
Abstract
Background:
Stepped care has been promoted for the management of mental disorders; however, there is no empirical evidence to support the cost-effectiveness of this approach for the treatment of anxiety disorders in youth.
Method:
This economic evaluation was conducted within a randomised controlled trial comparing stepped care to a validated, manualised treatment in 281 young people, aged 7–17, with a diagnosed anxiety disorder. Intervention costs were determined from therapist records. Administrative data on medication and medical service use were used to determine additional health care costs during the study period. Parents also completed a resource use questionnaire to collect medications, services not captured in administrative data and parental lost productivity. Outcomes included participant-completed quality of life, Child Health Utility – nine-dimension and parent-completed Assessment of Quality of Life – eight-dimension to calculate quality-adjusted life years. Mean costs and quality-adjusted life years were compared between groups at 12-month follow-up.
Results:
Intervention delivery costs were significantly less for stepped care from the societal perspective (mean difference −$198, 95% confidence interval −$353 to −$19). Total combined costs were less for stepped care from both societal (−$1334, 95% confidence interval −$2386 to $510) and health sector (−$563, 95% confidence interval −$1353 to $643) perspectives but did not differ significantly from the manualised treatment. Youth and parental quality-adjusted life years were not significantly different between groups. Sensitivity analysis indicated that the results were robust.
Conclusion:
For youth with anxiety, this three-step model provided comparable outcomes and total health sector costs to a validated face-to-face programme. However, it was less costly to deliver from a societal perspective, making it an attractive option for some parents. Future economic evaluations comparing various models of stepped care to treatment as usual are recommended.
Introduction
Individual or group cognitive behavioural therapy (CBT) is the treatment of choice for children and adolescents diagnosed with anxiety disorders (James et al., 2015; Rapee et al., 2009; Reynolds et al., 2012). These psychological interventions have demonstrated efficacy with 50–60% of youth remitting from their anxiety diagnosis. Low-intensity psychological interventions based on CBT such as bibliotherapy, guided self-help and Internet-based CBT also have effectiveness (Arnberg et al., 2014; Cuijpers et al., 2010) and cost-effectiveness (Donker et al., 2015) credentials to support their use in the treatment of some anxiety disorders in adults. Support for these methods with children is growing (Pennant et al., 2015; Rapee et al., 2006; Thirlwall et al., 2013).
The concept of stepped care has been promoted as a means to reduce health care costs without compromising effectiveness (Bower and Gilbody, 2005). The least intensive intervention is delivered first, with more intensive interventions adopted for individuals who do not respond to initial treatment. This approach has been increasingly promoted for the management of mental disorders (Australian Government Department of Health, 2016; National Institute for Health and Care Excellence [NICE], 2010). However, the empirical evidence to support the efficacy and cost-effectiveness of stepped care for the management of anxiety disorders is limited (Ho et al., 2016). Our team have conducted the first trial in youth and compared the efficacy of a three-step intervention to an empirically validated CBT programme (Rapee et al., 2017). The results demonstrated that stepped care provided similar outcomes in terms of remission rates compared to standard care with face-to-face CBT but used less clinician time. This study reports on the cost-effectiveness of this trial from societal and health sector perspectives.
Method
The study protocol including the collection of data on medication and medical service utilisation for use in the economic evaluation was approved by the Department of Health (EC00106), Macquarie University (EC00124) and Deakin University (EC00213) human research ethics committees. This trial was prospectively registered on the ANZ clinical trials registry (CTRN12612000351819). Participants in the stepped care trial also completed the economic measures as reported in this study. Details of the stepped trial methodology and primary study results have been previously published (Rapee et al., 2017). In brief, participants were recruited through a university clinic in New South Wales between August 2012 and May 2014. Participants were screened to determine suitability and then completed a structured diagnostic interview with a trained clinician. Inclusion criteria were as follows: between 7 and 17 years of age, met diagnostic criteria for an anxiety disorder as their primary (most interfering) disorder and were willing to be randomised to the study treatments. Parents and children provided signed informed consent to enter the trial. Eligible participants were randomly assigned to receive either an empirically validated, manualised programme (Cool Kids) or stepped care. A flow chart of participant movement through the trial is provided in Figure S1 (supplementary materials).
Interventions evaluated
The control condition was the manualised Cool Kids programme consisting of 10 face-to-face, 60-minute individual sessions over 12 weeks with a therapist following a structured CBT programme that included psychoeducation, cognitive restructuring, exposure as well as social and problem-solving skills (Arendt et al., 2016; Hudson et al., 2009; Rapee et al., 2006).
