
Abstract
Background:
Supporting the decision-making of mental health service users fulfils professional, ethical and moral obligations of mental health practitioners. It may also aid personal recovery. Previous research on the effectiveness of supported decision-making interventions is limited.
Aims:
The study aims to explore from several perspectives the barriers and facilitators to supported decision-making in an Australian context. Supported decision-making was considered in terms of interpersonal experiences and legal supported decision-making mechanisms.
Methods:
In all, 90 narrative interviews about experiences of supported decision-making were conducted and analysed. Participants were mental health service users who reported diagnoses of schizophrenia, psychosis, bipolar disorder and severe depression; family members supporting them and mental health practitioners, including psychiatrists. The data were analysed thematically across all participants.
Results:
Negative interpersonal experiences in the mental health care system undermined involvement in decision-making for people with psychiatric diagnoses and family carers. Mental health practitioners noted their own disempowerment in service systems as barriers to good supported decision-making practices. All groups noted the influence of prevailing attitudes towards mental health service users and the associated stigma and discrimination that exist in services and the broader community. They believed that legal supported decision-making mechanisms facilitate the participation of mental health service user and their family supporters in supported decision-making.
Conclusions:
Enabling supported decision-making in clinical practice and policy can be facilitated by (1) support for good communication skills and related attitudes and practices among mental health practitioners and removing barriers to their good practice in health and social services and (2) introducing legal supported decision-making mechanisms.
Introduction
Supporting the decision-making of mental health service users (MHSUs) fulfils the professional, ethical and moral obligations of mental health practitioners and may also aid personal recovery. Supported decision-making (SDM), the process whereby individuals make decisions with the assistance of others (Hale et al., 2017), arises from legal and ethical arguments about personhood and the right personally to decide matters of importance (Pathare and Shields, 2012). SDM allows individuals ‘to give expression to their wishes and preferences regarding a particular decision’. (Gooding, 2013: 434). It aligns with personal recovery principles that emphasise hope, identity and personal responsibility (Slade et al., 2014).
The practice of SDM reflects international human rights law principles which are shaping mental health law and policy reform worldwide (McSherry and Weller, 2010). The United Nations Convention on the Rights of Persons with Disabilities (CRPD) sets out as its first guiding principle, ‘[r]espect for inherent dignity, individual autonomy including the freedom to make one’s own choices …’ (Article 3).
SDM is distinct from ‘substituted decision-making’ and ‘shared decision-making’ (Pathare and Shields, 2012). Substituted decision-making refers to one person, such as a guardian, making decisions on behalf of a MHSU. Shared decision-making generally refers to clinical practices that enable collaborative decision-making for health care decisions (Simmons and Gooding, 2017). A fundamental difference between these types of decision-making is that SDM shifts power from clinicians to MHSUs. Formal and informal mechanisms may facilitate SDM practices in mental health treatment and support services. Mental health laws in some jurisdictions promote SDM through advance statements or directives by which MHSUs outline their treatment preferences and ‘nominated persons’ schemes whereby MHSUs nominate others to advocate for them when unwell. Family members, carers and peers may provide informal support for decision-making.
There is more substantial research on shared decision-making in mental health services (Joseph-Williams et al., 2014; Shay and Lafafa, 2015; Simmons et al., 2010) than on the implications of SDM for mental health practice. In their synthesis of existing literature, Bee et al. (2015) found substantial barriers to MHSU involvement in decision-making, concluding that any involvement is commonly driven by tokenism. Although few implementation studies have been conducted, there is evidence that concerns about barriers are warranted. A systematic review found that only 20% of clinicians in mental health services (psychiatrists, nurses, psychologists, social workers and case managers) accessed advance statements; of those, only 67% of requests were followed (Nicaise et al., 2013). The same review found that while mental health clinicians gave overall endorsement of advance directives, psychiatrists were least likely to describe them as beneficial (Nicaise et al., 2013). A study of psychiatrists’ responses to a clinical vignette found that 70% would not adhere to requests in an advance statement (Sellars et al., 2017).
Recent reforms to mental health laws across Australia and New Zealand have aimed to address human rights concerns as well as assist personal recovery. This study was undertaken following reforms to mental health legislation in Victoria, Australia. It documents the experiences, views and preferences of MHSUs, family supporters and mental health practitioners (MH practitioners) about SDM, treatment and personal recovery. The study aims to explore the obstacles and facilitators to SDM in Australia.
