
Abstract

Psychosis is a heterogeneous syndrome with a highly variable prognosis where treatment refractory and relapsing courses are all too common. We and others have been studying abnormal immunological markers in patients with first-episode psychosis. Recently, the recognition and description of autoimmune encephalitis associated with antibodies against N-methyl-
NMDAR antibody (anti-NMDAR) encephalitis
Anti-NMDAR encephalitis was initially described as a severe and fulminant neuropsychiatric syndrome, commencing with a prodrome of non-specific symptoms. Commonly, within 2 weeks, neuropsychiatric symptoms emerge and patients frequently present to psychiatrists. Seizures and abnormal involuntary movements may occur in the disease course. In the later stages, there is a rapid decrease in responsiveness with autonomic dysregulation, frequently requiring management in the intensive care setting. Diagnosis is made by testing for NMDAR antibodies in plasma and cerebrospinal fluid (CSF), as changes on electroencephalography (EEG) and magnetic resonance imaging (MRI) are often non-specific or absent. The presence of NMDAR antibodies in this clinical situation necessitates specialist medical care with screening for and removal of neoplasms when present and initiation of immunotherapy. Early diagnosis and treatment result in the most favourable prognosis for patients.
Uncertainty exists regarding the role of NMDAR antibodies in patients with psychosis
We reported a case series of seven patients (six females, one male, mean age: 26.4 years; range: 16–37 years) diagnosed and treated for anti-NMDAR encephalitis (McKeon et al., 2016). Of these, three had prolonged mental health care for psychosis, two with treatment refractory illness for approximately 6 years and one with a relapsing remitting illness with four hospitalisations and ongoing outpatient care for more than 15 years. All three had received electroconvulsive therapy at some stage and all experienced remission of psychosis but persistent cognitive deficits following immunotherapy.
We recently completed a prospective observational study in which 113 patients admitted for management of psychosis were tested for anti-neuronal antibodies. Of these, six were antibody positive, four (3.5%) with NMDAR antibodies, one (0.8%) with voltage-gated potassium channel (VGKC) antibodies and one with antibodies to an undefined antigen. Cerebrospinal fluid (CSF) examination in the five patients with antibodies to NMDAR or VGKC revealed an inflammatory process. All had remission of psychosis following administration of immunotherapy (Scott et al., 2018). Others have identified similar high rates of antibodies in patients with early psychosis. Lennox et al. (2017) reported that 9% of patients with first-episode psychosis had serum anti-neuronal antibodies although the detection of antibodies in this cohort did not influence their clinical care.
Should all patients with early psychosis be tested for anti-neuronal antibodies?
Questions continue as to which patients with psychosis should be investigated for anti-neuronal antibodies. The recent Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders (Galletly et al., 2016) and others (Lennox et al., 2017) have recommended testing patients with first episode of psychosis for anti-neuronal antibodies. The rationale for this is that early therapy for autoimmune encephalitis is associated with better outcomes.
However, universal screening of patients presenting with psychosis requires consideration. The expense for the tests is not insignificant, costing at least AUD$150 depending on the laboratory, and as with any other test, widespread use as a screening tool without due attention to the clinical presentation of the patient might lead to a substantial proportion of false-positive results and risk overlooking those who are false-negatives. Therefore, appropriate testing of patients with first-episode psychosis must consider the clinical context of the individual.
Guidelines for targeted testing of anti-neuronal antibodies in patients with early psychosis
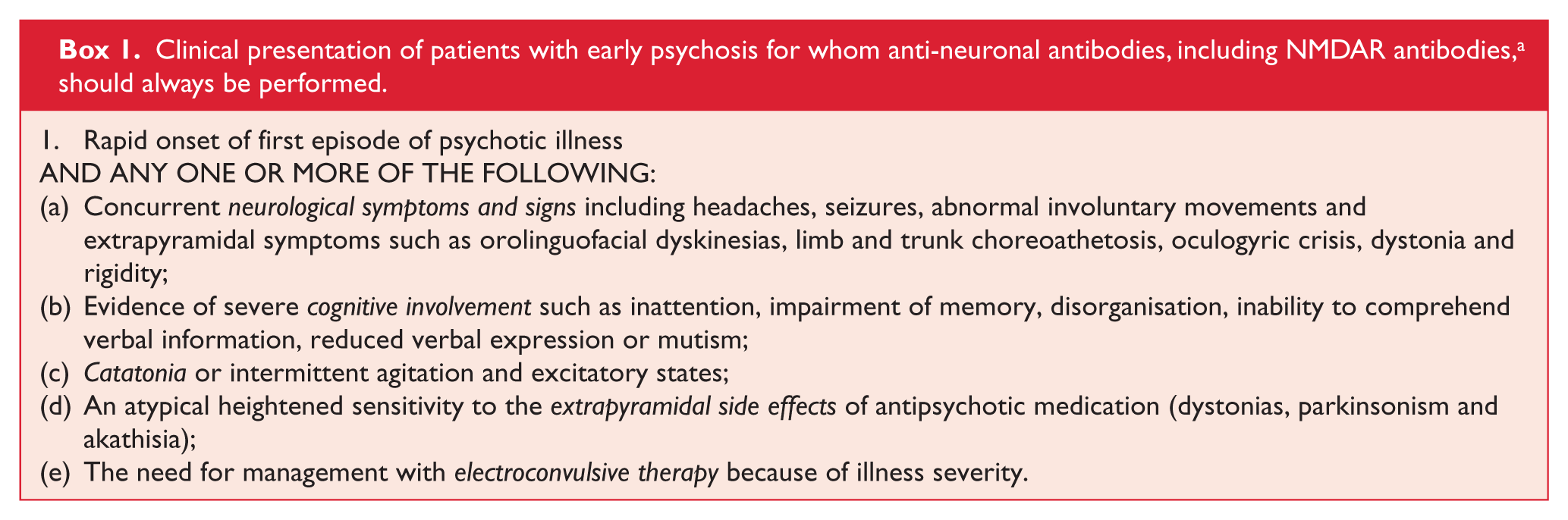