Participants allocated to the stepped care group could receive up to three steps. Step 1 comprised a therapist-assisted, low-intensity intervention (CBT via printed or CD-ROM materials) (Rapee et al., 2006; Wuthrich et al., 2012). Therapists provided parents of children (<13 years) with up to four 30-minute sessions over the telephone that focused on support, motivation and guidance. Adolescents (>12 years old) received up to four 40-minute calls from a therapist with the time divided between the young person and a parent. Step 2 followed the standard, manualised, Cool Kids programme, although the number of sessions could be reduced based on the judgement of the therapist to avoid redundancy. If required, Step 3 comprised up to 12 sessions of individually tailored CBT (Rapee et al., 2017). At each step, the qualifications and experience of the therapist increased. Step 1 therapists were undergraduate psychology students and trainees required to follow structured guidelines. The Cool Kids and Step 2 therapists were nationally registered psychologists. Step 3 therapists had postgraduate clinical psychology degrees and had worked specifically with anxious youth for 1–5 years.
Resource use and costs
The economic perspective of this study was societal with a secondary analysis from the Australian health sector perspective as recommended by the Second Panel on Cost-Effectiveness in Health and Medicine (Sanders et al., 2016). The health sector costs included the resources required to deliver the stepped care or Cool Kids comparator interventions (largely the time of the health professionals) as well as the cost of health care resources (patient out of pocket and government-reimbursed costs) used by the participants over the trial period. Societal costs consisted of the health sector costs plus an estimate of the parental time required for intervention delivery in addition to self-reported parental lost productivity. An impact inventory with details of specific costs by perspective is listed in Table S1 (supplementary materials).
The intervention costs were calculated based on detailed records for the number, length, type of contact and the level of training of the clinician making contact with each participant or parent. The health sector costs included the cost of the self-help materials (book or CD-ROM) provided in Step 1 of the stepped care intervention as well as the cost of the clinician contact based on the number of hours and multiplied by an hourly wage with on-costs as provided in Table S2 (supplementary materials).
For the societal perspective, assumptions were made about the amount of parental time required for intervention delivery. The additional cost of parental time involved in the delivery of the Step 1, low-intensity intervention, was calculated by multiplying the estimated hours of parental involvement by a leisure time wage rate (25% of the average wage rate) of $12.47/hour (Australian Bureau of Statistics, 2014; Jacobs and Fassbender, 1998). In Step 1, participants over the age of 12 independently worked through a CD-ROM describing therapeutic techniques and exercises, while parents of children under the age of 13 worked through chapters in a book. It was assumed that for each chapter completed, 1 hour of parental time would have been spent working through the relevant material. The number of chapters completed was collected from parents each time the therapist called. If the child was under the age of 13, the parent spent the entire time on the phone during the therapist call. For children over 12, it was estimated that the parent spent only a quarter of the time on the phone with the child using the remaining time.
For Steps 2 and 3, as well as the comparator of Cool Kids, parental time was costed using an average wage rate plus overhead costs of $49.87 (Australian Bureau of Statistics, 2014) since the face-to-face sessions for these steps occurred during normal working hours. It was assumed that one parent would be required to transport their child to the sessions and would not be able to work either in paid or unpaid activities (relevant for home-based parents) while the session was being delivered.
Participants or their parents (dependent on age) had the option of providing consent to access Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data over a 15-month period (3 months prior to the baseline assessment and up to the 12-month follow-up). The parents of participants were also asked to complete a questionnaire to gather data on additional health care resources used by their child. For the participants who provided MBS/PBS consent, the questionnaire asked for over-the-counter medication and supplement use, non-Medicare listed service use, out-of-pocket fees and hospitalisations as well as time off from usual activities to care for their child. For participants who chose not to consent to provision of MBS/PBS data, a more detailed questionnaire requested information on health care provider visits covered by the MBS and prescription medications covered by PBS.