Method
The project collected personal accounts of MHSUs, family supporters and MH practitioners (including psychiatrists) for presentation on an online resource (http://research.healthtalkaustralia.org/supported-decision-making/overview). The project was undertaken in collaboration with Healthtalk Australia (http://healthtalkaustralia.org). Ethics approval was received from Monash University (CF13/2980-2013001607).
Narrative interviews were conducted during 2014 and 2015. Eligible participants were people who self-reported as having received a diagnosis of major depression, bipolar disorder, psychosis or schizophrenia and felt sufficiently well to participate in the interview. Recruitment occurred through posters, staff contact and email networks in community mental health organisations.
Interviews lasted between 1 and 2 hours, were video- or audio-recorded with participants’ consent and held at locations chosen by participants. The interview began with an invitation to recount lived experiences of being diagnosed with mental illness and involvement in decision-making about treatment and other life decisions. Follow-up questions included (1) how participants experienced mental health services, (2) how they made decisions about treatment, (3) how they conceptualised personal recovery and (4) how they would have liked to be supported when making important decisions about their mental health and general well-being.
Recruitment of family supporters followed the same process. Eligible participants were caring for a family member who received one of the above diagnoses. Interviews lasted between 1 and 3 hours and were held at locations convenient for participants. Interviewees were asked to describe their experience of caring for a family member, including their involvement in assisting the person’s decision-making about treatment and life decisions.
