
Abstract
Objective:
To examine (1) the 12-month prevalence of social anxiety disorder (SOC), separation anxiety disorder (SEP) and generalized anxiety disorder (GAD) in a large, nationally representative sample of Australian youth; (2) patterns of comorbidity between these disorders; (3) demographic and socio-environmental correlates and (4) the psychosocial impact and service use associated with each condition.
Method:
Data are from the 2013/2014 Australian national, face-to-face household Young Minds Matter survey of mental health and wellbeing. Informants were parents or carers reporting on 6310, 4- to 17-year-olds (55% of eligible households). The presence of each of the three anxiety disorders was determined based on the Diagnostic Interview Schedule for Children–Version IV.
Results:
In the past 12 months, 6.6% of youth had experienced at least one of SOC, SEP or GAD, with rates of 2.3% for SOC, 4.3% for SEP and 2.3% for GAD. Rates did not differ by gender but were significantly higher for SOC and GAD and lower for SEP in 12- to 17-year-olds than 4- to 11-year-olds. Comorbidity between these disorders was high, although lower for SEP. Having SOC, SEP or GAD was associated with not living with both biological parents, having a parent with a mental health problem, elevated negative family events, low carer employment and peer victimization. The association with family risk factors was greater for SEP than for SOC and GAD. Although the majority of anxious youth had received professional help, this was less likely in the younger cohort.
Conclusion:
Social, separation and generalized anxiety disorders in young people are relatively common and impairing, with a high level of comorbidity. There are both commonalities and differences in socio-environmental correlates. The majority of anxious youth received some form of professional assistance, although the rate was lower among children compared to adolescents.
The literature examining the prevalence and correlates of anxiety disorders in youth has typically focussed on anxiety disorders in general or a single-anxiety disorder. There is a paucity of research that examines such factors in different anxiety disorders within the same sample, particularly across a broad age range of young people in large, representative, community populations. Also, the majority of papers have tended to ignore the issue of comorbidity between anxiety disorders, making it difficult to determine whether results relate to a specific anxiety disorder or to anxiety in general. Furthermore, many of the studies comparing characteristics of different anxiety disorders in youth have focussed on those who have been referred for treatment and who may not necessarily be representative of those with anxiety disorders in community samples.
Large-scale, national studies of the prevalence of mental health problems provide important information to inform the planning and provision of mental health services and also to provide a baseline against which a nation can compare prevalence rates over time. A recent meta-analysis from 41 studies, 27 countries and 63,130 young people (Polanczyk et al., 2015) suggested a prevalence rate for anxiety disorders of 6.5% over the past 1–12 months. When this figure is considered in terms of the total number of youth affected in national populations, then clearly the implications are considerable. The meta-analysis did not, however, report separately on the prevalence of different types of anxiety disorders. In 2013/2014, Australia conducted the second Australian Child and Adolescent Survey of Mental Health and Wellbeing and, for the first time, included assessment of anxiety disorders with separate evaluation of social anxiety disorder (SOC), separation anxiety disorder (SEP) and generalized anxiety disorder (GAD). This enabled close examination of the prevalence, comorbidity, correlates, level of impairment and professional service use associated with these three disorders among Australian youth.
The study also provided the opportunity to examine age and gender differences in prevalence of the three specific anxiety disorders. In terms of age difference, few studies have examined the prevalence of different types of anxiety disorders from early childhood through to older adolescence in the same sample. In a review of the limited evidence available, Beesdo-Baum and Knappe (2012) concluded that SEP is more prevalent among younger children, with SOC and GAD increasing in prevalence by adolescence. We predicted that this would also be the case in the Australian sample. In terms of gender differences for specific disorders, the findings to date have been conflicting, and there are an insufficient number of studies to enable a meta-analysis (Costello et al., 2011). Some studies have reported that all anxiety disorders are more common in girls than in boys (Beesdo et al., 2009), whereas others have found minimal gender differences in early childhood, with anxiety becoming more prevalent in females in later adolescence and early adulthood (Craske, 2003). Based on this perspective, we proposed that gender effects would be more evident in adolescents (12–17 years) than children (4–11 years) across all anxiety disorders.
The data also enabled examination of patterns of comorbidity including (1) between the three anxiety disorders, (2) with other mental health problems and (3) whether such patterns differ by age and gender. To date, most studies examining comorbidity between anxiety disorders have involved clinical samples and relatively narrow age ranges and generally report a high degree of comorbidity between anxiety disorders (Verduin and Kendall, 2003). Confirmatory factor analytic studies of anxiety symptoms in the general population of youth suggest that the symptoms that characterize different anxiety disorders tend to load substantially on a higher order factor of ‘anxiety in general’, with residual variance among subsets of symptoms that relate to specific anxiety disorders (Spence, 1997). Such studies also confirm an association between anxiety symptoms and a broader internalizing factor that is also associated with depression symptoms, again with residual variance among subsets of symptoms relating to specific anxiety disorders and depression (Carragher et al., 2016). The common variance between symptoms is proposed to underlie the high level of comorbidity between anxiety disorders and with depression. Such models also suggest common risk mechanisms and vulnerabilities that may underlie continuities and discontinuities associated with different anxiety disorders (Hankin et al., 2016). On this basis, we predicted that not only would there be a high degree of comorbidity between SOC, SEP and GAD but also there would be significant associations between all three anxiety disorders and socio-demographic risk factors. However, Hankin et al. (2016) also proposed that there are particular environmental risks that are more strongly associated with particular manifestations of symptom-specific syndromes. These authors suggested that specific vulnerabilities to environmental risk come into play at different points of the life span and drive developmental changes in particular symptom clusters. They proposed that in early childhood, family stressors have a particular association with SEP, whereas in adolescence, peer issues and social rejection/exclusion have a particular association with SOC. Although this study did not permit examination of longitudinal associations, we proposed that SEP in the younger age group (4–11 years) would be more strongly associated with family stressors than is the case for other anxiety disorders, whereas peer victimization would have a stronger association with SOC during adolescence. There is good evidence that SOC in youth is associated with elevated peer victimization (Gren-Landell et al., 2011; Spence and Rapee, 2016; Stapinski et al., 2015; Tillfors et al., 2012). However, it is unclear whether peer victimization is also associated with SEP and GAD.
Information about patterns of comorbidity and differential risk factors for specific anxiety disorders at different ages has implications for the design of treatment programmes for anxiety disorder. Most current treatment programmes are ‘generic’ and assume that high levels of comorbidity indicate common underlying etiological and maintaining mechanisms that justify the use of a generic approach for the treatment of all types of anxiety disorders across childhood and adolescence (Spence et al., 2017). If comorbidity between anxiety disorders changes with age or if socio-environmental risk factors differ for different anxiety disorders, then this may influence the choice of generic versus disorder-specific intervention.
The study also provides data to inform mental health service planning in relation to the uptake of professional services for each of the three anxiety disorders at each age level. Epidemiological studies have highlighted the under-treatment of youth with anxiety disorders (Merikangas et al., 2011), but it is unclear whether this is consistent across the anxiety disorders and across age groups. There are multiple factors that influence the receipt of professional services for children with mental health problems including, for example, the duration and severity of the disorder, the degree of impairment and interference caused to family functioning (Gulliver et al., 2010). The gender of the child is also likely to play a role, with parents and teachers having different perceptions about the need for treatment for boys versus girls (Green et al., 1996). Some studies suggest that boys are more likely to be referred for mental health treatment partly because they are more likely to show externalizing problems than girls. Less is known about gender differences in the referral of those with anxiety disorders, but there is some evidence that boys with anxiety disorders may be more likely to be referred than girls because of a perception that girls are more likely to ‘grow out of’ anxiety problems (Green et al., 1996).