The PBS data provided the patient contribution and the amount paid by the government for each prescription medication through this scheme. The MBS data similarly provided the total provider charge as well as the government benefit paid and the out-of-pocket costs. For participants who did not provide access to MBS/PBS data, standard PBS unit costs for medications were applied to each prescription medication reported (PBS, 2014). Health professional consultations were costed using a weighted average unit cost for each consultation type (i.e. general practitioner, psychiatrist etc.) based on standard MBS item reports (Australian Government Department of Human Services, 2017) as shown in Table S3 of the supplementary data. Medications and supplements not covered by PBS would be paid out of pocket by participants’ parents and were costed using online retail pharmacy sites (Chemist Warehouse, 2016). The reported reason and length of stay for hospital visits were used to assign a cost based on standard Australian public sector hospital costs (Independent Hospital Pricing Authority, 2016). Total costs to the government and the out-of-pocket costs paid by the parents of participants were summed for the 3-month period before the trial to represent baseline health sector costs. Parental lost productivity for the 3 months before the trial was added to health sector costs to derive baseline societal costs. Total costs were then summed over the 12 months after trial entry.
All costs are represented as 2015/2016 Australian dollars. Because the costing and outcomes were collected over five separate financial years, discounting was applied. Price indices were calculated based on the Australian Institute of Health and Welfare total health price index.
Outcomes
The primary outcome measure for the base case analysis was quality-adjusted life years (QALYs) for the youth. QALYs were derived by weighing the length of life spent in a particular health state by the utility of that health state. Utility values (or weights) are constrained between 0 and 1 where 0 refers to death and 1 refers to perfect health. A multi-attribute utility assessment, the Child Health Utility – nine-dimension (CHU-9D) was completed by participants at baseline and end point. The CHU-9D is a nine-item, generic paediatric preference-based measure of health-related quality of life which also provides utility values (Stevens, 2011). An Australian adolescent-specific scoring algorithm that uses preference weights derived from profile case best–worst scaling methods in young people was used for this study (Ratcliffe et al., 2016).
To assess the utility for parents of participants, the Assessment of Quality of Life – eight-dimension (AQOL-8D) was completed at each assessment. This 35-item multi-attribute utility instrument was chosen since it potentially has greater sensitivity to mental health quality of life domains compared to the EuroQol five-dimension (EQ-5D) (Mihalopoulos et al., 2014). The preference weights in the utility algorithm used in this study were derived from the Australian general population (Centre for Health Economics, 2014). The area under the curve method was applied to calculate QALYs separately for children and parents (Glick et al., 2015).
Statistical analysis
Analyses were conducted using Excel 2013 and STATA 15 (StataCorp LP, College Station, TX, USA).
The base case analyses were undertaken as intention to treat (ITT). All enrolled participants who completed a baseline assessment were included; however, 8% of participants did not provide MBS/PBS data, complete a follow-up resource use questionnaire or CHU-9D. The missing at random assumption required for multiple imputation was tested through a series of logistic regressions comparing participant characteristics for those with and without missing end point data. To account for missing health care costs and utility data, the ICE multiple imputation technique in STATA was used (Royston and White, 2011) with baseline utility, total costs, participant age and sex used as predictors for imputation. The total costs of health care resources, lost productivity and QALYs at 12-month follow-up were imputed eight times based upon the amount of missing data (White et al., 2011).
Generalised linear models (gamma family, log link), using the mim command to combine the estimated coefficients across the imputed data sets, were used to determine the size and significance of differences between groups for total costs due to the skewness of both cost and QALYs. Two-part multivariate models were used when calculating the differences for the specific cost categories (i.e. medications, health professional visits) due to the number of participants reporting zero costs (Glick et al., 2015). Generalised linear models (Gaussian family, identity link) were used to evaluate between-group differences in QALYs. For each cost and outcome, unadjusted models were developed along with models incorporating the covariates of age, gender, baseline utility or baseline cost as appropriate.
Incremental cost-effectiveness ratios (ICERs) were calculated as the difference in average cost between the stepped care intervention and the Cool Kids comparator divided by the difference in average QALYs between the two groups. To determine the sampling uncertainty, nonparametric bootstrapping was performed in STATA which provided the 95% confidence intervals (CIs) for the incremental cost per QALY calculated. In total, 1000 iterations were performed and graphically represented on a cost-effectiveness plane.
Sensitivity analyses
The results from participants with completed data were compared to the ITT data set that used multiple imputation. One-way sensitivity analyses were undertaken to explore the effect of underlying assumptions on the results. To reflect the likely cost to the government, the intervention delivery cost was varied using the MBS-reimbursed benefit per contact as an alternative to the hourly wage rate for personnel time (Table S4 – supplementary materials). There may also be the possibility of double counting parental productivity so we removed the cost of parental time involved in the delivery of the intervention from the societal costs as an additional sensitivity analysis.