MH practitioners were recruited through partner organisations, information distributed at sector events and professional associations. Interviews lasted approximately 1 hour were audio-recorded and predominantly conducted at the participant’s workplace. Participants were invited to describe their experience of working with MHSUs and family supporters. The questions focused on processes related to SDM, its impact on personal recovery, opportunities and concerns about participating in SDM and the potential role for MH practitioners in developing SDM mechanisms.
Data analysis
Interviews were transcribed and transcripts returned to participants for review. Coding frameworks were developed by the research team. Transcripts were imported into NVivo 10 software for qualitative data management and analysed thematically. The analysis used an experience-centred approach based on a socially and culturally directed research framework (Andrews et al., 2008). Team members were involved in cross-checking the analysis and identifying emergent themes. Common and divergent themes among participant groups were identified in the analysis (see Knight et al., 2018 for details).
Results
In all, 92 interviews were conducted, with two people subsequently withdrawing consent. Interviews with 29 MHSUs were analysed. Participants were mostly female, aged over 40 years and reported receiving a range of lifetime diagnoses (Table 1). Of the 29 family supporters, most were female, aged over 60 years and supported people who had experienced compulsory treatment at some time (Table 2). A total of 12 psychiatrists and 20 other MH practitioners were employed across inpatient and community mental health treatment settings, including forensic, youth and aged care (Table 3).