Based on the limited data available, we proposed that the receipt of professional help would be greater among older youth with GAD, SOC or SEP and that boys with such disorders would be more likely to receive professional help than girls. Given that referral for professional help is also likely to be influenced by the level of impairment, we also examined whether the type and severity of impairment in functioning at home and school and in relationships with friends is equivalent for GAD, SOC and SEP. Current studies have demonstrated significant impairments in these areas for anxiety problems in general (Muroff and Ross, 2011; Strauss et al., 1987) but have not compared patterns of impairment across subtypes of anxiety, nor examined whether the level of impairment influences referral practices.
Although the national survey included the diagnostic assessment of obsessive–compulsive disorder (OCD), this paper is limited to GAD, SOC and SEP. This decision was based in recent arguments presented in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013) that resulted in the exclusion of OCD from the anxiety disorders. Also, for resource reasons, the national survey did not examine the anxiety disorders of panic/agoraphobia or post-traumatic stress disorder, and diagnostic interviews for GAD, SOC and SEP were restricted to parent/carer report.
To summarize, the goals of this study were to examine (1) the 12-month prevalence of SOC, SEP and GAD in a large, nationally representative sample of Australian youth; (2) patterns of comorbidity between these disorders; (3) demographic and socio-environmental correlates and (4) type and severity of impairment in functioning and service use associated with each condition and whether these factors differed according to age group and gender of the young person. This paper also discusses the findings in relation to comparable studies internationally.
Methods
The Young Minds Matter survey was conducted during 2013–2014. Detailed information about the design, sampling and survey interview methods has been published previously (Hafekost et al., 2016; Lawrence et al., 2015). In brief, the survey first used a multi-stage, area-based sample selection procedure to select the areas for interviewing, to ensure that the sample was nationally representative in terms of economic, social and geographical characteristics. Participation of families from within the identified areas involved voluntary recruitment and informed consent of eligible households where there was at least one child aged 4–17 years. The survey also included an over-sampling of 800 16- to 17-year-olds given that this age group has traditionally shown a low participation rate and yet they are of particular interest given the increasing rates of onset of mental health problems and increasing contact with mental health services. The oversample was recruited through additional screening in approximately 50% of the areas selected in the main sample.
Where there were multiple eligible children in the household, one was selected at random. Participants in this study were 6310 parents and carers reporting on one eligible young person, reflecting a 55% response rate. Face-to-face interviews were conducted with the primary carer of the selected child in each household. Comparison with 2011 Australian Census, data showed that the sample was broadly representative of the Australian population in terms of major demographic characteristics, with no differences with respect to area-level socio-economic indicators (i.e. Socio-Economic Indexes for Areas [SEIFA]), population distribution, age, gender and country of birth of the total population of 4- to 17-year-olds in Australia and demographic characteristics including household income, family type, household tenure, parent/carer education and labour force status of families with children aged 4–17 years. There was, however, a slightly higher proportion of children aged 4–7 years and a lower proportion of families with only one eligible child than would be expected based on random sampling. Table 1 summarizes the socio-demographic characteristics of the sample.
Main demographic characteristics of the sample.
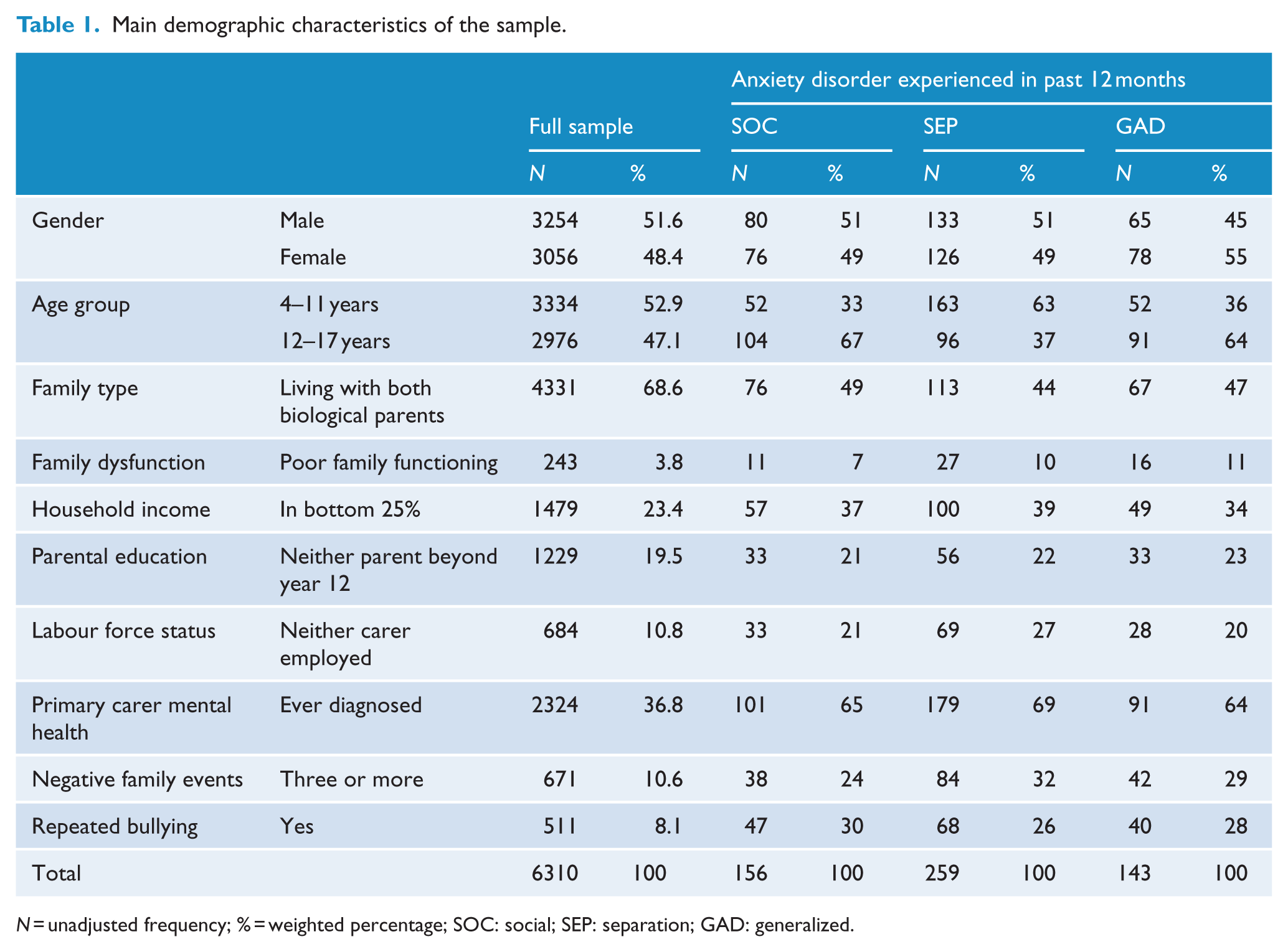
N = unadjusted frequency; % = weighted percentage; SOC: social; SEP: separation; GAD: generalized.
Ethical considerations
The research protocol was approved by the Australian Government Department of Health Human Research Ethics Committee and The University of Western Australia Human Research Ethics Committee.
Measures
Clinical diagnoses
SOC, SEP and GAD were assessed using the Diagnostic Interview Schedule for Children–Version IV (DISC-IV; Shaffer et al., 2000), aligned with the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994). In total, seven DISC-IV modules were completed by parents and carers in relation to their children’s symptoms and the impact of these over the previous 12 months: anxiety disorders (SOC, SEP and GAD and OCD), major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD) and conduct disorder (CD). In line with other national surveys that have used the DISC-IV, the criteria for impairment in this study required either severe impairment in one or more functional domains or at least moderate impairment in two or more domains. Only those who met the threshold level of symptoms and impairment criteria for diagnostic status are reported on in this paper.
Socio-environmental data included the following:
Family structure (living with both biological parents – yes/no);
Household income (lowest 25% of equivalized annual household income – yes/no); The lowest 25% of the equivalized household income is less than AUD$28,000 (~US$22,000) per annum. The equivalized income is calculated using an equivalence factor that enables comparison across families of different sizes based on the modified OECD Equivalence Scale (Hagenaars et al., 1994). The household income is divided by the weighted household size. In calculating the weighted household size, the first adult contributes 1 point, any additional adults or young people aged 14 years or over contribute 0.5 points and any children under the age of 14 years contribute 0.3 points.