Results
The 281 randomised participants were well matched across the two groups at baseline. As shown in Table 1, baseline utility values for children and their parents were similar between the two groups. The percentage of participants consenting to the use of MBS/PBS data was not significantly different between groups. Mean health sector and societal costs in the 3 months preceding participation in the study were comparable between groups.
Participant baseline data mean (SD) unless specified otherwise.
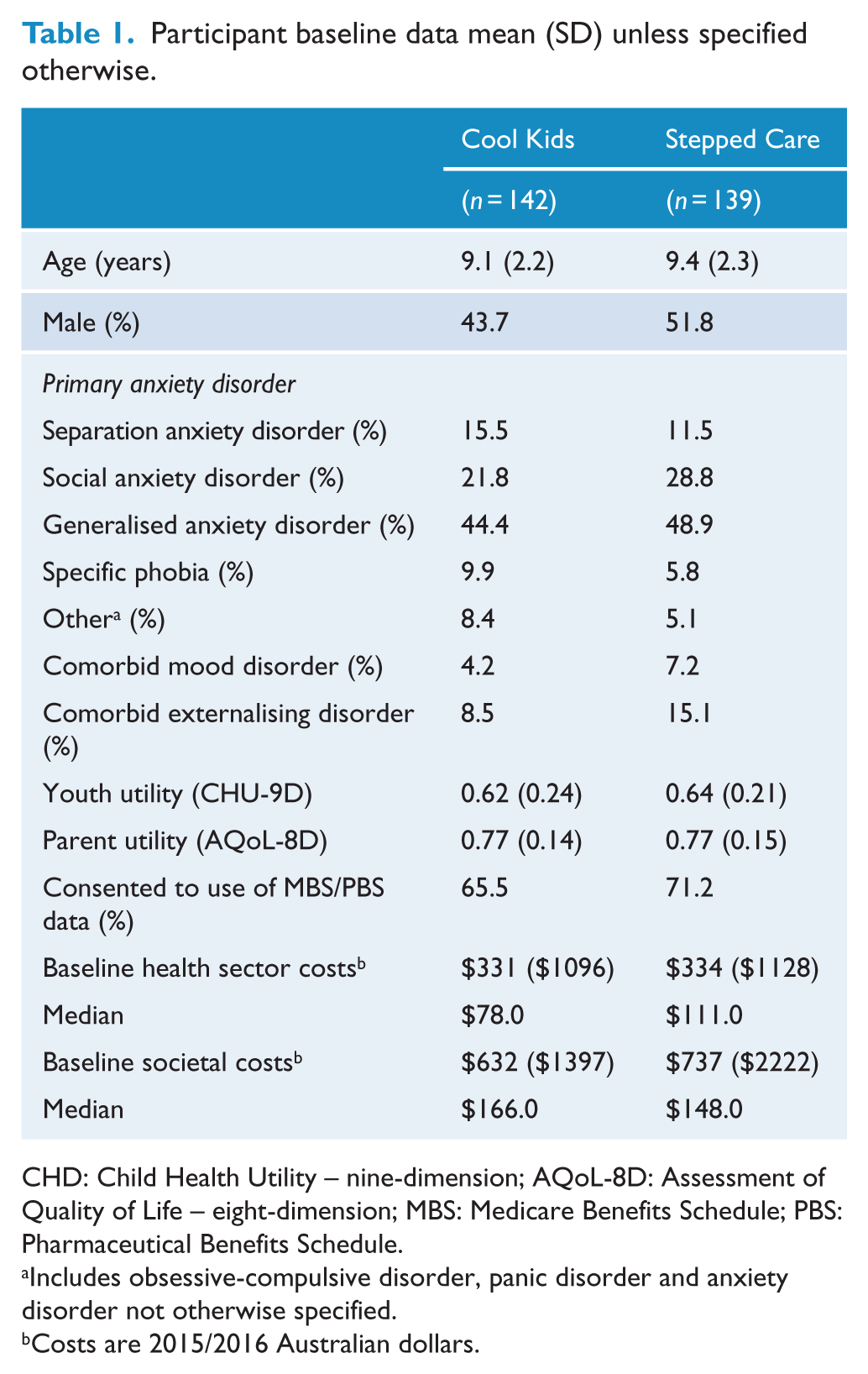
CHD: Child Health Utility – nine-dimension; AQoL-8D: Assessment of Quality of Life – eight-dimension; MBS: Medicare Benefits Schedule; PBS: Pharmaceutical Benefits Schedule.
