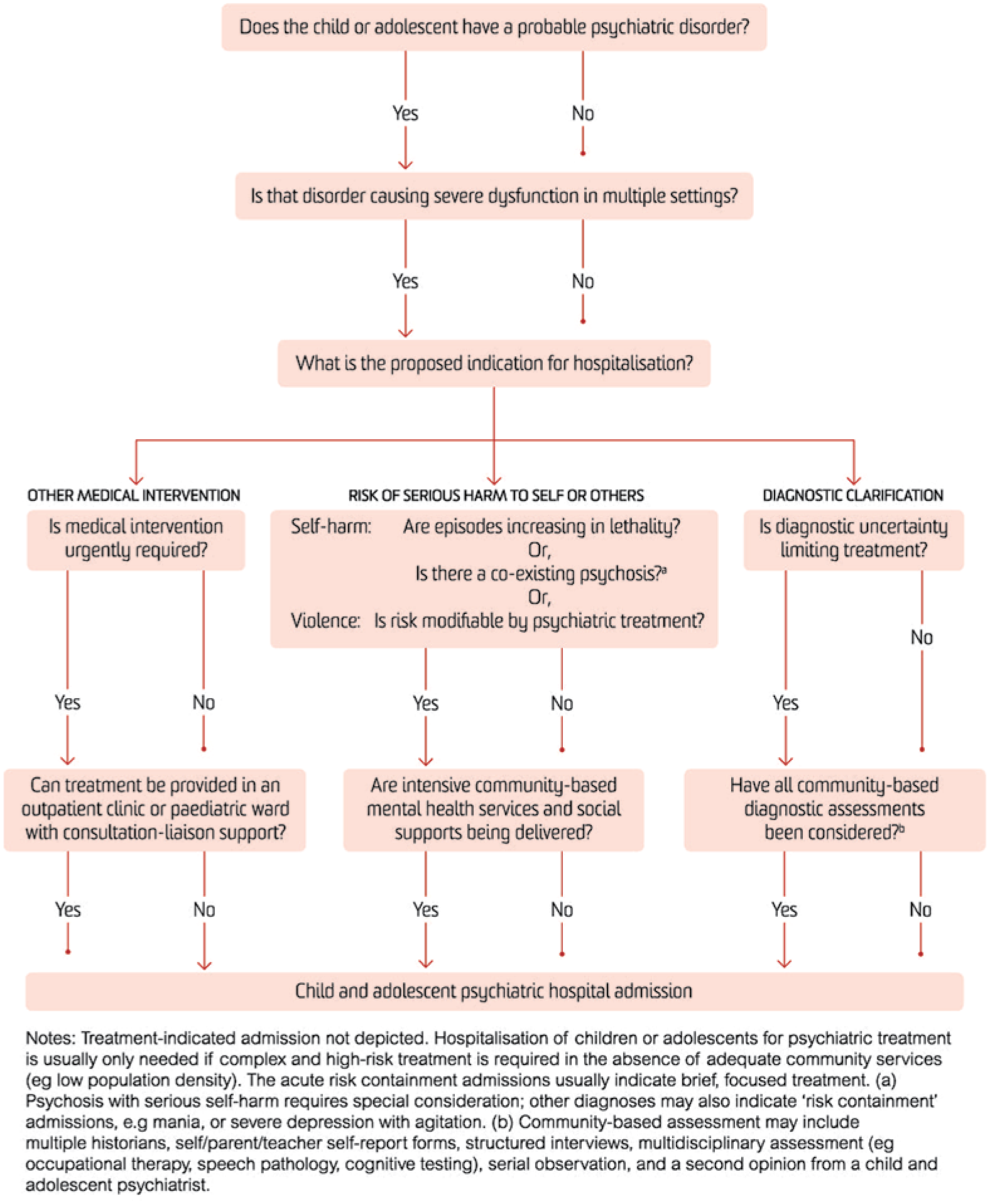
Decision tree: child and adolescent psychiatry hospital admissions.