Characteristics of MHSU.
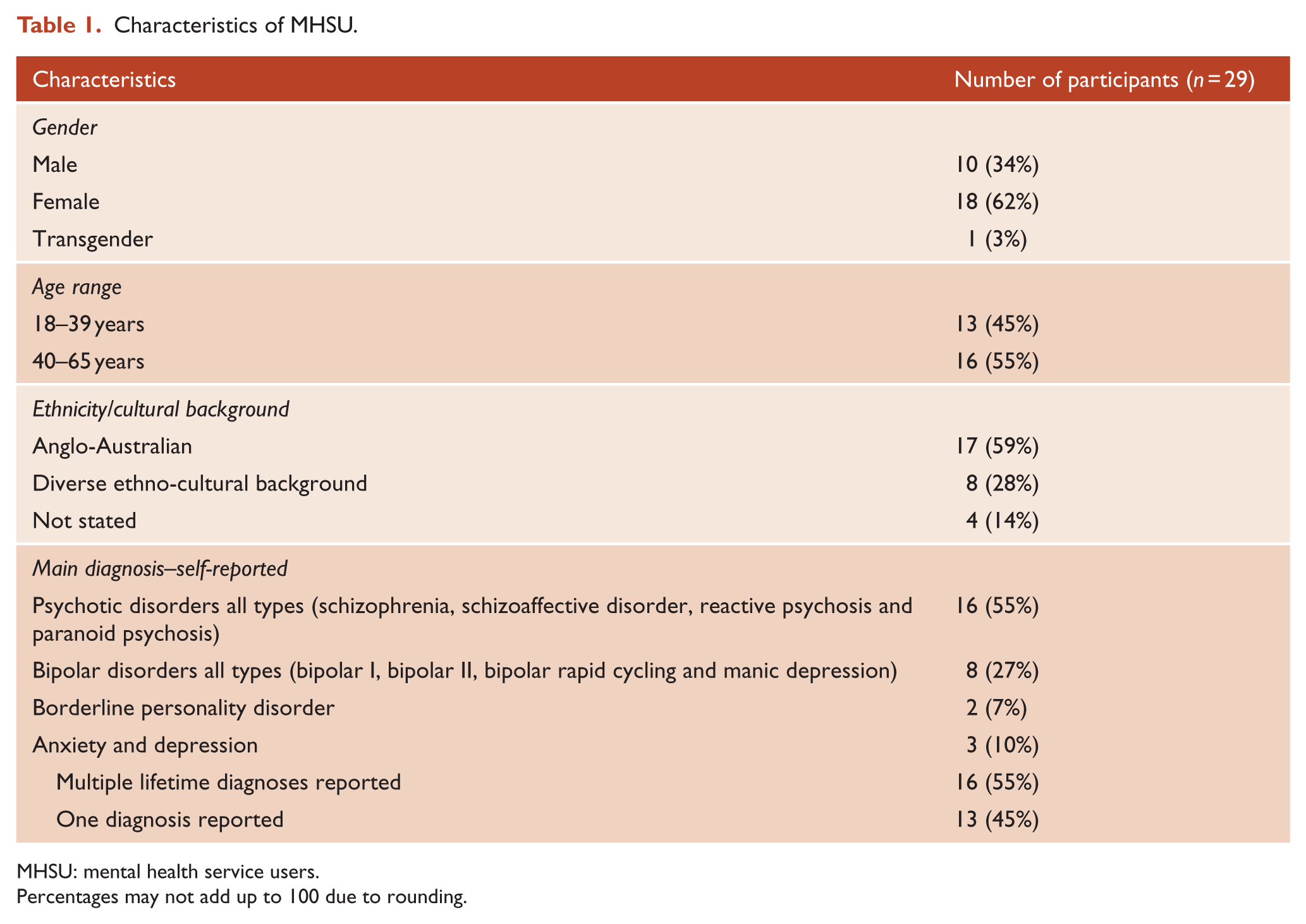
MHSU: mental health service users.
Percentages may not add up to 100 due to rounding.
Characteristics of carer participants.
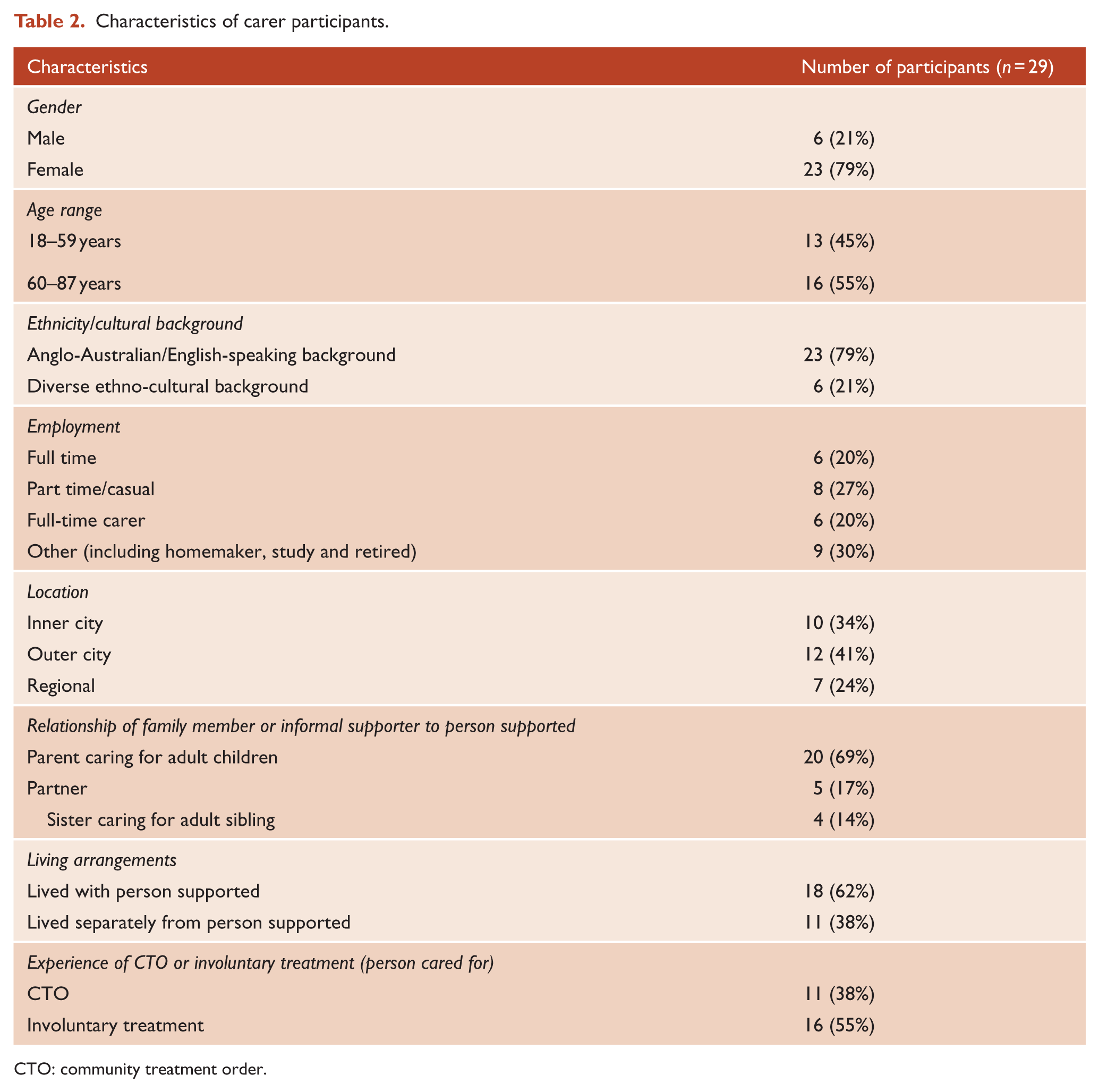
CTO: community treatment order.
Characteristics of mental health practitioner participants.
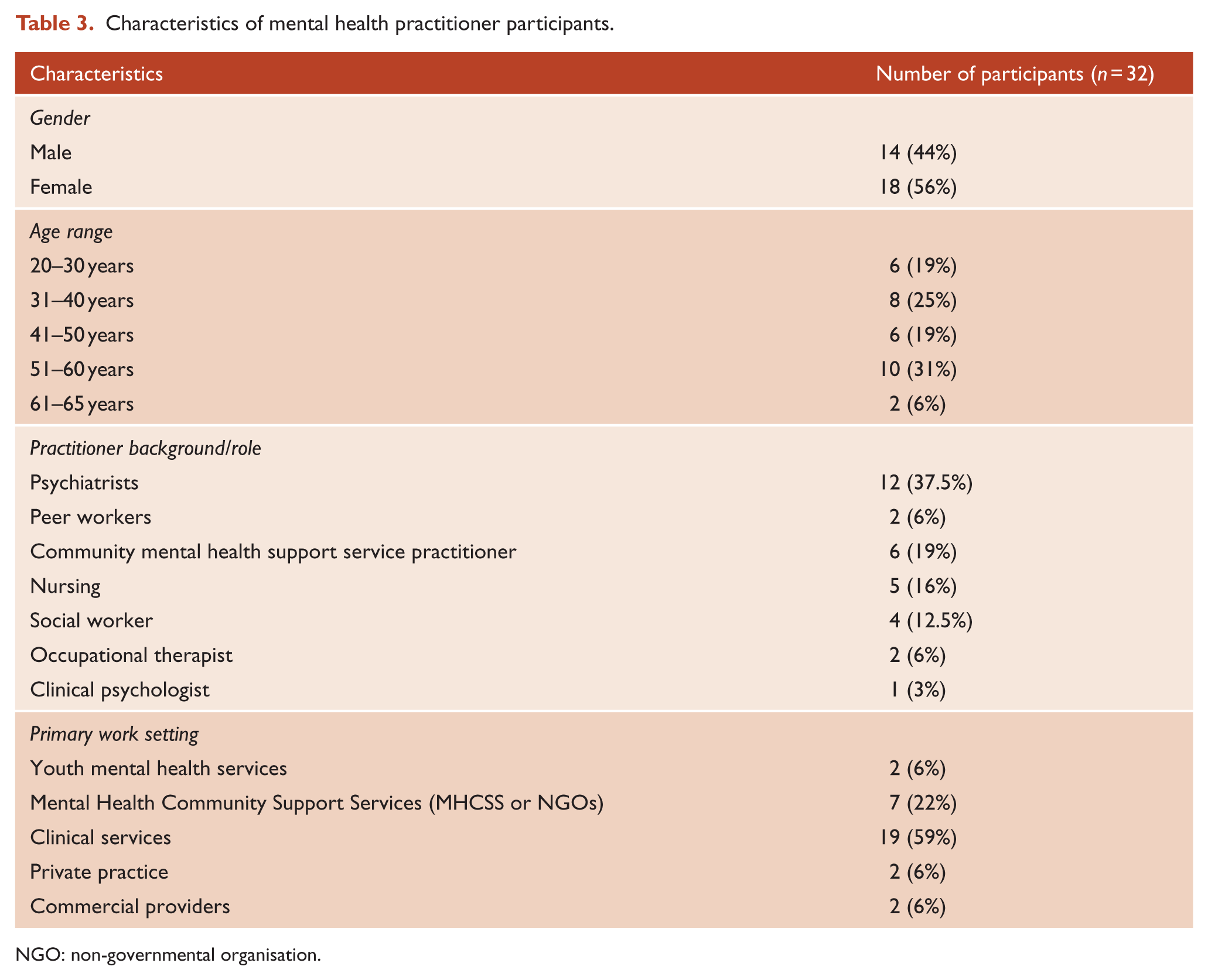
NGO: non-governmental organisation.
Views of MHSU and family supporters on SDM
Given the significant commonalities in experiences of SDM and the difficulties reported by MHSUs and family supporters, the results from both sets of interviews are presented in this section. The next section focuses on the professional experiences of MH practitioners.
MHSUs reported limited experience of SDM. Participants appreciated clinicians who demonstrated communication skills and empathy and connected this to increased decision-making capacity. When interactions with MH practitioners were perceived as impersonal, they had a negative impact on the motivation and ability to be involved in decision-making. Barriers to establishing useful relationships with clinicians included lengthy waiting times to see MH practitioners, long gaps between appointments and poor continuity of care.
Participants commented frequently on the value of the professional relationship established with general practitioners (GP) who helped them make decisions:
[My GP’s] been a fantastic advocate … he’s just been with me every step of the way … I could have had someone who was very high-handed and just wanted me in and out … just another patient, part of the numbers. I think I’m a real person with my doctor. (Joseph, 37)
Most family supporters described a good experiential knowledge of their family member’s daily life alongside inexperience at managing personal matters associated with mental health conditions. They questioned whether psychiatrists can engage productively with their patients’ or family supporters’ experience during limited and infrequent consultations:
I think [carers] know more about the illness than what a doctor does … Because [carers] see it daily and a doctor only sees the patient once a month, once every few months. (Wendy, 67)
Family supporters described feeling ‘overlooked’ and believed that clinicians did not understand or support their role in the decision-making process. Many relied on their GP to assist them negotiate the system. They recommended education and training in independence skills for MHSUs and for themselves about their rights and the SDM support they could expect from clinicians.
Legal mechanisms
MHSUs valued the opportunity for SDM through legal mechanisms. Having their daily affairs in order influenced their mental health and they perceived advance statements as reducing the anxiety associated with hospital stays:
I just heard someone mention [the advance statement] and then I followed up on it on my own … I wrote out some things and it’s not just about my medical treatment. (Allison, 36)
Some family supporters described how advance statements could enable them to act on wishes and preferences previously specified and noted that persons cared for would need to be comfortable with supporters’ involvement in discussions about treatment.