Includes obsessive-compulsive disorder, panic disorder and anxiety disorder not otherwise specified.
Costs are 2015/2016 Australian dollars.
Table 2 provides detailed intervention delivery costs for each step as well as the overall cost from societal and health sector perspectives. The mean cost of delivering the entire stepped care intervention was significantly lower than the comparator from the societal perspective (mean difference $198; p = 0.034). The mean cost of delivering the stepped care intervention was also less than the comparator from the health sector perspective, but was not statistically significant (mean difference $129; p = 0.056).
Intervention delivery costs by perspective.
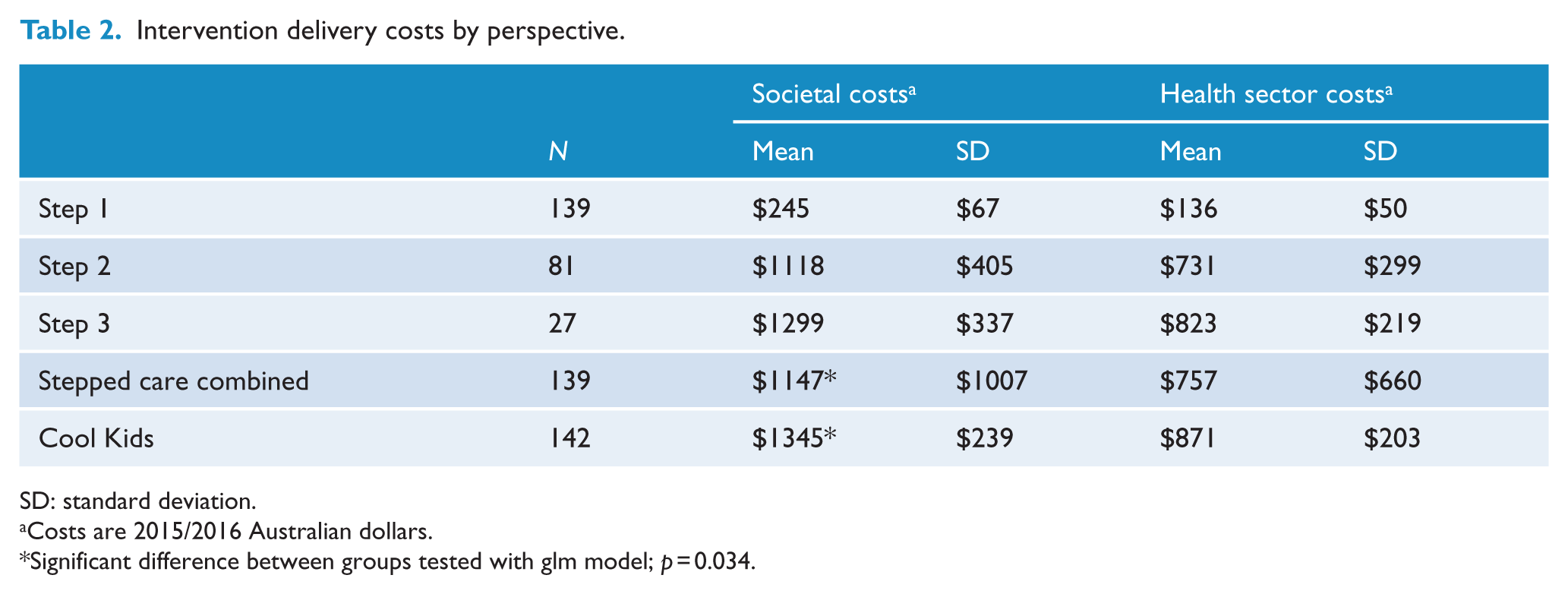
SD: standard deviation.
Costs are 2015/2016 Australian dollars.
Significant difference between groups tested with glm model; p = 0.034.
The cost of medications, health professional services, hospital visits and parental productivity were lower for the stepped care group as shown in Table 3; however, none of these differences were statistically significant.
Group means and differences for specific cost categories at 12-month follow-up.

SE: standard error; CI: confidence interval.
Costs are 2015/2016 Australian dollars.
Adjusted mean differences were calculated using a two-part, generalised linear model (glm) adjusted for baseline cost and CHU-9D score, except for the intervention costs which only used the glm adjusted for baseline cost and CHU-9D.