Level of parent/carer education (neither carer exceeded high-school education – yes/no);
Labour force status (neither carer in full-time employment – yes/no), derived from the Australian Bureau of Statistics standard formats;
Primary carer mental health (self-report as to whether the primary carer was ever diagnosed with a mental health disorder by a doctor or other health professional);
Negative family events – primary carer report of the occurrence of each of 12 stressor events over the past 12 months that would be likely to impact on the family, such as whether a family member had experienced a serious illness; assault; injury; death of a close relative or whether they or their partner had experienced a separation, unintended loss of employment, living with a new partner, problems with police or a natural disaster. For statistical analysis purposes, elevated negative family events were defined as the experience of three or more events;
Experience of repeated bullying – assessed from primary carer report that (a) the child had been bullied, teased or picked on to the point of distress, including in person or via mobile phone, text message, Internet or email, and (b) that in the past 12 months, this had occurred with a frequency ranging from every few weeks to all the time;
Family functioning – assessed using the 6-item version of the General Functioning Scale of the McMaster Family Assessment Device (Byles et al., 1988) that has been shown to have strong psychometric properties equivalent to the original 12-item version (Boterhoven de Haan et al., 2015).
Service use: parents and carers responded to an extensive set of questions about service use received at school (or another educational institution) or from a qualified health practitioner in the previous 12 months in relation to their child’s presenting emotional or behavioural problems.
Impact on functioning: severity of the impact of mental disorders on functioning was assessed using a measure specifically developed for the study (Hafekost et al., 2016). It included 17 items adapted from Shaffer et al. (2000) and Bird et al. (2005) assessing the impact of each disorder on (a) functioning at school or in the workplace; (b) quality of relationships and participation with friends; (c) disruption to family activities and (d) the individual in terms of distress, achievements and sleep patterns. A final Graded Response Model was fitted to the item data to construct a composite score measuring severity of impact on function. The score was standardized and categorized into mild, moderate and severe impact. Psychometric and scoring details are outlined in detail in Zubrick et al. (2015).
Absence from school: carers were asked to report on the number of days that the young person had been absent from school over the school year to date. This was computed as the percentage of days absent of the year to date. For those with an anxiety disorder, carers also reported on the number of days absent from school in the past 12 months as a consequence of the anxiety problems.
Data analysis
Survey data were weighted to represent the full Australian population of 4- to 17-year-olds and to adjust for patterns in non-response, specifically the over-representation of younger children and families with more than one child aged 4–17 years and the over-sampling of 16- to 17-year-olds. Survey estimates and associated confidence intervals (CIs) were determined using STATA to account for the weighting and the clustered nature of the sample design using the method of Taylor Series Linearization (Wolter, 2007). Associations between categorical variables were examined using chi-square tests (χ²: Wald adjusted) and binary logistic regression analyses to determine odds ratios (ORs).
Results
The 12-month prevalence rates
Table 2 shows an overall 12-month prevalence of 6.6% for the experience of at least one of the three disorders, with the highest rate being for SEP (4.3%) followed by SOC (2.3%) and GAD (2.2%). Although there was no significant difference by age group for the 12-month prevalence of experiencing any one or more of the three anxiety disorders, there were significant age effects for the disorders individually, albeit in different directions. Prevalence rates were significantly higher for the 12- to 17-year-olds compared to 4- to 11-year olds for SOC (χ²(1565) = 21.67, p < 0.001) and GAD (χ²(1565) = 9.76, p = 0.002). In contrast, rates for SEP were significantly higher for the 4- to 11-year-olds compared to 12- to 17-year-olds (χ²(1565) = 7.88, p = 0.02). These age effects were evident for both boys and girls. There were no significant differences in prevalence rates between the genders for SOC, SEP or GAD for either the 4- to 11-year-olds or the 12- to 17-year-olds and no significant interactions between age and gender.
Weighted 12-month prevalence of parent-reported social, separation and generalized anxiety disorders by age group and gender.
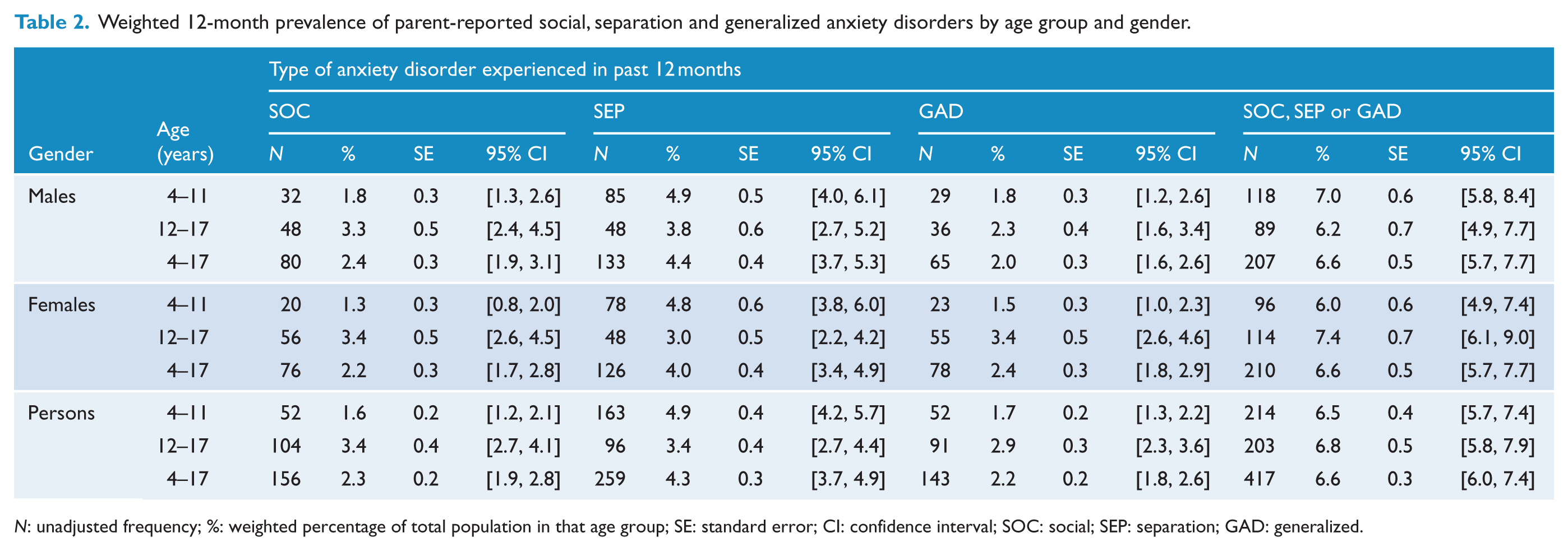
N: unadjusted frequency; %: weighted percentage of total population in that age group; SE: standard error; CI: confidence interval; SOC: social; SEP: separation; GAD: generalized.
Comorbidity between anxiety disorders
There was a high degree of comorbidity between the three anxiety disorders (see Table 3), although the data show a higher level of comorbidity for SOC and GAD than for SEP. All three anxiety disorders showed a relatively high level of comorbidity with MDD, although again this was somewhat lower for SEP and was particularly high for GAD (41.4%). There was also a moderate degree of comorbidity between each anxiety disorder and ADHD.
Comorbidity between anxiety and other disorders for the previous 12 months among 4- to 17-year-olds.