Detailed clinical descriptions of 53 patients diagnosed with anti-NMDAR encephalitis revealed 87% of patients had acute behavioural change and 74% of patients had neurological involvement, including seizures (19%), speech impairment (19%) and headache (17%) (Herken and Pruss, 2017). Consistent with this, in our experience, most patients with psychosis associated with anti-NMDAR encephalitis have a number of readily detectable clinical features which are summarised in Box 1. Where these are present, we recommend comprehensive investigation for evidence of anti-neuronal antibodies. A lumbar puncture should be considered for patients meeting these criteria, who are negative for plasma anti-neuronal antibodies and are not responding to treatment. Even with coinciding substance use, an autoimmune aetiology must be considered. In our study, one patient’s illness occurred after cannabis use and was initially attributed to this substance (Scott et al., 2018).
Clinical presentation of patients with early psychosis for whom anti-neuronal antibodies, including NMDAR antibodies, a should always be performed.
Laboratories in Australia require clinicians to specifically order N-methyl-
The suggested screening criteria are based on relatively small cohort studies and focus particularly on NMDAR antibodies. These criteria may well not be valid for other antibodies or in other populations. Further studies are needed to confirm the predictive validity of these criteria to identify all those with an autoimmune cause to their psychosis.
Conversely, there are patients whose first episode of psychosis is very unlikely to be a result of anti-NMDAR encephalitis (Box 2). Routine screening for anti-neuronal antibodies in this population, with a likely very low prevalence, might result in the false-positive rate exceeding the true-positive rate, making interpretation of the results difficult, thereby exposing patients to unnecessary investigations and wasting scarce clinical resources.
Clinical presentations of patients with early psychosis for whom investigation for anti-neuronal antibodies is not indicated.

Future directions in clinical research of anti-neuronal antibodies in psychosis
Testing for anti-neuronal antibodies in patients with schizophrenia has not been recommended, and further studies are needed to determine who should be tested. Our research has shown there are patients currently in mental health services who have anti-NMDAR encephalitis but are currently receiving standard care for psychosis. Research is needed to determine whether immunotherapy in addition to or as an alternative to antipsychotic treatment changes the long-term outcome in those patients with psychosis positive to anti-neuronal antibodies.
The diagnosis of autoimmune encephalitis is primarily based on the presence of anti-neuronal antibodies in the patient with neuropsychiatric illness, and there are few other reliable diagnostic tools. Developing synergistic, confirmatory testing, such as advanced imaging techniques to establish the presence of central nervous system (CNS) inflammation undetectable on standard MRI, would be useful in this context. The very low prevalence of this disorder and the need to intervene early mean it will be difficult to perform randomised controlled trials of immunotherapy versus usual care to establish the efficacy of immunotherapy in antibody-positive patients with psychosis. As such, research will likely depend largely on case series. Optimising the size and usefulness of these series will require combined efforts nationally or even internationally to develop databases of affected patients, which should include clinical observations, laboratory and imaging data and treatment response as a minimum.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.G.S. is affiliated with the Queensland Centre for Mental Health Research which receives core funding from Queensland Health. The studies of anti-neuronal antibodies in first-episode psychosis was funded by generous support from the RBWH Foundation and from philanthropic donations (BAP Parking and others). J.G.S. is supported by a National Health and Medical Research Council Practitioner Fellowship Grant APP1105807. A.S. is supported by a Queensland Health Junior Doctor Fellowship and a Mater Research Foundation Betty McGrath Fellowship.