As shown in Table 4, the reference case results using multiple imputation for missing costs and QALYs analysed with generalised linear models revealed no significant differences in mean total costs or QALYs between the two study groups. Mean total societal costs over the 12-month follow-up were $1334 lower for the stepped care group, and mean health sector costs were $563 less than the comparator. The utility values for the participants (CHU-9D) and their parents (AQoL-8D) at the 12-month follow-up had improved for both study groups from the baseline assessment. This led to slightly more but not significant QALYs in the Cool Kids comparator group over the stepped care group (adjusted mean difference for participants −0.011, 95% CI = [−0.037, 0.015]; mean difference for parents −0.002, 95% CI = [−0.014, 0.010]).
Utility values, QALYs and total costs at 12-month follow-up following multiple imputation.
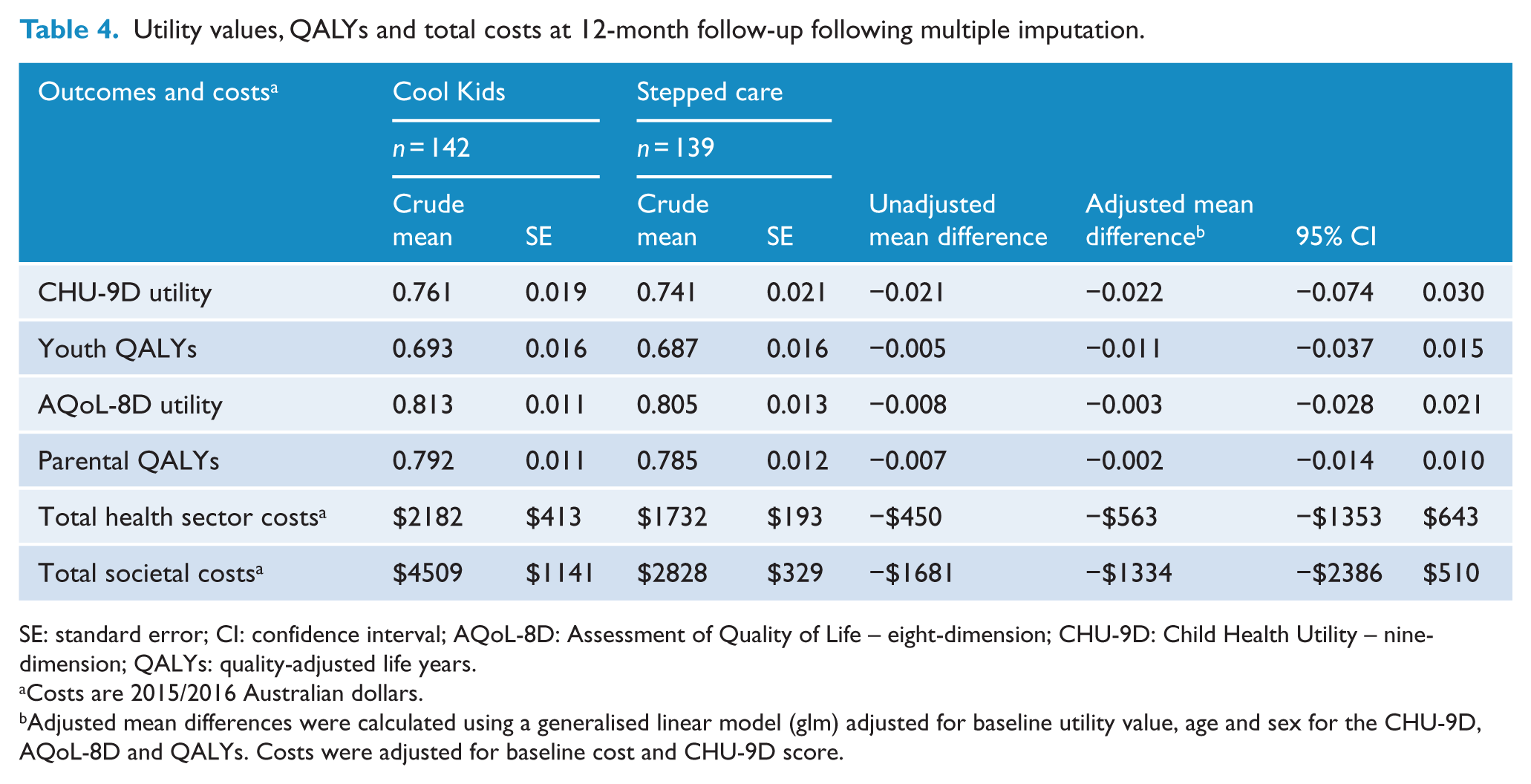
SE: standard error; CI: confidence interval; AQoL-8D: Assessment of Quality of Life – eight-dimension; CHU-9D: Child Health Utility – nine-dimension; QALYs: quality-adjusted life years.