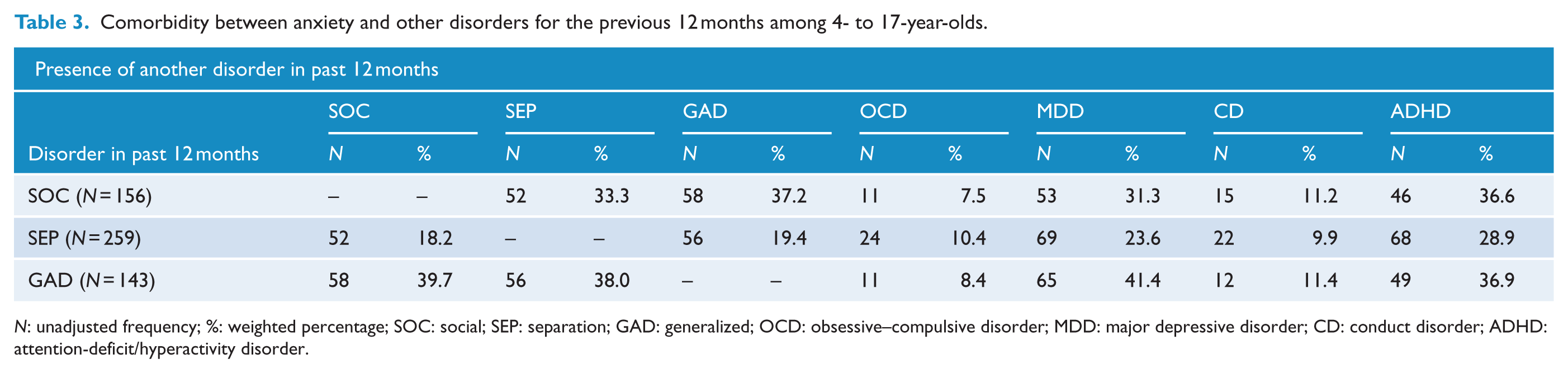
N: unadjusted frequency; %: weighted percentage; SOC: social; SEP: separation; GAD: generalized; OCD: obsessive–compulsive disorder; MDD: major depressive disorder; CD: conduct disorder; ADHD: attention-deficit/hyperactivity disorder.
We then examined whether the lower rate of comorbidity for SEP could be attributed to the lower average age of those with SEP. In keeping with this proposition, Table 4 shows that the comorbidity rates between SEP and the two other disorders were significantly lower for the 4- to 11-year-olds compared to 12- to 17-year-olds. While 11.0% of 4- to 11-year-olds with SEP also experienced SOC and 13.6% experienced comorbid GAD, 32.1% of 12- to 17-year-olds with SEP showed comorbid SOC and 30.7% showed comorbid GAD. There were no significant age differences in comorbidity for those with SOC or GAD in their profile, nor significant gender differences in comorbidity between anxiety disorders.
Comorbidity (% and ORs) for anxiety disorders by age group and gender.
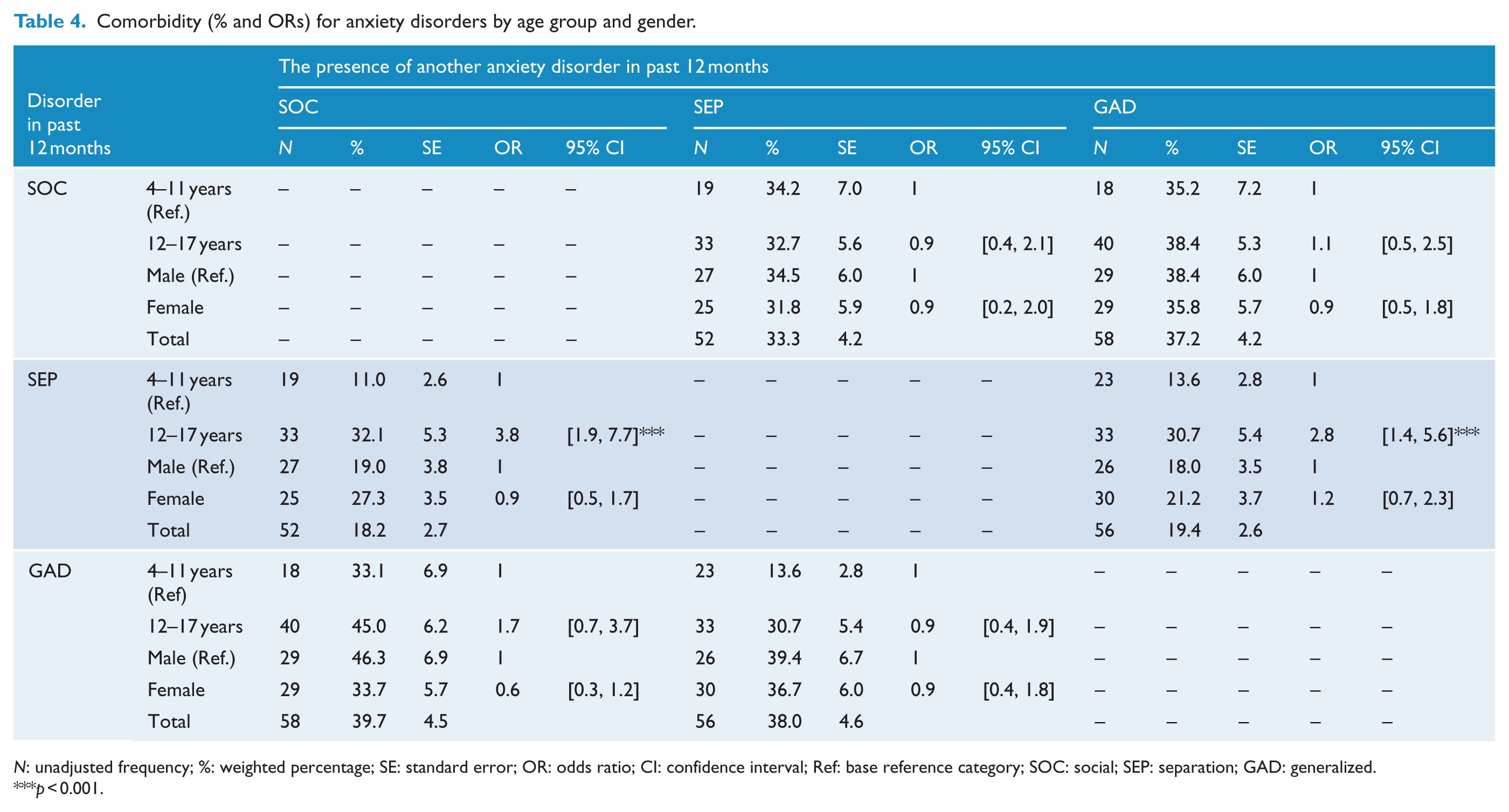
N: unadjusted frequency; %: weighted percentage; SE: standard error; OR: odds ratio; CI: confidence interval; Ref: base reference category; SOC: social; SEP: separation; GAD: generalized.
p < 0.001.
Demographic and environmental correlates of anxiety disorders
Table 5 shows that having an anxiety disorder (one or more of SOC, SEP or GAD) was associated with not living with both biological parents, family dysfunction, having a parent with a mental health problem, elevated negative family events, low carer employment, low family income (bivariate only) and the experience of repeated bullying. There was no association with age, gender or parent/carer education.
Bivariate and multivariate logistic regression analysis for demographic and life experiences in relation to experience of any one or more anxiety disorders.