The admission decision weighs patient, family and health service factors; hence, there is geographical variance in admission patterns. Psychiatric hospitalization of children and adolescents is likely to be more productive if both parents and treating community clinicians support the admission, families participate in the treatment and both parents and community clinicians participate in discharge planning and assertive follow-up (James and Worrall-Davies, 2015).
Admission indications
Research and expert opinion coalesce into three principal indication categories (see Figure 1): (1) a period of detailed observation to facilitate diagnosis, (2) acute containment of risk and supervised initiation of treatment and (3) non-psychiatric medical assessment or treatment that cannot, because of the child’s condition, be undertaken in a general medical setting (Indig et al., 2017). These indications presuppose a psychiatric disorder causing marked multidimensional functional impairment refractory to community resources. Risk containment appears the most common reason for a request for psychiatric hospitalization of children and adolescents (O’Herlihy et al., 2008).
Diagnostic clarification
Psychiatric assessment in hospital cannot replace a thorough community-based multidisciplinary assessment (Leckman et al., 2017). However, 24-hour observation in a controlled environment may serve several functions. It can resolve ambiguity about transient phenomena such as mood elevation or psychotic symptoms. It affords the observation of the young person isolated from perceived exacerbating factors. Careful observation may also identify factitious symptoms and Munchausen syndrome by proxy.
Acute containment of risk and treatment
Self-harm and suicide risk warrant hospitalization if the risk cannot be contained by intensive and assertive outpatient treatment (if available). Recurring episodes of self-harm with increasing lethality are a ‘red flag’. Low lethality self-harm, such as superficial cutting, is better managed in the community. Self-harm in the presence of concurrent psychosis makes the situation volatile and unpredictable; hence, hospitalization is typically required for stabilization. The risk of violent (or other) harm to others is determined by a similar rationale to adult patients, that is, hospital admission is indicated when the risk of harm is likely to respond to psychiatric treatment, such as in the case of suspected or confirmed mania or psychosis.
Child and adolescent psychiatrists draw on community resources to support the administration of regular and pro re nata medications in addition to engagement with non-pharmacological interventions. Family-based therapies (indications include eating disorders, obsessive–compulsive disorder, bipolar disorder, psychosis and oppositional defiance disorder) are best conducted with the family living in their home. Hospitalization is therefore best reserved for situations where the treatment is high risk and complex and where community support is not accessible. Examples of high risk and complex include the need for parenteral administration and the cross taper of medications where there are significant risks for drug interactions.
Other medical intervention
Psychiatric hospitalization of children for other medical assessment or treatment, unmanageable on a paediatric ward, is sometimes indicated, for example, an emotionally dysregulated child with autism spectrum disorder who needs investigation for seizures. The risks of psychiatric hospitalization, as always, need consideration. And questions need to be asked: Can the procedure be carried out on an outpatient basis? Could consultation-liaison psychiatry support paediatric ward staff to manage challenging behaviour?
Other requests for psychiatric hospitalization
Hospitalization is sometimes requested to resolve problems other than from the three categories reviewed above (see Figure 2). Usually, these problems can be managed outside the psychiatric inpatient setting if appropriate resources are provided. There may be a request to transfer a child out of a medical bed due to disruptive behaviour. The recommended action here is an intervention on the ward from the consultation-liaison team. Welfare agencies may seek hospitalization as a form of out-of-home-care placement to address child protection concerns; this carries the risk of a prolonged admission with pathologizing and scapegoating of the child. If the child is thought to have been abused and requires forensic assessment, the paediatric ward offers a less stigmatizing environment. Otherwise, the preferred solution is emergency foster care or other out-of-home placement. Hospitalization may be sought by parents or clinicians as respite from the management of conditions that are unlikely to respond to inpatient treatment. Examples include behavioural disturbance associated with intellectual disability, borderline personality disorder, autism or substance use. A planned time-limited admission may be warranted, but there should be more sustainable avenues for respite available within the community.
Other requests for the psychiatric hospitalization of children.
The evidence for indications of psychiatric hospitalization for children and adolescents is limited. But clinicians, often in emotionally heightened and time-pressured settings, must make decisions. We hope the framework outlined above will inform them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.