
Abstract
Dear Editor
For publication,
Charles Bonnet Syndrome (CBS) is characterized by vivid visual hallucinations in patients with visual impairment. Traditionally, patients present with optical illusions marked by distortion of shape, size, motion or color, that is, altered perception of the shape and size of people and objects that appeared smaller or larger than normal. The syndrome was first described in 1955 by Todd as Alice in Wonderland syndrome. Several causes have been correlated to the emergence of illusions, including viral infections of the central nervous system, as the Epstein-Barr viral infection (Lanska and Lanska, 2013). We hereby present a case of CBS secondary to neurological varicella-zoster (VZ) infection. To the best of our knowledge, regarding VZ infection, there is only one case reported in the literature so far (Soriani et al., 1998).
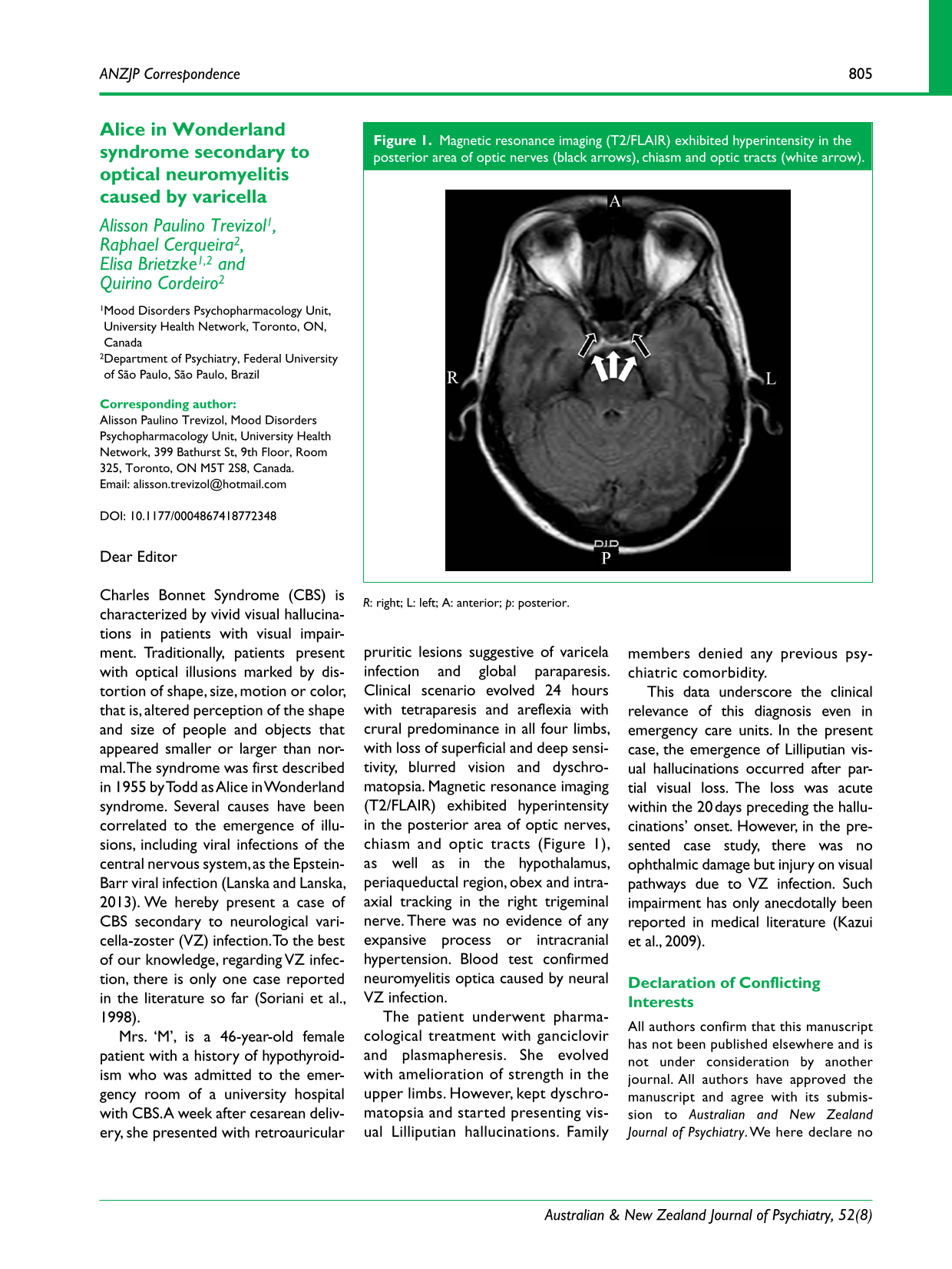
Mrs. ‘M’, is a 46-year-old female patient with a history of hypothyroidism who was admitted to the emergency room of a university hospital with CBS. A week after cesarean delivery, she presented with retroauricular pruritic lesions suggestive of varicela infection and global paraparesis. Clinical scenario evolved 24 hours with tetraparesis and areflexia with crural predominance in all four limbs, with loss of superficial and deep sensitivity, blurred vision and dyschromatopsia. Magnetic resonance imaging (T2/FLAIR) exhibited hyperintensity in the posterior area of optic nerves, chiasm and optic tracts (Figure 1), as well as in the hypothalamus, periaqueductal region, obex and intra-axial tracking in the right trigeminal nerve. There was no evidence of any expansive process or intracranial hypertension. Blood test confirmed neuromyelitis optica caused by neural VZ infection.

Magnetic resonance imaging (T2/FLAIR) exhibited hyperintensity in the posterior area of optic nerves (black arrows), chiasm and optic tracts (white arrow).
The patient underwent pharmacological treatment with ganciclovir and plasmapheresis. She evolved with amelioration of strength in the upper limbs. However, kept dyschromatopsia and started presenting visual Lilliputian hallucinations. Family members denied any previous psychiatric comorbidity.
This data underscore the clinical relevance of this diagnosis even in emergency care units. In the present case, the emergence of Lilliputian visual hallucinations occurred after partial visual loss. The loss was acute within the 20 days preceding the hallucinations’ onset. However, in the presented case study, there was no ophthalmic damage but injury on visual pathways due to VZ infection. Such impairment has only anecdotally been reported in medical literature (Kazui et al., 2009).
Footnotes
Declaration of Conflicting Interests
All authors confirm that this manuscript has not been published elsewhere and is not under consideration by another journal. All authors have approved the manuscript and agree with its submission to Australian and New Zealand Journal of Psychiatry. We here declare no conflict of interest related to the present manuscript.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.