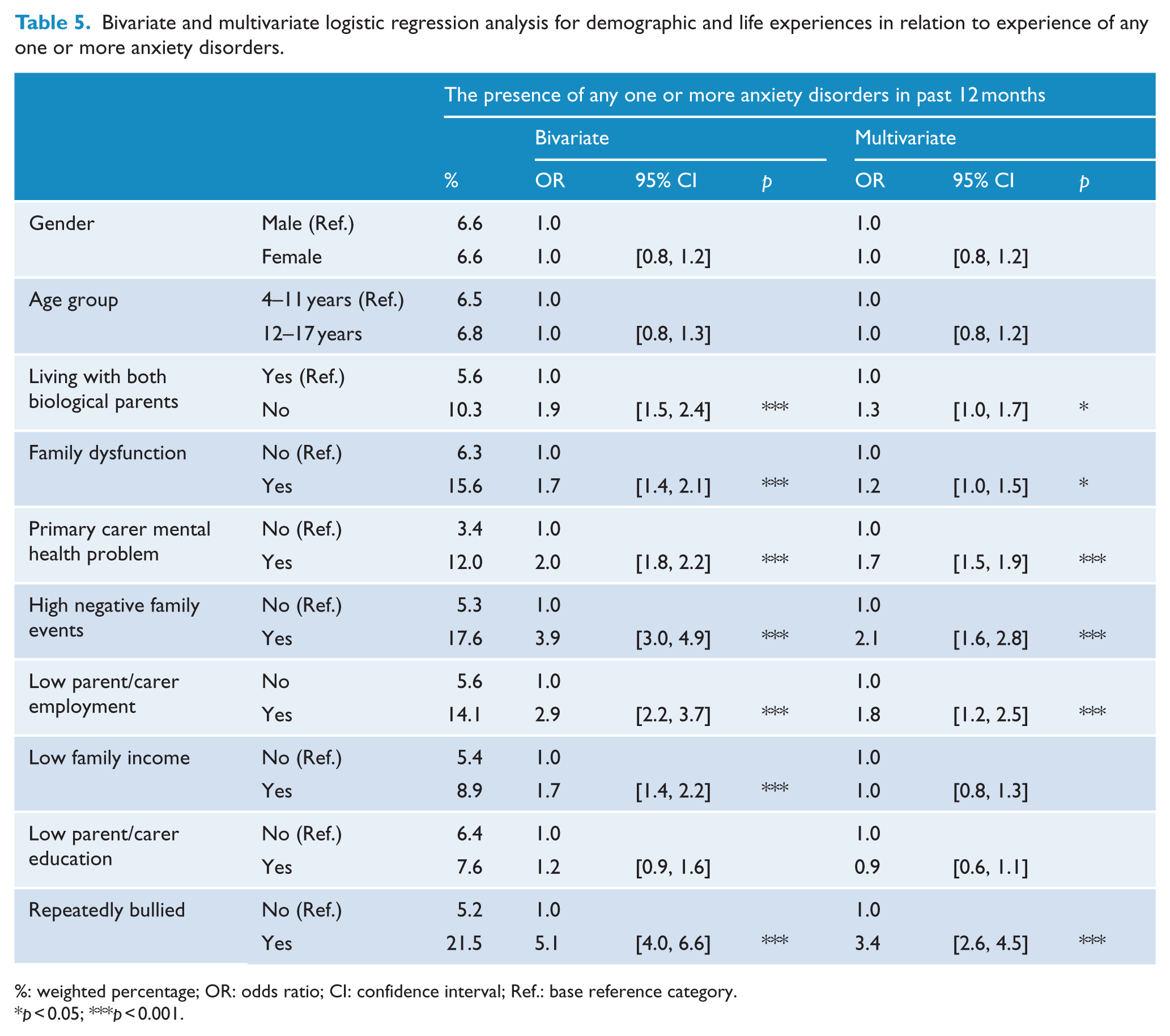
%: weighted percentage; OR: odds ratio; CI: confidence interval; Ref.: base reference category.
p < 0.05; ***p < 0.001.
When each anxiety disorder was examined individually (Table 6), the bivariate associations showed a similar pattern as reported above for the experience of any anxiety disorder, with little difference between disorders with the exception of age differences, the direction of which differed for the individual anxiety disorders. Multivariate logistic regression analyses, adjusting for age group, gender and the presence of the other two anxiety disorders, showed that SOC, SEP or GAD were all associated with having a parent with a mental health problem and repeated bullying over the previous 12 months, but multivariate associations with family dysfunction, elevated negative family events and low parent/carer workforce participation were only evident for SEP. We also examined the interaction between socio-demographic factors and age group, given the prediction peer victimization would be more strongly associated with SOC in adolescents compared to children and that family factors would be more strongly associated with SEP in children than adolescents. There was no significant interaction between age group and peer victimization in its association with any of the anxiety problems. For the interactions between family factors and age group, there was a significant association for SOC and the interaction between family negative life events and age, OR = 4.1, 95% CI: [1.2, 13.5], p = 0.021, and for SEP and the interaction between parent education and age, OR = 2.4, 95% CI: [1.1, 5.3], p = 0.036. Follow-up analyses indicated that elevated family negative life events were associated with SOC only for adolescents, OR = 2.12, 95% CI: [1.11, 4.04], p = 0.023, and low parent education was associated with SEP only for adolescents, OR = 1.97, 95% CI: [1.16, 3.34], p = 0.012.
Bivariate and multivariate (adjusting for the other anxiety disorders) logistic regression analyses for demographic and life experiences in relation to social, separation and generalized anxiety disorders.
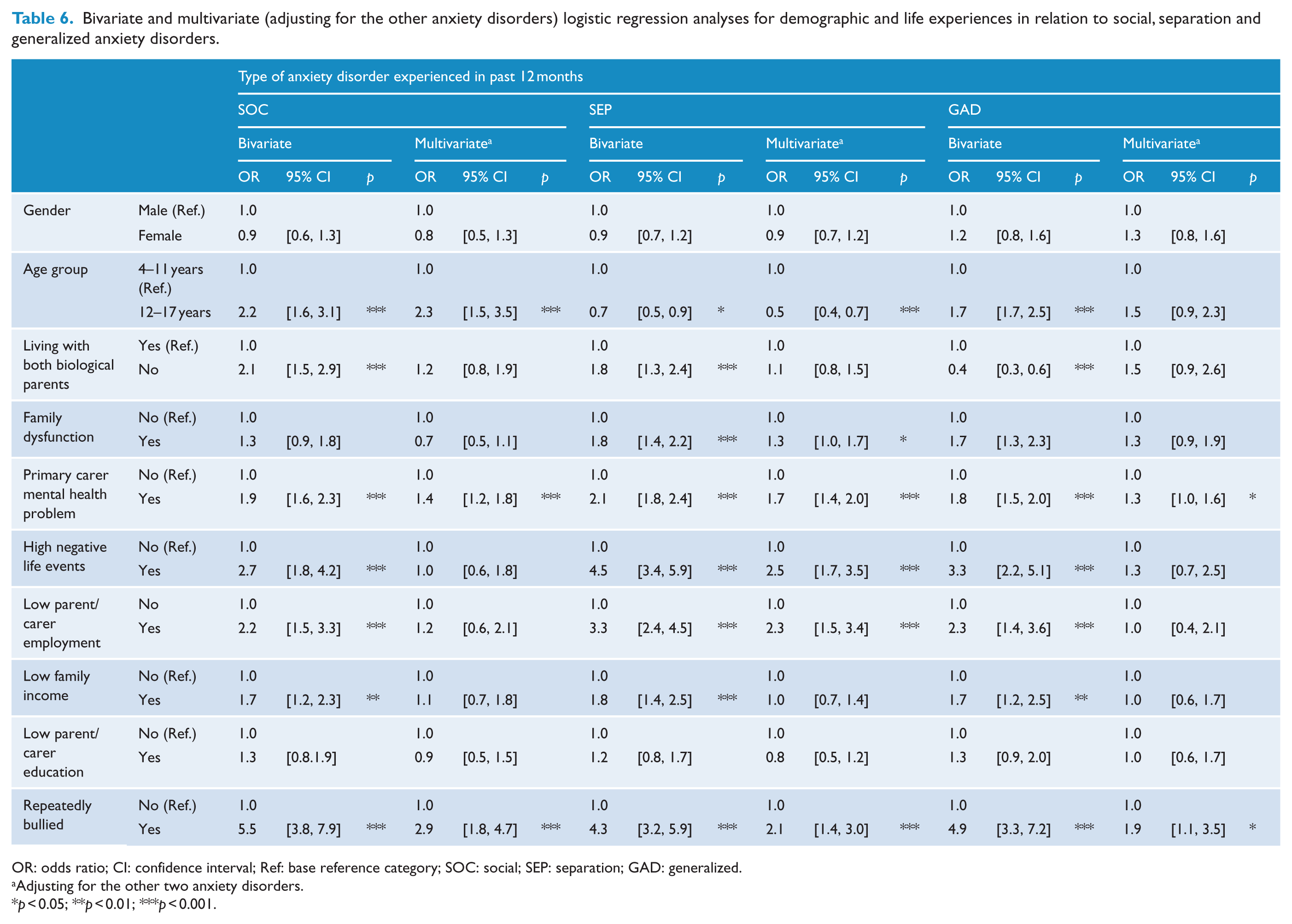
OR: odds ratio; CI: confidence interval; Ref: base reference category; SOC: social; SEP: separation; GAD: generalized.