Costs are 2015/2016 Australian dollars.
Adjusted mean differences were calculated using a generalised linear model (glm) adjusted for baseline utility value, age and sex for the CHU-9D, AQoL-8D and QALYs. Costs were adjusted for baseline cost and CHU-9D score.
Cost-effectiveness planes which are scatter plots of the bootstrapped incremental cost and QALYs are shown in Figure 1. From the societal perspective (Figure 1(a)), 37% of the iterations were located in the south-east quadrant indicating that the intervention was more effective and less costly, also referred to as ‘dominant’. There were 59% of iterations falling in the south-west quadrant where the intervention was less costly but also delivered fewer QALYs. The cost-effectiveness plane showing the results from the health sector perspective (Figure 1(b)) was similar with 35% of iterations in the dominant quadrant and 51% in the less costly, less effective quadrant.

Cost-effectiveness planes: (a) societal perspective and (b) health sector perspective.
Sensitivity analysis
The analysis of complete cases provided similar results to the ITT analysis as shown in Table S5 (supplementary materials). The cost-effectiveness planes in Figure S2 (supplementary materials) showed that stepped care resulted in more iterations falling in the dominant quadrant of the cost-effectiveness planes (62% and 54% for the societal and health sector perspectives, respectively).
Using the MBS-reimbursed benefit to cost the intervention delivery resulted in very similar total costs compared to the base case for both health sector and societal perspectives.
When the analysis was modified to remove the cost of the parental time from the intervention, the results from the societal perspective were similar to the base case analysis as demonstrated in Table S5 and Figure S3.
Discussion
This is the first economic evaluation of a stepped care treatment strategy for youth with an anxiety disorder. It provides valuable evidence regarding a stepped care model of treatment hypothesised to be cost-effective. Despite several organisations recommending a stepped care approach for the delivery of mental health services based on the assumption of cost-effectiveness (NICE, 2010; National Mental Health Commission, 2014; New South Wales Mental Health Commission, 2014), there has been little evidence to support this premise (Ho et al., 2016; van Straten et al., 2015).
Our findings suggest that the currently evaluated three-step model of stepped care provides similar outcomes assessed as QALYs and remitted cases (Rapee et al., 2017) at a comparable total cost to an empirically validated, face-to-face psychological therapy from both societal and health sector perspectives. The sensitivity analysis showed that these findings were robust. Previous studies of stepped care in the treatment of adults with anxiety as well as the prevention of depression demonstrated that stepped care was cost-effective compared to care as usual (Goorden et al., 2014; Van’t Veer-Tazelaar et al., 2010). In these previous economic evaluations, stepped care was more costly than care as usual but also resulted in improved outcomes (QALYs and diagnoses averted). However, care as usual is not a uniform, empirically validated comparator and many people with mental disorders receive sub-optimal care (Harris et al., 2015; Wang et al., 2005). Therefore, the current findings are important since this is the first comparison of stepped care to a validated, effective treatment.
The cost to deliver the stepped care intervention was on average $198 less from the societal perspective as a result of the lower cost of parental time required to deliver the stepped care intervention. Even though parents were required to spend time working through materials in the Step 1 low-intensity intervention with their children, we made a conservative assumption that this occurred in the parents’ leisure time incurring less cost than the face-to-face sessions received by all participants in the control condition. In addition, 42% of the young people in the stepped care group did not progress to Step 2 and therefore did not incur additional intervention delivery costs. Therefore, the stepped care model is less costly to parental time averaging across the sample and required particularly less time for families that recover after Step 1.
From the perspective of a psychology practice manager, these study results suggest that stepped care may be less costly to deliver than face-to-face manualised therapy. It would be concerning if any cost savings realised through psychology practices would be shifted to other parts of the health care system such as hospitals. However, in our study, the group receiving stepped care spent less on medications, health care providers and hospital services, even though these differences were not significantly different from the control group. This was an important aspect of the economic evaluation and the use of administrative data was a significant strength. About 68% of participants’ parents (or participants who were greater than 14 years old) consented to the use of participant-specific data from the MBS and PBS. This provided specific dates of service for health professional visits and prescriptions as well as the specific amounts paid by government (as the third-party payer) and the out-of-pocket payments by participants’ families limiting recall bias and missing data.