Hospital environment
MHSUs identified staff responses within hospital environments as potentially undermining SDM. Many participants experienced constrained communication with clinicians about treatment options. Emotional memories of coercion were recounted to explain why they did not currently participate in decision-making. Family supporters struggled with experiences of being ‘treated like a criminal’ when visiting hospitals. Being searched during a hospital visit left strong memories of unnecessary use of force and powerlessness:
They took [my wife] to the local psych hospital and that was my first introduction to a psych hospital … It was a pretty demeaning experience … as a carer and a husband … I felt that they were looking at me like I was [sigh] the local drug supplier that was coming in for a junkie. (Ben, 55)
Discrimination and stigma
All MHSUs described feeling ignored or judged as less capable than others. This affected their ability to make decisions about developing and maintaining close relationships. Participants were concerned about family and friends feeling disappointed if they told them about their diagnosis, treatment and experiences:
I don’t really feel that I’m able to talk to people about [my mental health]… it’s a real sense of shame that these are the things that I should be able to manage myself, and guilt about, that I’m not managing it and that I’m letting people down. (Daniel, 39)
Nearly all family supporters described ongoing exposure to discrimination experienced firsthand by the person they support, resulting in social isolation and a lack of support for dealing with complex decisions.
Views of mental health practitioners on SDM
Experience with SDM
In the interviews with mental health practitioners, it was sometimes unclear whether participants fully understood the differences between SDM and shared decision-making:
I don’t think nurses on the floor specifically get the difference between [Substitute, Shared, Supported] decision-making … they don’t feel safe with allowing someone to make a decision that could … cause them … harm. (Mental Health Nurse)
Participants identified opportunities for and benefits from SDM, including the opportunity to empower people, show them respect and expand their potential for decision-making. Many participants, particularly more junior staff, described attitudinal barriers to SDM that they found difficult to challenge. Participants identified signs of change but recognised that this requires concerted effort:
… the old system was extremely paternalistic and patronising to patients and a lot of the staff have got those embedded attitudes … there needs to be a big education of the patients and families and carers, and … the staff. (Psychiatrist)
Practices and suggestions for facilitating SDM
Participants identified structural and social barriers to MHSUs’ autonomy in the community and within services. These barriers were linked with poor understanding of mental illness:
Because we’re afraid. And that’s why people are marginalised, because it’s easier to just see them as other … than it is to see them as your brother or sister or mother or as anybody else. (Psychiatrist)
MH practitioners described numerous suggestions for improving SDM in everyday practice. They supported the use of legal and rights-based mechanisms including advance statements. Other identified enablers included interpersonal skills, support for consumer empowerment and the development of management and leadership strategies. MH practitioners recognised that building trust, engaging peer supporters, listening skills and early intervention could improve SDM:
… terms like empowerment – I think they’re meaningful, people can feel that they have greater agency … in a very important area of their life … if you think about the conditions experienced by the people that we’re mostly working with – one of the big issues for them is that they can lose hope. (Psychiatrist)
Empowering MHSUs meant supporting them to make their choices and develop or redevelop confidence through risk-taking. MH practitioners suggested that they should provide access to credible Internet-based tools and resources. MH practitioners recommended several strategies at management and leadership levels: SDM focused staff supervision and support; training and professional development; recognition and support for ‘pockets of excellence’ and resourcing and education.
Discussion
The results of this study suggest that most interviewees were in favour of MHSUs being empowered to make decisions about their treatment and care with the support of both formal and informal mechanisms. A key feature of these interviews was the emphasis placed on the importance of interpersonal skills and relationships in enabling SDM.
Participants indicated that experiences of care and treatment affect the decision-making capacity of MHSUs. Interactions that build trust are perceived as supporting confidence in decision-making, while impersonal care or structures hindering regular contact with health practitioners are seen as eroding it. Family supporters noted that regular contact with practitioners, especially GPs, who can provide guidance through mental health systems, best established trust. Family supporters’ engagement needs to extend to meaningful exchange of information and involvement in care.
MH practitioners reported being disappointed by prevailing attitudes in systems perceived as disempowering staff and MHSUs. While MH practitioners were aware of the possibilities for improvements in current systems, they pointed to an inability to change existing conditions. Several MH practitioners commented on poor understanding of the differences between substituted, shared and SDM.
All participants described stigma and discrimination as playing an important role in undermining MHSUs’ confidence about decision-making, consistent with broader experience and the literature on this topic (Thornicroft, 2006). MHSUs reported being presumed to lack the mental capacity for involvement in treatment decisions and that stigma and discrimination undermine their use of social supports. Talking through various options when able to do so, however, was perceived as helping to clarify their thoughts and preferences.
Despite frustrations about limitations in the implementation of SDM, participants identified legal mechanisms, especially advance statements and nominated persons, as offering increased opportunities. SDM implementation also needs dedicated resources and training and committed leadership. Engaging GPs, peer support workers and others who can provide continuity of care, or are seen to have high levels of trust, appears key to SDM. Here, the synchronicity with personal recovery is evident (Slade et al., 2014).