Adjusting for the other two anxiety disorders.
p < 0.05; **p < 0.01; ***p < 0.001.
Impact on functioning and school absence
By definition, the experience of an anxiety disorder required that the young person show either severe impairment in one or more functional domains or at least moderate impairment in two or more domains. Table 7 indicates that those with comorbid anxiety were most likely to show moderate-to-severe impairment across the four domains, with youth with SEP in their profile being less likely to show moderate-to-severe impairment across these domains than those with SOC or GAD. Given that the lower level of impairment among those with SEP could reflect the younger average age of those with this disorder, we examined whether age was related to level of impairment. For those with SEP in their profile, the 12- to 17-year-olds were more likely to show moderate-to-severe impairment than the 4- to 11-year-olds in the domains of family (37.0%, standard error [SE] = 4.2% vs 54.1%, SE = 5.3), friends (31.9%, SE = 4.1% vs 69.4%, SE = 5.2) and school (30.6%, SE = 3.9% vs 64.7%, SE = 5.3); OR = 2.0, 95% CI: [1.2, 3.4], p = 0.003; OR = 4.8, 95% CI: [2.7, 8.5], p < 0.001; and OR = 4.1, 95% CI: [2.3, 7.4], p < 0.001, respectively. Thus, among the adolescents with SEP, the severity of impairment tended to be equivalent to that associated with SOC and GAD. Indeed, Table 7 shows that for both SEP and SOC, anxious adolescents showed greater levels of impairment than children, particularly in the areas of friends and school. For GAD, levels of impairment were high for both anxious children and adolescents. The proportion of youth with an anxiety disorder who showed moderate-to-severe impairment did not differ by gender for any of the disorders or areas of impairment.
Weighted percentage of youth showing moderate-to-severe impairment of functioning and high level of school absence over the previous 12 months (according to parent/carer report) by age group.
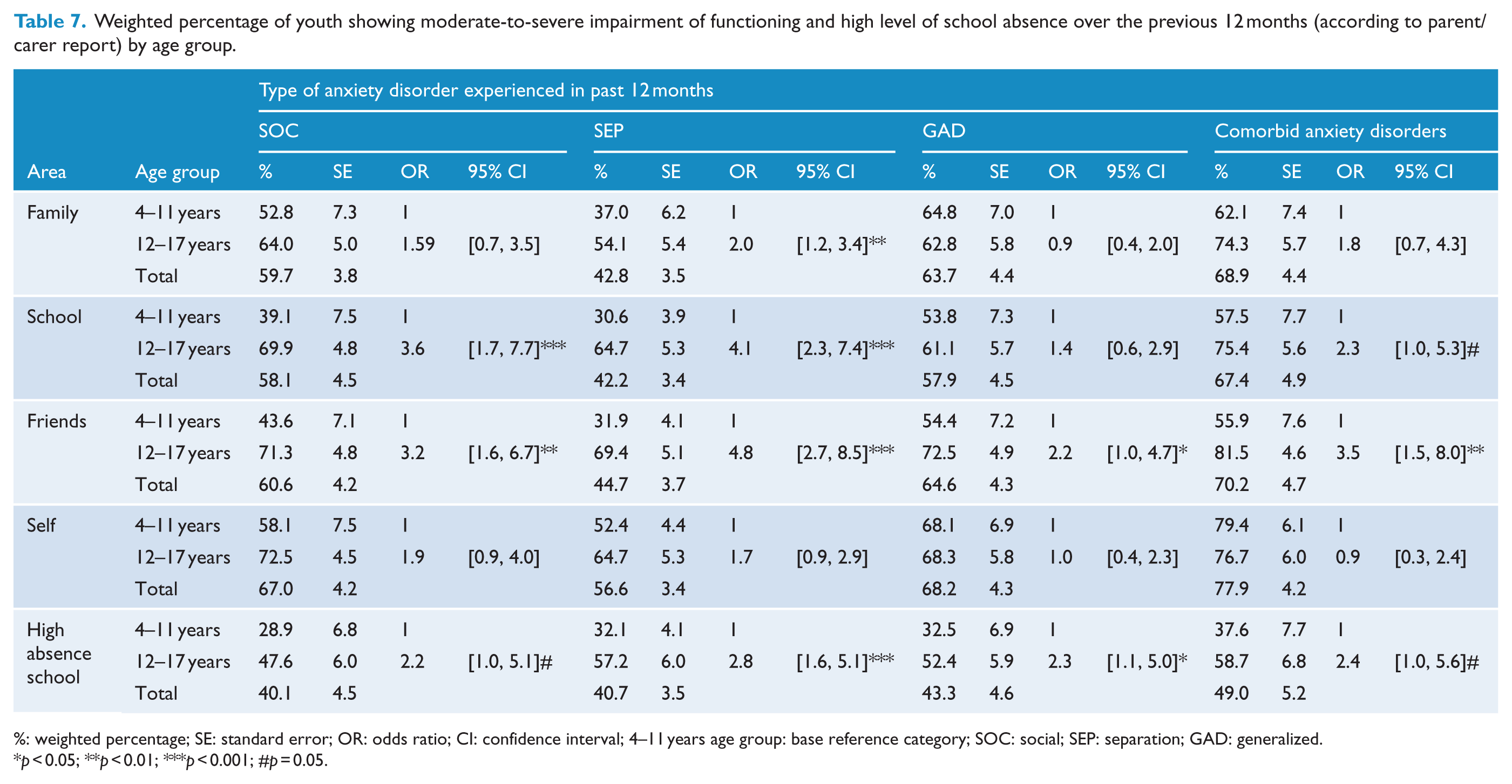
%: weighted percentage; SE: standard error; OR: odds ratio; CI: confidence interval; 4–11 years age group: base reference category; SOC: social; SEP: separation; GAD: generalized.
p < 0.05; **p < 0.01; ***p < 0.001; #p = 0.05.
In terms of absence from school, over 40% of those with an anxiety disorder showed a high rate of school absence (defined as ⩾8% of days absent in the year to date) compared to 16.4% of non-anxious peers (p < 0.001). Carers reported a mean of 6.7 days of school absence in the year to date (standard deviation [SD] = 8.6) for young people without an anxiety disorder, with a higher rate for those with an anxiety disorder (mean = 13.5, SD = 17.0 for SOC; mean = 11.5, SD = 12.7 for SEP and mean = 15.2, SD = 18.9 for GAD). Anxious adolescents were significantly more likely to show a high rate of school absence than anxious children (see Table 7).