While the cost of parent-reported lost productivity was not statistically different between groups, the mean was $750 lower in the stepped care group compared to the Cool Kids control group. This may support our assumption that parents would lose more time from work to accompany their child when attending face-to-face sessions. Therefore, stepped care may be particularly advantageous to parents who do not have flexible work schedules and would incur a substantial opportunity cost from work absenteeism to attend therapy with their child.
While Australians currently have access to CBT through psychologists under the government-funded Better Access initiative (Australian Government Department of Health, 2017), research has shown that nearly 40% of young people with anxiety still do not seek treatment (Spence et al., 2018). Some commonly cited barriers to accessing mental health care for young people include perceived stigma, confidentiality, a preference for self-reliance and cost (Gulliver et al., 2010; Sheffield et al., 2004). Therefore, these results provide evidence that a stepped care model can be recommended as an alternative to initial face-to-face psychology services for young people with anxiety, minimising several barriers to accessing care without compromising outcomes or increasing costs.
There are a variety of stepped care models available; however, the ideal number and nature of steps for the treatment of anxiety in youth has not been defined. The initial three-step model evaluated in this trial only included CBT, given the strength of the evidence regarding its efficacy. However, this required a resource-intensive and expert-based final step. A different form of psychological therapy or the use of medications are alternatives shown to be effective and cost-effective as the final step in stepped care treatment models for adults with anxiety and depression (Goorden et al., 2014; Ho et al., 2016). Therefore, further research into the optimal number and composition of steps for the treatment of anxious youth is required.
The results of this economic evaluation are subject to limitations. This study was conducted at a single specialist referral centre in Australia which would have a high level of socioeconomic advantage. The randomised controlled design of the study was beneficial for the internal validity of the study; however, this also led to limitations in the ability to generalise the findings. Ideally, a more naturalistic study design conducted at a number of different sites would assist in the translation of results into practice.
Some information that was collected through self-reported questionnaires such as medications and services not reimbursed through the government (i.e. hospitalisations) as well as parental lost productivity would be subject to recall bias. However, both groups in the study would be subject to similar bias and the percentage consenting to the use of MBS/PBS data was not significantly different between groups.
It is also important to note that the study was powered to detect differences in the main clinical outcome of remission from the primary diagnosis and not to detect cost differences (Rapee et al., 2017). This may explain the non-significant differences in costs. Given the data from this study, we would require approximately 600 participants per group to be able to detect a significant difference in societal costs.
There was also the potential that the cost of parental time was double-counted by estimating parental time contributing to the delivery of the intervention in addition to costing the parent-reported time lost from work. We attempted to address this issue by conducting a sensitivity analysis where the parental time required to deliver the intervention was removed from the total cost. The results were unchanged in this sensitivity analysis.
Despite these limitations, the results suggest that for young people with anxiety disorders, this three-step model of care consisting of a low-intensity self-help intervention, followed by two intensities of face-to-face CBT, provides comparable outcomes to a validated face-to-face programme. From the health sector perspective, intervention delivery and total costs were lower but not significant. It is only when we take into account parental time involved in delivering the interventions from the societal perspective that stepped care becomes less costly to deliver. Future research to evaluate various models of stepped care as a treatment for young people with anxiety compared to treatment as usual in multiple settings is recommended.
Supplemental Material
Clean_copy_Supplementary_Materials_13_11_2018 – Supplemental material for Economic evaluation of stepped care for the management of childhood anxiety disorders: Results from a randomised trial
Supplemental material, Clean_copy_Supplementary_Materials_13_11_2018 for Economic evaluation of stepped care for the management of childhood anxiety disorders: Results from a randomised trial by Mary Lou Chatterton, Ronald M Rapee, Max Catchpool, Heidi J Lyneham, Viviana Wuthrich, Jennifer L Hudson, Maria Kangas and Cathrine Mihalopoulos in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the research staff and therapists who worked on this project as well as the participants and their parents who took the time to complete the study assessments.
Availability of data and material
The data sets generated and/or analysed during this study are not publicly available due to issues of participant confidentiality but would be made available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.M.P., H.J.L., V.W. and J.L.H. developed and distributed the Cool Kids programme but receive no financial benefit. There are no other conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by National Health & Medical Research Council (grant APP1027556).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.