The differences between SDM and other types of decision-making need clarification. MH practitioners need training in rights-based approaches to considering risk-taking by MHSUs, to considering MHSUs’ ‘wishes and preferences’ rather than ‘best interests’ (Pathare and Shields, 2012) and for system-wide support for working in accordance with these principles. The ethical tensions and cultural challenges (Slade, 2017) for MH practitioners, MH service settings, families and society more broadly are common to shared decision-making and SDM. The evolving human rights frameworks epitomised by the CRPD, however, requires mental health organisations to engage in SDM. Although discussion about the CRPD has focused on the question of minimising coercion, the support for positive rights of MHSU, including their legal standing and agency, is essential. The CRPD may be viewed as ‘an opportunity to find new ways of ensuring voluntary access to the highest attainable standard of mental health services and community care’ (McSherry, 2015).
A strength of this study is the number of interviews undertaken. However, the study has some limitations. Although a diverse sample of people were engaged in interviews, the study did not seek to be representative and was based on participants opting in. This may result in bias in the sample. In addition, SDM is an emerging practice and participants had difficulty in drawing on current experience.
Conclusion
SDM enables MHSUs to make decisions with support from informal and formal supporters. There are several legal frameworks aimed at facilitating SDM (Davidson et al., 2016). Personal recovery and human rights frameworks provide the impetus for SDM to be implemented in mental health care and treatment (Carroll and McSherry, 2015). This can be promoted by training and support for MH practitioners in the practice of SDM and cultural changes in MH service settings.
International human rights law reinforces the need for people in MH service systems to treat each other with respect and dignity which is also central to a person-centred approach to health care (Goodrich and Cornwell, 2008). However, in this study, it was evident that the degree of autonomy people experienced varied due to stages of care and concerns about the risk of harm to self or others. No country has yet abandoned compulsory care and this is unlikely to occur. Nonetheless, the human rights framework can and needs to change in highly significant ways to comply with international law and provide adequate support for recovery: the culture of many service systems will need to change and legal systems evolve to support MH practitioners, service planners and policymakers to facilitate SDM.
Participants identified many barriers and facilitators to SDM. There was general acceptance that SDM should be facilitated through legal schemes including advance statements and nominated persons and through good practice models. Several barriers to SDM were identified including impersonal care, stigma and discrimination, an emphasis on risk rather than recovery and a lack of leadership in implementing SDM. This study highlights the need for system-level practices that address clinicians’ concerns and that reposition MHSUs as decision-makers and supporters as core to this process. Ultimately, participants were optimistic about the potential for SDM to promote recovery, but there remains a need for guidelines and training for staff, improved access to information and advocacy for MHSUs and change oriented leadership to enable SDM to be embedded into practice. There is also a need to improve the uptake of legal mechanisms such as advance statements. These initiatives all require evaluation in relation to recovery and well-being outcomes for MHSUs as well as monitoring of practice and system-level change.
Footnotes
Acknowledgements
The authors acknowledge the substantial support provided by Maureen Robinson and Healthdirect Australia, a national, government owned, not-for-profit organisation, in the development of two online resources based on this project: http://research.healthtalkaustralia.org/supported-decision-making/overview; ![]() . Finally, a special thank you must go to participants who generously shared their experiences.
. Finally, a special thank you must go to participants who generously shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This project was funded by the Australian Research Council (LP130100557) 2014–2018 and supported by partner organisations: Victorian Department of Health and Human Services, Mind Australia Limited, NEAMI National, Wellways, Tandem Carers, Victorian Mental Illness Awareness Council (VMIAC) and Healthdirect Australia. Helen Herrman is supported by an Australian National Health and Medical Research Council Practitioner Fellowship (1080820) 2015–2019.
Language Disclaimer
In writing this paper, the authors acknowledge that there are many different opinions about the respectful use of language in the context of mental health experiences and systems. Some people are quite satisfied with the kinds of words and phrases commonly used within mental health settings, while others find this language inaccurate and offensive. For the purposes of this paper, to describe the participants in the study who had received treatment from mental health services, the terms ‘people diagnosed with’ a specific mental health condition or ‘mental health service users’ are used interchangeably. Family members assisting mental health service users are described as ‘family supporters’.