Receipt of professional help
In total, 72.8% of those with a diagnosis of SOC, 60.7% of those with SEP and 70.9% of those with GAD had received assistance from a professional at school or a health service in the previous 12 months in relation to an emotional or behavioural problem (Table 8). The lower rate of receipt of help for those with SEP may be confounded by the younger average age of those with this disorder. Of youth with SEP in their profile, the 4- to 11-year-olds were less likely (53.1%, SE = 4.1) to have received some form of professional help than the 12- to 17-year-olds (75%, SE = 4.7); OR = 2.7, 95% CI: [1.5, 4.9], p = 0.001. Overall, youth with one or more anxiety disorders were less likely to have received some form of professional assistance if they were aged 4–11 years (52.9%, SE = 3.5) than aged 12–17 years (72.4%, SE = 3.4); OR = 2.3, 95% CI: [1.5, 3.6], p = 0.001. Child gender did not significantly influence the receipt of professional services for any of the disorders. Those with comorbid anxiety problems (79.9%, SE = 3.9) were significantly more likely to have received some form of professional help in the past 12 months than those with a single-anxiety diagnosis (54.5%, SE = 3.1); OR = 1.8, 95% CI: [1.4, 2.4], p < 0.001. Receipt of professional help was also more likely to have occurred for anxious youth who showed greater impairment in functioning. Youth with one or more anxiety disorders who showed moderate-to-high impairment in three or four of the four domains were significantly more likely to have received some form of professional help (87.0%, SE = 3.0) than youth with impairment in two or less of the four domains (46.7%, SE = 3.1); OR = 7.65, 95% CI: [4.3, 13.6]. We also examined the proportion of anxious youth who received assistance over the past 12 months for their mental health problem if the criteria were restricted to mental health professionals (including individual or group counselling from a school counsellor, psychiatrist, psychologist, social worker or family therapist) and excluded services from the school nurse, placement in a special class or school and general practitioners (GPs). This analysis indicated that the proportion of youth with an anxiety disorder receiving assistance from a mental health professional (55.9%) was only slightly lower than figure shown for ‘any health or educational service’ (see Table 8). This suggests that the majority of health and school services received had involved a mental health professional.
Weighted percentage of youth in receipt of professional assistance related to anxiety disorder(s) over the previous 12 months (according to parent/carer report).
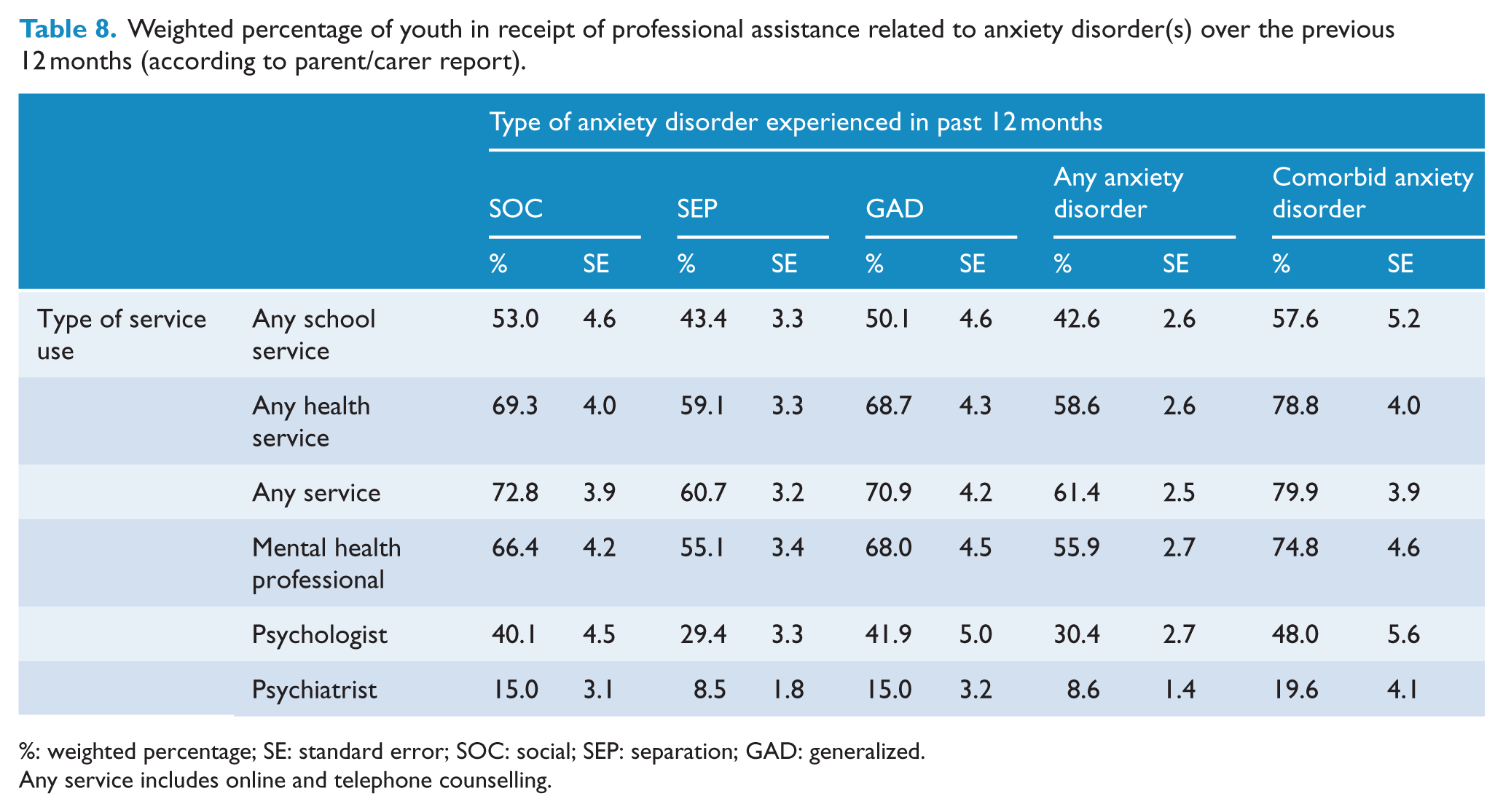
%: weighted percentage; SE: standard error; SOC: social; SEP: separation; GAD: generalized.
Any service includes online and telephone counselling.
Discussion
This study, based on parent/carer report, found a 12-month prevalence rate of 6.6% for the experience of at least one anxiety disorder (SOC, SEP and/or GAD) in a large, nationally representative sample of 4- to 17-year-old Australians. This figure is consistent with a recent meta-analysis reported by Polanczyk et al. (2015) that estimated a prevalence rate of 6.5% (95% CI: [4.7, 9.1]) over the past 1–12 months in 4- to 18-year-olds. The finding is also consistent with the 12-month prevalence rate of 6.9% reported by Roberts et al. (2007) in a large sample of adolescents in the United States and 6.9% reported by Canino et al. (2004) among 4- to 17-year-olds in Puerto Rico. Both studies used the DISC-IV. Although estimates for the prevalence of anxiety disorders have varied widely according to the methodology used (Costello, 2015), the figure reported in this study appears to be consistent with other large-scale epidemiological studies using the DISC-IV and with the recent meta-analysis noted above (Polanczyk et al., 2015). The data presented here emphasize the relatively high prevalence of anxiety disorders in young people, all of whom are experiencing significant distress and impairment to functioning.
In terms of the individual anxiety disorders, the prevalence rates in this study were SOC (2.3%), SEP (4.3%) and GAD (2.2%). These rates differ somewhat from those reported for the US National Comorbidity Survey Replication-Adolescent (NCS-A) study that reported 12-month prevalence rates of 8.2% for SOC, 1.6% for SEP and 1.1% for GAD (Kessler et al., 2012). The discrepancies may reflect methodological differences as the Kessler et al.’s (2012) study was limited to 13- to 17-year-olds and used the World Health Organization (WHO) Composite International Diagnostic Interview (Merikangas et al., 2010b) rather than the DISC and adolescents rather than parents as informants. Also, the particularly high rate for SOC found in that study is inconsistent with other studies that have reported lower 12-month prevalence estimates for SOC, more in keeping with the present study (Canino et al., 2004; Gren-Landell et al., 2009; Ranta et al., 2009).
Consistent with predictions, this study noted differences in prevalence rates by age group for each of the three anxiety disorders, being higher for SOC and GAD in the 12- to 17-year-olds, but higher for SEP in the 4- to 11-year-olds. Contrary to expectations, no significant gender differences were found in the prevalence of any of the anxiety disorders for either the younger or older age groups. It had been expected that while gender effects may not be evident in the younger age group, anxiety disorders would be more prevalent in females during adolescence (Craske, 2003). While the absence of a gender difference in prevalence of anxiety disorders in this study contrasts with some studies that found significantly higher prevalence rates in teenage girls than boys for all three anxiety disorders (Canino et al., 2004; Kessler et al., 2012), no difference between genders was found for anxiety disorders in a large epidemiological study in the United Kingdom with 5- to 15-year-olds (Ford et al., 2003) nor in the Great Smoky Mountains Study with from age 9 to 26 years (Copeland et al., 2014) nor the US National Health and Nutrition Examination Survey (Merikangas et al., 2010a). It is unclear why the findings have differed across studies. The use of parents rather than youths as the informant may be a factor, but some studies that also failed to find gender effects used combined parent–youth report (Copeland et al., 2014; Ford et al., 2003) or youth report alone (Merikangas et al., 2010a); thus, the issue is unclear. In the future, with the conduct of more studies, it may be possible to use meta-analytical methods to determine the impact of informant and other methodological factors on gender differences in anxiety disorder prevalence.
In terms of comorbidity, there was a high level of co-occurrence of the experience of SOC, SEP and GAD but also strong comorbidity between these anxiety disorders and MDD and ADHD. There were, however, differences in comorbidity patterns for the three anxiety disorders. The finding of a lower rate of comorbidity for SEP could potentially reflect an age effect, as SEP tended to be more prevalent in the younger age group, and generally, comorbidity tended to be lower in 4- to 11-year-olds than in the older age group. For the older youth with SEP, comorbidity rates were similar to those for other anxiety disorders. Possibly, anxiety problems are more specific earlier in childhood, with symptoms becoming more generalized with increasing age, resulting in greater comorbidity with other disorders. Indeed, Beesdo et al. (2009) in an empirical review concluded that the number of ‘pure’ disorder anxiety cases decreases with age in favour of patterns with multiple anxiety disorders by late adolescence or early adulthood.
When environmental correlates were examined, there were both consistencies and differences in their association with the three anxiety disorders. Young people with an anxiety disorder were more likely than youth without any of these conditions to live apart from a biological parent; to live in a family with a parent with a mental health problem, elevated negative family events, low family income and low parent–carer workforce participation and to have experienced repeated bullying in the previous 12 months. These factors continue to be significant (other than low family income) in multivariate analyses adjusting for age and gender. The pattern of results differed for the individual anxiety disorders when adjusting for the experience of the other two anxiety disorders, with a diagnosis of SEP having the strongest unique associations with the family risk factors. This finding was consistent with our prediction, based on the proposition of Hankin et al. (2016), that an adverse family environment has its greatest impact in early childhood when disorders such as SEP tend to have their onset. Consistent with this view, the results indicated that although living with a parent/carer with a diagnosed mental health problem was associated with increased risk of experiencing SOC, SEP and/or GAD, this effect was stronger for the younger compared to older age group (although it was still a risk factor in the older age group).
A striking finding was the strong association between the experience of repeated bullying and all three anxiety disorders. We had proposed that peer victimization would be most highly associated with SOC, in line with the theoretical position of Hankin et al. (2016) and that the association would be stronger in adolescents than children. However, the experience of peer victimization was linked to each of the three anxiety disorders, even when SOC was controlled in analyses for SEP and GAD, and the effects were equivalent across age groups. Although we cannot draw conclusions about directions of causality, the findings are consistent with studies that show the adverse impact of peer victimization on the development of internalizing problems in children and adolescents (Stapinski et al., 2015; Tillfors et al., 2012; Zwierzynska et al., 2013). The present findings suggest that contrary to our predictions, such an impact not only spans the anxiety disorders but also spans childhood and adolescence.
In terms of impairment associated with anxiety disorders, the findings suggest a greater adverse effect with increasing age, particularly for functioning at school and with friends, and a higher level of impairment associated with GAD and SOC than SEP. Impairment tended to be greater for those with comorbid anxiety disorders. Those with an anxiety disorder were also more likely to show a high rate of absence from school than youth without an anxiety disorder, and again, this was greater for adolescents than children.
When we examined the receipt of professional assistance, around 61% of those with at least one of the three anxiety disorders had received some form of professional assistance over the past 12 months, with around 56% receiving help from a mental health professional. Furthermore, 30% of those with SOC, SEP and/or GAD had received help from a psychologist and around 9% from a psychiatrist. These findings suggest a much higher rate of professional help than has generally been reported in the literature. For example, Essau et al. (2000) reported that only 18.2% of adolescents with an anxiety disorder had received professional help, and a later review of the literature suggested an even lower rate of assistance for anxious young people (Essau and Ollendick, 2012). However, most of the studies examined in the review were conducted prior to 2000, and a more recent large-scale survey in the United States found that 40.1% of adolescents with an anxiety disorder had received some form of professional help, with 22.3% from a mental health specialist (Costello et al., 2014). This more recent finding is more consistent with the results of this study. It is possible that over the past decade, there has been an increased awareness of anxiety disorders and their long-term adverse impact if left untreated, resulting in a greater likelihood that anxious young people will be referred for professional help. Unfortunately, it is not possible to compare the findings of the most recent Australian study with its predecessor (Sawyer et al., 2000) as that survey did not include the assessment of anxiety disorders.
In terms of factors associated with receipt of professional help, youth were more likely to have received assistance if they were in the older age group, had a comorbid rather than single-anxiety problem, exhibited greater impairment or presented with SOC or GAD in their profile (rather than SEP). However, gender was not associated with the receipt of professional help.
Although the study has many strengths, it is important to recognize its limitations. For example, the interviews did not address all anxiety disorders, such as panic/agoraphobia or specific phobias, thereby limiting the conclusions that can be drawn about these types of problems. Furthermore, the interviews did not examine lifetime occurrence of disorders, thus preventing our examination of age of onset. The response rate of 55% of eligible households was also an issue, as we cannot discount the possibility of bias in the sample despite the rigorous attempts to survey a representative sample of the population.
A further limitation concerns the use of parent/carer rather than youth report. Some prior epidemiological studies have used parent report for the child age group and combined parent and youth report for assessing diagnoses and correlates among the adolescents (Canino et al., 2004; Ford et al., 2003). The authors of these studies argued that adolescents are in a strong position to report on their mental health, whereas children are not. However, in order to avoid the confound of differential informants for diagnoses in the different age groups and to reduce the interview burden on the adolescents (and survey costs), the study restricted data collection for the anxiety modules to parent report. Ideally, future national youth surveys should include parent and youth evaluation of anxiety disorders.
This study also did not consider sub-threshold anxiety, and yet the main report from this national survey indicated significant distress and interference in daily living for young people with anxiety symptoms but who fell short of diagnostic criteria (Lawrence et al., 2015), consistent with findings elsewhere in the literature (Balázs et al., 2013). It is important that this neglected group of young people are not forgotten as they may benefit from targeted prevention to prevent development to a full-blown disorder.
Conclusion
This study confirmed, among a large, representative, Australian community sample, the relatively high prevalence of SOC, SEP and GAD during childhood and adolescence for both males and females, accompanied by significant impairment in functioning across multiple domains and a high rate of use of services from school and health sectors. Clearly, these disorders are a major issue in terms of personal distress to children and families and the cost of providing services.
All disorders showed a high level of comorbidity, although this was lower for SEP. Although there was a high degree of commonality between the three anxiety disorders in terms of the socio-environmental factors with which they were associated (such as peer victimization and living with a parent with a mental health problem), there were also differences. In particular, family factors such as family dysfunction, negative family life events and low carer employment were more strongly associated with SEP than for SOC or GAD. The findings reinforce the need for continued and enhanced provision of services for the treatment of anxious youth and for further development and evaluation of prevention and early intervention initiatives targeted at modifying family and individual risk factors for child and adolescent anxiety disorders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Professor Zubrick is supported by a Centre of Excellence grant from the Australian Research Council (CE40100027).